Jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Here is a comprehensive overview of jaundice from multiple authoritative medical textbooks.
Jaundice (Icterus)
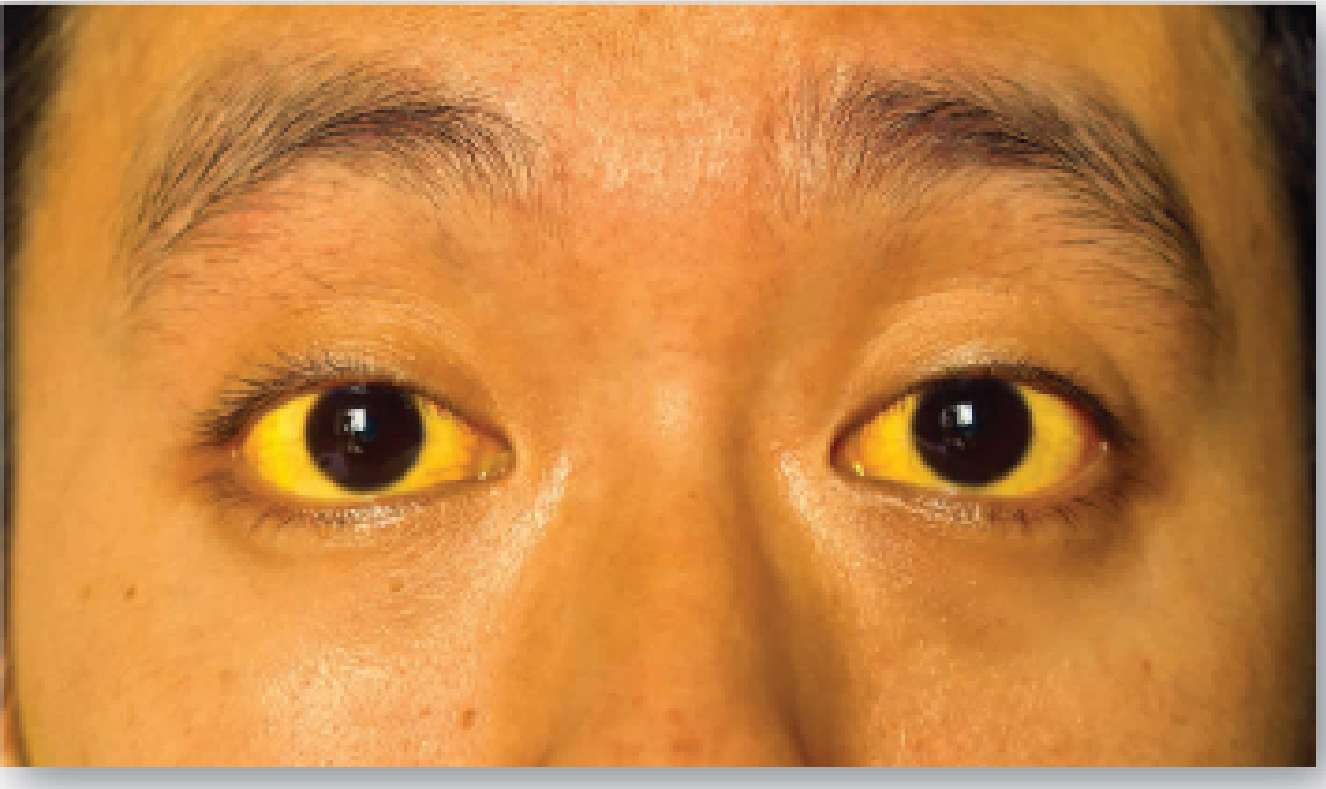
Jaundice: Icteric sclerae in a patient with hyperbilirubinemia - Lippincott's Biochemistry
Definition
Jaundice (icterus) is the yellow discoloration of the skin, sclera, nail beds, and mucous membranes caused by deposition of bilirubin, secondary to elevated serum bilirubin (hyperbilirubinemia). It becomes clinically visible when serum bilirubin rises above 2 to 3 mg/dL (normal: ≤1 mg/dL). Although not a disease itself, it is a symptom of an underlying disorder and may indicate a serious condition requiring systematic workup. - Lippincott Illustrated Reviews: Biochemistry, 8th ed, p. 799
Bilirubin Metabolism (Normal Physiology)
Understanding jaundice requires knowledge of normal bilirubin handling:
-
Formation: ~85% of bilirubin comes from breakdown of senescent RBCs (lifespan ~120 days) by the mononuclear phagocyte system. Heme oxygenase opens the porphyrin ring, converting heme → biliverdin (green) → bilirubin (red-orange).
-
Transport to liver: Bilirubin is water-insoluble (unconjugated bilirubin, UCB), so it is transported in plasma bound to albumin. It enters hepatocytes via facilitated diffusion and binds to ligandin.
-
Conjugation: In hepatocytes, bilirubin UDP-glucuronosyltransferase (UGT) adds 2 glucuronic acid molecules to form bilirubin diglucuronide (conjugated bilirubin, CB) - making it water-soluble.
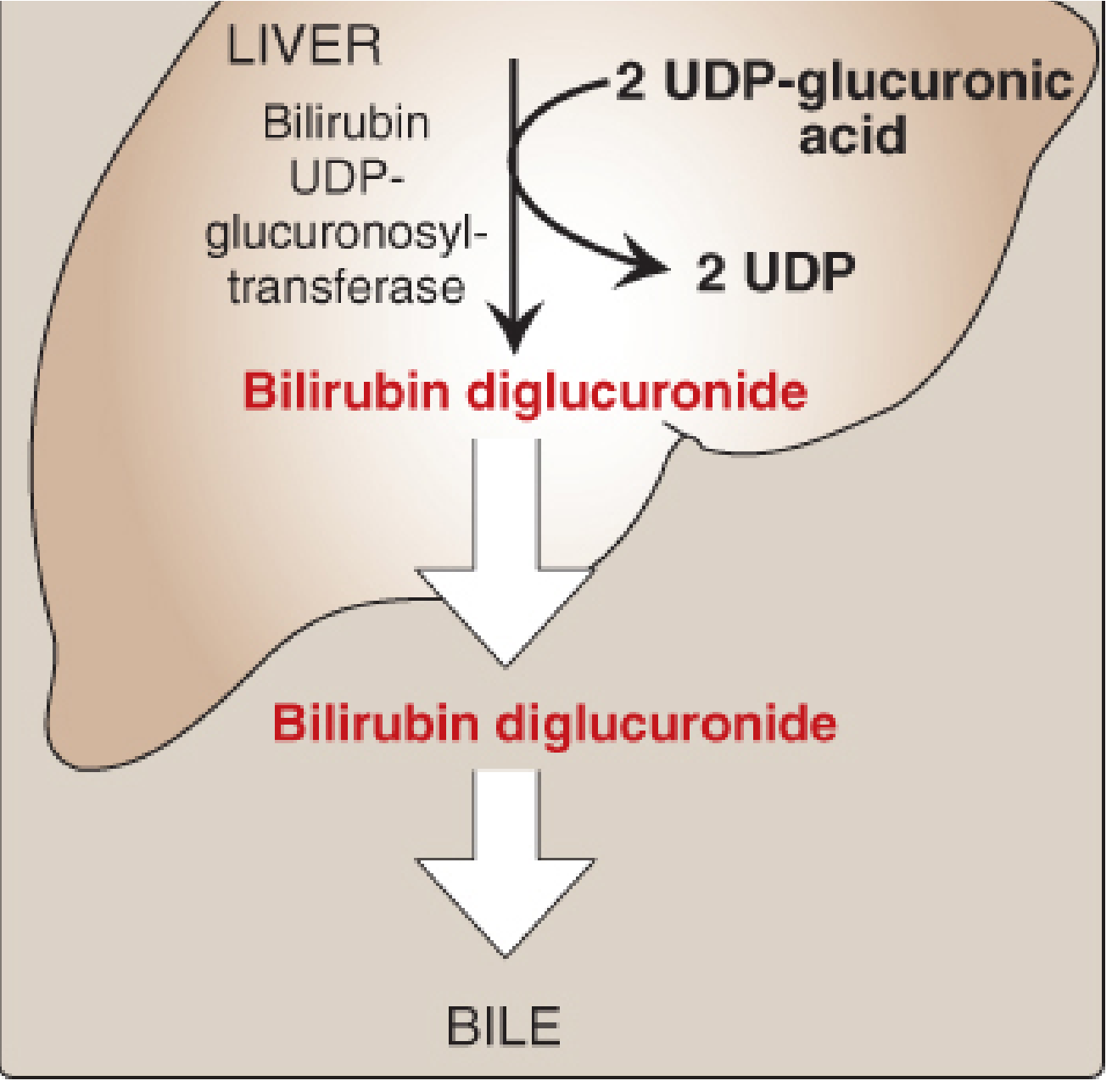
Conjugation of bilirubin in the liver - Lippincott's Biochemistry
-
Secretion into bile: CB is actively transported into bile canaliculi (rate-limiting step; impaired in liver disease).
-
Intestinal metabolism: Gut bacteria reduce CB → urobilinogen (colorless) → stercobilin (brown, gives feces its color). Some urobilinogen is reabsorbed, recycled enterohepatic, and a fraction excreted by kidneys as urobilin (yellow urine color).
- Lippincott Illustrated Reviews: Biochemistry, 8th ed, pp. 794-798
Classification of Jaundice
Jaundice is classified by the site of metabolic defect into three major types:
1. Prehepatic (Hemolytic) Jaundice
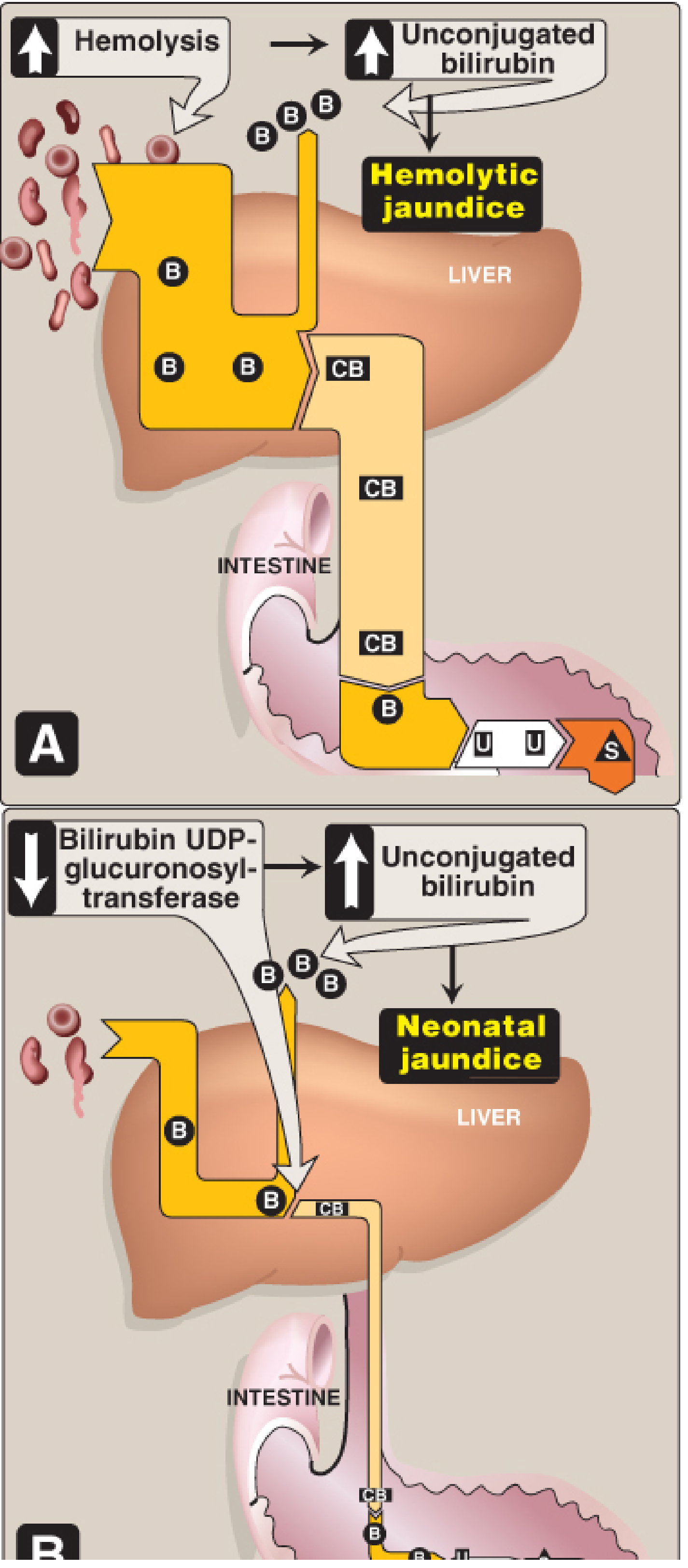
Hemolytic jaundice (A) and Neonatal jaundice (B) - Lippincott's Biochemistry
-
Mechanism: Excessive RBC breakdown overwhelms the liver's conjugation capacity (normal liver can conjugate >3,000 mg/day vs. normal production of ~300 mg/day).
-
Bilirubin type: Predominantly unconjugated (indirect) hyperbilirubinemia
-
Urine: Urobilinogen elevated; no bilirubin in urine (UCB not filtered by kidney)
-
Stool: Dark (increased stercobilin)
-
Causes:
- Hereditary hemolytic anemias (sickle cell, thalassemia, hereditary spherocytosis, G6PD deficiency)
- Acquired hemolytic anemias: immune-mediated (autoimmune, drug-induced, positive Coombs test) and non-immune (mechanical valve hemolysis, microangiopathy, infections, toxins)
- Reduced albumin (malnutrition, burns) - impairs UCB transport
-
Schwartz's Principles of Surgery, 11th ed, p. 1381
2. Intrahepatic (Hepatocellular) Jaundice
-
Mechanism: Damage to hepatocytes impairs both conjugation and excretion of bilirubin. Intrahepatic cholestasis causes regurgitation of CB back into blood.
-
Bilirubin type: Both unconjugated and conjugated elevated
-
Urine: Dark (bilirubinuria present); increased urobilinogen
-
Stool: Pale/clay-colored (decreased stercobilin)
-
LFTs: Elevated ALT and AST
-
Causes:
- Hepatitis (viral, alcoholic, autoimmune)
- Cirrhosis
- Ischemic hepatitis
- Inherited disorders:
- Gilbert's syndrome: Reduced UGT activity → mild unconjugated hyperbilirubinemia triggered by fasting/illness; benign, affects 4-7% of population
- Crigler-Najjar syndrome: Rare, severe UGT deficiency in neonates; risk of kernicterus/bilirubin encephalopathy
- Dubin-Johnson syndrome: Defect in canalicular transport protein (MRP2) → conjugated hyperbilirubinemia; generally benign
- Rotor's syndrome: Similar to Dubin-Johnson but without liver pigmentation
-
Schwartz's Principles of Surgery, 11th ed, p. 1381
3. Posthepatic (Obstructive/Cholestatic) Jaundice
-
Mechanism: Obstruction of bile flow prevents CB from reaching the duodenum; CB regurgitates into blood.
-
Bilirubin type: Predominantly conjugated (direct) hyperbilirubinemia
-
Urine: Dark (bilirubinuria - CB is water-soluble and renally filtered); no urobilinogen (bile not reaching gut)
-
Stool: Pale/clay-colored (absence of stercobilin)
-
Symptoms: RUQ/epigastric pain, nausea, pruritus (bile salt deposition)
-
Causes:
- Intrinsic: Cholelithiasis, choledocholithiasis, cholangiocarcinoma, biliary strictures (benign or malignant), primary sclerosing cholangitis, cholangitis, papilla of Vater disorders
- Extrinsic: Pancreatic cancer (classic painless obstructive jaundice + Courvoisier's sign), pancreatitis, pancreatic pseudocyst
- Iatrogenic: Surgical clip misplacement, retained stones, bile duct injury
-
Schwartz's Principles of Surgery, 11th ed, p. 1381-1382
Comparative Summary Table
| Feature | Prehepatic | Hepatic | Posthepatic |
|---|---|---|---|
| Bilirubin type | Unconjugated ↑ | Both ↑ | Conjugated ↑ |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | Elevated | Elevated | Absent |
| Stool color | Normal/dark | Pale | Pale/clay |
| ALT/AST | Normal | Elevated | Normal/elevated |
| ALP/GGT | Normal | Variable | Markedly elevated |
| Key causes | Hemolysis | Hepatitis, cirrhosis | Gallstones, pancreatic Ca |
Neonatal Jaundice
A special form of prehepatic + hepatic jaundice. It results from:
- Accelerated physiological hemolysis (fetal Hb replacement)
- Immature hepatic UGT enzyme expression (delayed postnatal induction)
This causes physiological jaundice, typically appearing day 2-3 of life and resolving within 1-2 weeks. Severe hyperbilirubinemia risks kernicterus (UCB deposition in basal ganglia causing permanent neurological damage). Treatment is phototherapy (converts bilirubin to water-soluble isomers excreted in urine without conjugation). G6PD deficiency worsens neonatal jaundice, especially when co-inherited with a UGT1A1 polymorphism (Gilbert's variant). - Goldman-Cecil Medicine; Lippincott's Biochemistry
Clinical Approach to a Jaundiced Patient
- History: Duration, associated pain (colicky = stones; painless = malignancy), fever (cholangitis), drug/alcohol use, travel, family history
- Physical exam: Hepatomegaly, splenomegaly, stigmata of chronic liver disease, Courvoisier's sign (palpable gallbladder in painless jaundice = suggests malignant obstruction)
- Labs:
- Fractionated bilirubin (direct vs. indirect)
- LFTs: ALT, AST (hepatocellular pattern) vs. ALP, GGT (cholestatic pattern)
- CBC (hemolysis: anemia, reticulocytosis, elevated LDH, low haptoglobin)
- Peripheral smear
- Coagulation (PT/INR - synthetic function)
- Imaging: Ultrasound abdomen (first-line to detect biliary dilation, stones, liver lesions); CT or MRCP for further characterization; ERCP for therapeutic intervention
- Important: ERCP should not be the primary investigation if hilar cholangiocarcinoma is suspected - axial imaging first. - Maingot's Abdominal Operations
Pruritus in Jaundice
Jaundice is commonly associated with pruritus (from bile salt deposition). Management options include:
-
Topical: Astringents, moisturizers, steroid creams
-
Antihistamines (H1 and H2), phenothiazines, bile acid resins (cholestyramine)
-
Opioid antagonists (note: reverses analgesia in patients on opioids)
-
Rifampicin, gabapentin (anecdotal evidence)
-
Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Sources: Lippincott Illustrated Reviews: Biochemistry 8th ed | Schwartz's Principles of Surgery 11th ed | Goldman-Cecil Medicine | Sleisenger & Fordtran's GI & Liver Disease | Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.