Classify gall stones. Discuss the etiopathogenesis. Clinical features, investigation and treatment of acute calculous cholecystits.Describe etiology, clinical features, investigations, differential diagnosis and management of Gallstones***** ➢ Discuss obstructive jaundice with investigations and management***
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
GALLSTONES (CHOLELITHIASIS) AND ACUTE CALCULOUS CHOLECYSTITIS
PART 1: CLASSIFICATION OF GALLSTONES
Gallstones affect 10-20% of adult populations in high-resource countries. More than 95% of biliary tract disease is attributable to gallstones. In the USA/Europe, over 80% are cholesterol or mixed stones; in Asia, 80% are pigment stones.
Three Main Types:
| Type | Composition | Key Associations |
|---|---|---|
| Cholesterol stones | >50% crystalline cholesterol monohydrate | Obesity, female sex, OCP, pregnancy, rapid weight loss, ileal disease |
| Black pigment stones | Bilirubin polymer + calcium phosphate + calcium bicarbonate; <30% cholesterol | Haemolysis (hereditary spherocytosis, sickle cell disease), cirrhosis, advancing age |
| Brown pigment stones | Calcium bilirubinate + calcium palmitate + calcium stearate + cholesterol | Bile stasis, infection (E. coli, Clonorchis sinensis, Ascaris lumbricoides), bile duct foreign bodies |
Mixed stones contain 50-99% pure cholesterol with an admixture of calcium salts, bile acids, bile pigments and phospholipids.
PART 2: ETIOPATHOGENESIS OF GALLSTONES
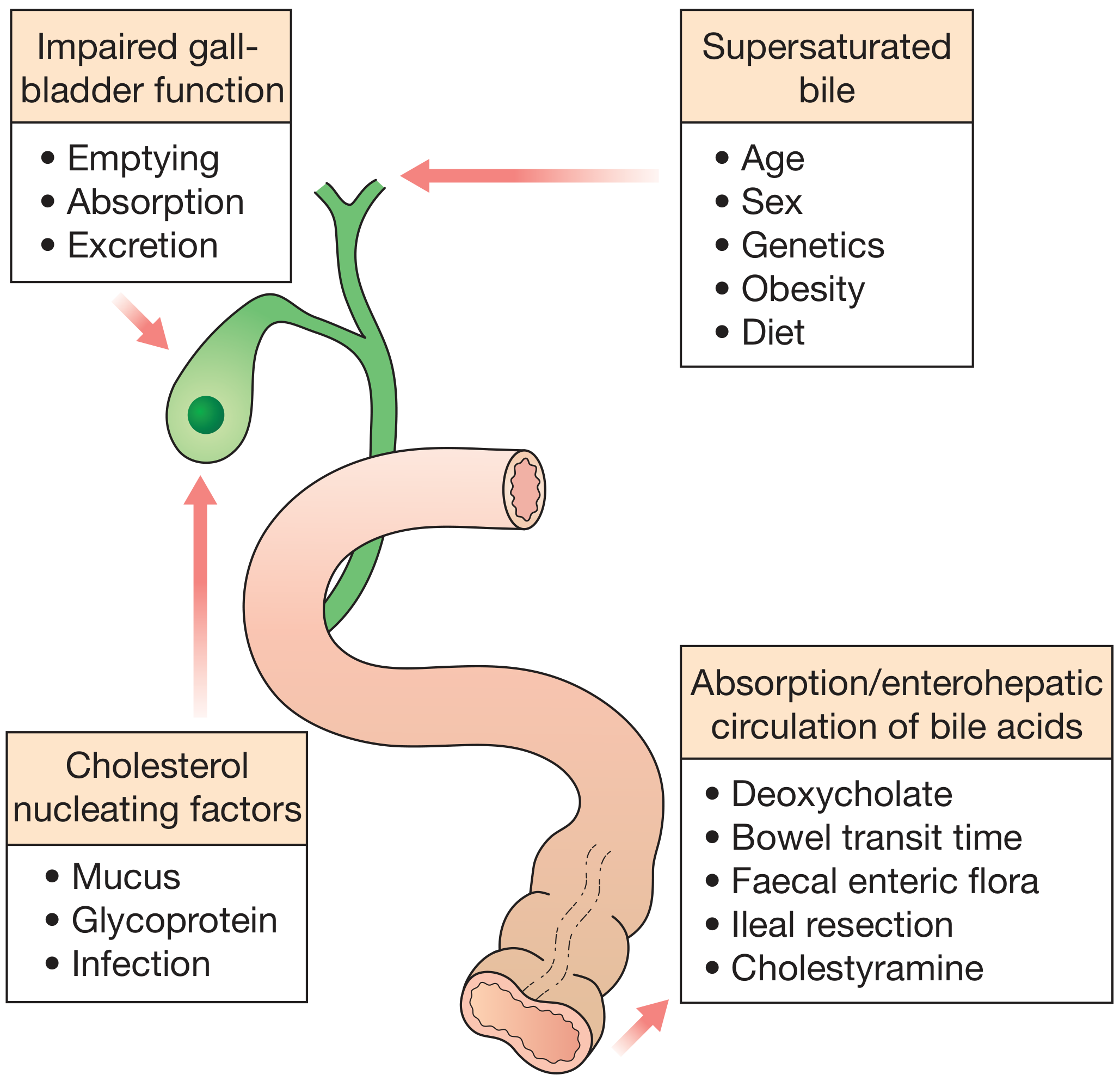
Cholesterol Stone Formation - Three Steps:
Step 1 - Supersaturation of bile with cholesterol:
- Cholesterol is insoluble in water and secreted from the canalicular membrane in phospholipid vesicles
- When bile is supersaturated with cholesterol and/or bile acid concentrations are low, unstable unilamellar phospholipid vesicles form
- Factors increasing cholesterol secretion: obesity, high-calorie diet, oral contraceptives, oestrogens (increase hepatic lipoprotein receptors and stimulate hepatic cholesterol synthesis)
- Factors depleting bile acid pool: ileal disease (Crohn's), ileal resection, cholestyramine
Step 2 - Nucleation of cholesterol crystals:
- Cholesterol monohydrate crystals nucleate from multilamellar vesicles
- Nucleating factors include mucus, glycoproteins, and infection
Step 3 - Gallbladder hypomotility/stasis:
- Abnormal gallbladder emptying aids aggregation of nucleated crystals
- This is why removing stones without removing the gallbladder leads to recurrence
Factors in gallstone formation:
Risk Factors (The "5 F's" mnemonic expanded):
- Fat - obesity, metabolic syndrome, hyperlipidaemia
- Female - higher prevalence due to oestrogen exposure
- Fertile - pregnancy increases biliary cholesterol secretion
- Forty - increasing age; predominantly middle to older age
- Fair - Northern Europeans, North/South Americans, Native Americans (Pima, Hopi, Navajo tribes up to 75%)
- Additional: oral contraceptives, rapid weight reduction, gallbladder stasis, inborn bile acid metabolism disorders, total parenteral nutrition, vagotomy
Pigment Stone Pathogenesis:
- Black stones: Unconjugated bilirubin increases due to haemolysis → precipitates as bilirubin polymer in concentrated supersaturated bile
- Brown stones: Bacterial β-glucuronidase (from E. coli, Bacteroides) deconjugates bilirubin glucuronide → insoluble unconjugated bilirubinate precipitates in infected stagnant bile in ducts
PART 3: CLINICAL FEATURES OF GALLSTONES
Asymptomatic ("silent") gallstones - >80% of cases:
- Prophylactic cholecystectomy generally NOT indicated
- 20-year follow-up: only 18% develop biliary pain; mean yearly probability is 2% in first 5 years, declining to 0.5% by years 10-20
Symptomatic gallstones:
- Right upper quadrant (RUQ) or epigastric pain, radiating to the back or right shoulder tip
- Pain is typically dull, continuous, and severe (not truly "colicky") - lasts minutes to hours
- Associated nausea, vomiting, anorexia
- Pain often starts at night (wakes the patient)
- Relieved when stone slips back into the gallbladder body
- Dyspepsia, flatulence, fatty food intolerance (less specific symptoms)
Complications - clinical presentations:
- Acute cholecystitis: fever, positive Murphy's sign, RUQ mass (omental wall-off)
- Empyema of gallbladder: high fever, rigors, severely ill patient
- Gangrene and perforation: peritonitis
- Choledocholithiasis: obstructive jaundice (dark urine, pale stools, pruritus)
- Cholangitis: Charcot's triad (RUQ pain + fever/rigors + jaundice); Reynolds' pentad adds shock + confusion
- Pancreatitis: epigastric pain radiating to the back, elevated amylase/lipase
Differential Diagnosis of biliary colic:
- Peptic ulcer disease / gastritis
- Acute pancreatitis
- Hepatitis (acute)
- Right-sided renal colic
- Myocardial infarction (inferior MI can mimic biliary pain)
- Irritable bowel syndrome
- Hiatus hernia / GORD
- Appendicitis (atypical)
PART 4: INVESTIGATIONS FOR GALLSTONES
Bloods:
- FBC - leucocytosis in cholecystitis (WBC >18,000/mm³ indicates moderate severity by Tokyo Guidelines)
- LFTs - elevated ALP, GGT, conjugated bilirubin if CBD involvement; transaminases elevated in hepatitis/pancreatitis
- Serum amylase/lipase - if pancreatitis suspected
- CRP - inflammatory marker to assess severity
- PT/INR - may be prolonged if jaundiced (Vitamin K deficiency)
- Serum albumin - marker of nutritional status
Imaging:
| Investigation | Role | Sensitivity |
|---|---|---|
| Ultrasound (1st line) | Detects gallstones, GB wall thickening (>4mm), pericholecystic fluid, acoustic shadowing, CBD diameter | ~95% for GB stones |
| MRCP | Best non-invasive test for CBD stones, strictures, choledocholithiasis | ~95% overall for biliary obstruction |
| CT abdomen | Excludes complications (perforation, abscess), detects CBD stones (less sensitive than MRCP), staging of malignancy | High for masses >2cm |
| HIDA scan (hepatobiliary iminodiacetic acid) | Functional assessment; non-filling = cystic duct obstruction (acute cholecystitis) when US equivocal | ~95% sensitivity for acute cholecystitis |
| ERCP | Therapeutic gold standard for CBD stones - sphincterotomy, stone extraction, stenting | Also diagnostic for strictures |
| EUS (endoscopic ultrasound) | Excellent for distal CBD, ampullary region tumors, FNA for tissue; sensitivity 84-91% for CBD stones | Better than MRCP for small stones |
Ultrasound criteria for acute cholecystitis:
- Sonographic Murphy's sign
- Gallbladder wall thickening >4mm
- Pericholecystic fluid
- Distended gallbladder with gallstones
PART 5: ACUTE CALCULOUS CHOLECYSTITIS
Pathogenesis:
Acute calculous cholecystitis accounts for 90% of all acute cholecystitis cases. The sequence is:
- Stone impaction in the cystic duct or gallbladder neck → outflow obstruction
- Chemical inflammation - mucosal phospholipases hydrolyze luminal lecithins to toxic lysolecithins → disrupts the protective glycoprotein mucus layer → bile salts exert direct detergent action on mucosa
- Prostaglandin release from distended gallbladder wall → mucosal and mural inflammation
- Distension and raised intraluminal pressure → compromised mucosal blood flow
- Bacterial superinfection (later phase) - bacteria from: E. coli, Klebsiella, Enterococcus, Bacteroides, Clostridium
- Progression → gangrenous cholecystitis → perforation → empyema/peritonitis
Clinical Features:
- Onset: Progressive RUQ or epigastric pain lasting >6 hours (distinguishes it from biliary colic)
- Fever: Low-grade initially; high fever suggests gangrenous cholecystitis or empyema
- Nausea and vomiting
- Anorexia, tachycardia, sweating
Physical signs:
- Murphy's sign (pathognomonic) - RUQ tenderness exacerbated during inspiration when palpating the right subcostal region; the patient catches their breath
- RUQ tenderness and guarding - tenderness, voluntary guarding
- Palpable mass - inflamed gallbladder walled off by omentum
- Jaundice (in ~20%) - due to CBD compression by periductal inflammation (Mirizzi syndrome) or concurrent choledocholithiasis
Complications:
- Empyema of the gallbladder - pus filling the lumen; high fever, rigors, very tender mass
- Gangrenous cholecystitis - wall necrosis; gas-forming organisms → emphysematous cholecystitis
- Perforation - generalised biliary peritonitis or localised pericholecystic abscess
- Fistula - cholecystoduodenal, cholecystocolic, or cholecystogastric
- Gallstone ileus - large stone erodes into duodenum, causes small bowel obstruction at ileocaecal valve
- Mirizzi syndrome - stone in cystic duct compresses common hepatic duct
Tokyo Guidelines 2018 - Severity Grading:
Grade I (Mild): Acute cholecystitis in a healthy patient with no organ dysfunction; mild inflammatory changes in the gallbladder
Grade II (Moderate): Any one of:
- Elevated WBC >18,000/mm³
- Palpable tender mass in RUQ
- Duration of symptoms >72 hours
- Marked local inflammation (gangrenous/emphysematous cholecystitis, pericholecystic abscess)
Grade III (Severe): Organ dysfunction in any one of:
- Cardiovascular: hypotension requiring dopamine ≥5 μg/kg/min or any epinephrine
- Neurological: decreased level of consciousness
- Respiratory: PaO₂/FiO₂ ratio <300
- Renal: oliguria; creatinine >2.0 mg/dL
- Hepatic: PT-INR >1.5
- Haematological: platelets <100,000/mm³
Management of Acute Calculous Cholecystitis:
Initial (non-operative) treatment:
- Nil by mouth + IV fluid resuscitation until pain resolves
- Analgesia - NSAIDs (diclofenac IM/IV reduces intraluminal pressure via prostaglandin inhibition), opioids (pethidine preferred over morphine to avoid Oddi spasm)
- IV Antibiotics - as cystic duct is blocked, serum concentration matters more than biliary concentration:
- Mild-moderate: cefazolin, cefuroxime, cefoxitin, or ciprofloxacin
- Severe: piperacillin-tazobactam or 3rd-generation cephalosporin + metronidazole
- Add anaerobic cover if gangrenous/emphysematous cholecystitis suspected
- Monitoring: temperature, pulse, WBC, CRP
Investigations to confirm:
- USG to confirm (first-line)
- If jaundiced: MRCP to exclude choledocholithiasis
- If complicated: CT scan
Surgical Management - Timing:
| Timing | Recommendation | Evidence |
|---|---|---|
| Early cholecystectomy (within 72h-7 days) | Preferred; safe if experienced surgeon available | Shorter total hospital stay (9.6 vs 17.8 days combined RCT data) |
| Delayed/interval cholecystectomy (6 weeks later) | If early surgery not feasible or Grade II with no deterioration | 26% failure requiring emergency surgery before 6 weeks |
| Emergency surgery | Grade III; imminent perforation; diagnostic uncertainty | Urgent |
- Laparoscopic cholecystectomy is the gold standard (higher conversion rate in acute vs. elective but still preferred)
- Tokyo Guidelines algorithm: Grade I → early laparoscopic cholecystectomy; Grade II → early LC if experienced surgeon available, otherwise conservative + delayed LC; Grade III → ICU stabilisation first, then LC when stable or cholecystostomy as bridge
- Percutaneous cholecystostomy - for Grade III patients unfit for surgery; tube drainage of gallbladder as a temporising measure
OBSTRUCTIVE JAUNDICE
DEFINITION
Obstructive (post-hepatic/cholestatic) jaundice is the clinical manifestation of impaired flow of conjugated bilirubin through the biliary tree into the duodenum. Total serum bilirubin is elevated, predominantly the direct (conjugated) fraction (>50% of total).
ETIOLOGY / CAUSES
Malignant (Painless, Progressive):
- Carcinoma of the head of pancreas (most common malignant cause)
- Cholangiocarcinoma (Klatskin tumour at hilum)
- Carcinoma of the gallbladder
- Ampullary carcinoma
- Metastatic disease compressing the biliary system
Benign (often Painful, Fluctuating):
- Choledocholithiasis (most common cause overall - painful, fluctuating)
- Primary or secondary sclerosing cholangitis
- Benign biliary strictures (post-operative, post-inflammatory)
- Choledochal cyst
- Parasites (Clonorchis sinensis, Ascaris)
- Haemobilia
- Pancreatic pseudocysts
- Chronic pancreatitis (pseudotumoral)
- Duodenal diverticulum / ampullary scarring
Congenital:
- Biliary atresia
- Caroli's disease
Key clinical pointer: Painful jaundice → likely stones; Painless progressive jaundice → likely malignancy (Courvoisier's law: a palpable non-tender gallbladder in the presence of jaundice is unlikely to be due to stones)
CLINICAL FEATURES
Symptoms:
- Jaundice - yellow discolouration of skin, sclerae, mucous membranes
- Dark urine (conjugated bilirubin - water soluble, excreted in urine → "Coca-Cola urine")
- Pale/clay-coloured stools (absence of stercobilinogen)
- Pruritus - due to bile salt deposition in skin; often severe
- Fatigue
- Abdominal pain - RUQ colicky pain in stones; epigastric pain in pancreatic cancer
- Weight loss, anorexia - suggests malignancy
- Fever and rigors - suggests cholangitis (Charcot's triad: pain + fever + jaundice)
Signs:
- Icteric sclerae, jaundiced skin
- Scratch marks (pruritus)
- Palpable, non-tender gallbladder (Courvoisier's sign) → malignant obstruction
- Hepatomegaly
- Splenomegaly in portal hypertension
- Cachexia, Virchow's node (left supraclavicular lymph node) - in GI malignancy
- Hepatic flap/asterixis if hepatic failure developing
DIFFERENTIAL DIAGNOSIS
| Type | Examples | Bilirubin | ALP | AST/ALT | Urine | Stools |
|---|---|---|---|---|---|---|
| Pre-hepatic | Haemolysis, spherocytosis | Indirect ↑↑ | Normal | Normal | Normal (no bili) | Normal/dark |
| Hepatic | Viral hepatitis, cirrhosis, drugs | Both ↑ | Mildly ↑ | Markedly ↑↑ | Bilirubin+ | Variable |
| Post-hepatic (Obstructive) | Stones, malignancy | Direct ↑↑ | Markedly ↑↑↑ | Mildly ↑ | Dark (bilirubin+) | Pale |
INVESTIGATIONS
Blood Tests:
| Test | Finding in Obstructive Jaundice |
|---|---|
| Total bilirubin | Elevated; repeat every 3-4 days to monitor trend |
| Direct (conjugated) bilirubin | >50% of total; markedly elevated |
| Serum alkaline phosphatase (ALP) | 3-4 fold elevation in 75% of cholestasis cases |
| GGT / 5'-nucleotidase | Elevated (confirms hepatobiliary source vs bone) |
| AST/ALT (transaminases) | Mildly elevated; very high levels (>1000 IU/L) suggest hepatocellular cause |
| Serum albumin | Low in chronic disease / malnutrition |
| PT/INR | Prolonged (Vitamin K malabsorption); corrects with IV Vitamin K in post-hepatic jaundice (unlike hepatic jaundice) - this response differentiates the two |
| FBC | Anaemia of malignancy; leucocytosis in cholangitis |
| Serum amylase/lipase | Elevated in pancreatic pathology |
| CA 19-9, CEA | Tumour markers for pancreatic and biliary malignancy |
| Alpha-fetoprotein | Hepatocellular carcinoma |
| Hepatitis serology (HBsAg, anti-HCV, HAV IgM) | Exclude viral hepatitis |
| ANA, AMA (anti-mitochondrial Ab) | Primary biliary cirrhosis (AMA+); autoimmune hepatitis |
Imaging Investigations:
-
Ultrasound (US) - FIRST LINE:
- Detects biliary duct dilation; establishes level of obstruction in ~67% of cases
- Sensitivity for CBD stones only 21-63% (poor for distal stones)
- Shows liver parenchyma, gallbladder, hepatic/pancreatic masses
-
MRCP (Magnetic Resonance Cholangiopancreatography):
- Non-invasive test of choice for biliary anatomy
- Sensitivity 95% for biliary obstruction; best for CBD stones
- Differentiates strictures but distinguishing benign vs malignant can be challenging
- No therapeutic capability
-
CT abdomen/pelvis:
- Excellent for pancreatic tumours >2cm, staging of malignancy
- Identifies vascular involvement, lymphadenopathy, metastases
- Less sensitive than MRCP for CBD stones
-
EUS (Endoscopic Ultrasound):
- Best for distal CBD, ampullary region, pancreatic head
- Enables fine-needle aspiration (FNA): sensitivity 84-91%, specificity 71-100%
- Can identify vascular invasion and lymph node metastases
-
ERCP (Endoscopic Retrograde Cholangiopancreatography):
- Primarily therapeutic (not just diagnostic)
- Cannulation successful in >90% cases
- Enables: sphincterotomy, stone extraction, balloon sweep, stent placement, brush cytology
- Complications: pancreatitis, cholangitis, bleeding, perforation
-
Percutaneous Transhepatic Cholangiography (PTC):
- Used when ERCP fails or inaccessible anatomy
- Allows external biliary drainage, internal stenting
-
Liver biopsy:
- Reserved for suspected parenchymal disease
- Contraindicated if PT prolonged and unresponsive to Vitamin K, or platelets <50,000/mm³
MANAGEMENT OF OBSTRUCTIVE JAUNDICE
General Preoperative Preparation:
-
Correction of coagulation:
- IV Vitamin K₁ 20 mg → rapid normalisation of PT within 12-24 hours (if liver synthetic function intact)
- Good response = post-hepatic obstruction (favourable surgical risk)
- Poor response = hepatocellular disease
-
Renal protection:
- Jaundiced patients at high risk of hepatorenal syndrome
- Aggressive IV fluid hydration pre- and post-operatively
- Monitor urine output; consider mannitol infusion
- Avoid nephrotoxic drugs
-
Nutritional support - correct malnutrition, hypoalbuminaemia
-
Antibiotics - treat concurrent cholangitis with broad-spectrum cover
Surgical mortality in jaundiced patients: ~20%; recognised risk factors:
- Old age
- Malnutrition
- Ongoing biliary infection
- Malignancy
- High serum urea (renal impairment)
Definitive Management Based on Cause:
A. Choledocholithiasis (CBD stones):
- ERCP + endoscopic sphincterotomy + stone extraction (first-line)
- Basket or balloon retrieval of stones
- Lithotripsy for large stones
- Followed by laparoscopic cholecystectomy for the gallbladder
B. Malignant Obstruction (Pancreatic/Bile Duct Cancer):
Resectable disease (~20% of periampullary cancers):
- Pancreaticoduodenectomy (Whipple's procedure) for periampullary/pancreatic head tumours
- Preoperative biliary drainage: controversial - not proven to reduce operative mortality; however, needed if neoadjuvant chemotherapy is planned
Non-resectable disease:
- Biliary decompression/palliation:
- ERCP + stenting (first-line for distal obstruction)
- Plastic stents: cheap but occlude every 3-4 months (biofilm formation); patency ~43 days
- Self-expanding metallic stents (SEMS): wider bore, patency ~125 days; preferred for >6 months survival
- Covered SEMS (cSEMS): prevent tumour ingrowth, removable; meta-analysis shows fewer adverse events vs uncovered SEMS
- Percutaneous transhepatic drainage (when ERCP fails)
- Surgical bypass (hepaticojejunostomy or choledochojejunostomy) if endoscopic approach not possible
- ERCP + stenting (first-line for distal obstruction)
- Only 25-30% of liver volume needs to be drained for jaundice resolution
- Right hepatic duct drains 50-55% of liver
- Left hepatic duct drains 30-35%
- Caudate lobe drains 10%
C. Benign Biliary Strictures (Bismuth Classification):
| Type | Level | Treatment |
|---|---|---|
| I | Low CHD stump >2 cm | ERCP dilation + plastic stents |
| II | Proximal CHD stump <2 cm | ERCP or surgical repair |
| III | Hilar; confluence preserved | Hepaticojejunostomy |
| IV | Hilar; confluence lost | Complex hepaticojejunostomy |
| V | Aberrant right sectoral duct | Surgical |
- Endoscopic treatment: serial large-bore plastic stents exchanged every 3-4 months; success 74-90%, recurrence up to 30% at 2 years
- Surgical hepaticojejunostomy (Roux-en-Y) for failed endoscopic treatment
D. Sclerosing Cholangitis:
- Ursodeoxycholic acid (medically)
- Dominant strictures: ERCP dilation + stenting
- Liver transplantation for end-stage disease
Summary Algorithm for Obstructive Jaundice:
Jaundice suspected
↓
Blood tests (LFTs, bilirubin fractions, ALP, transaminases, PT)
↓
Ultrasound abdomen (1st line)
↓
Biliary dilation?
YES NO
↓ ↓
MRCP/CT/EUS Consider hepatic/pre-hepatic cause
↓
Cause identified?
Stones → ERCP + extraction Malignancy → Resectable? → Whipple's
→ Non-resectable → ERCP stent / PTC
Benign stricture → ERCP or surgical bypass
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition - Chapters on Gallstones, Acute Cholecystitis
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Gallbladder pathology
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Acute Cholecystitis, Obstructive Jaundice
- Current Surgical Therapy, 14th Edition - Obstructive Jaundice evaluation and endoscopic management
- Pye's Surgical Handicraft, 22nd Edition - Management of obstructive jaundice, preoperative preparation
This is a shared conversation. Sign in to Orris to start your own chat.