How can I diagnose ARDS in ward setting without any ventilator available.. I am new PGR In general medicine ..
"acute respiratory distress syndrome" AND "diagnosis" AND "non-invasive"
PMID: 41935702
Diagnosing ARDS in a Ward Setting Without a Ventilator
1. Understand What ARDS Is (Briefly)
- Murray & Nadel's Textbook of Respiratory Medicine: "No diagnostic gold standard exists for ARDS, and it remains unclear whether it represents a single pathophysiologic process or multiple processes with similar clinical presentations."
2. The Berlin Definition - What It Requires and What to Do Without a Ventilator
| Criterion | Requirement |
|---|---|
| Timing | Onset within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest imaging | Bilateral opacities on CXR/CT - not fully explained by collapse, nodules, or effusion |
| Origin of edema | Respiratory failure not fully explained by cardiac failure or fluid overload |
| Oxygenation | PaO₂/FiO₂ (P/F ratio) ≤300 mmHg with PEEP ≥5 cmH₂O |
3. The Ward Workaround - Use the S/F Ratio Instead of P/F Ratio
"A 2007 analysis of ARDSnet data showed that the S/F ratio strongly correlated with a simultaneously drawn P/F ratio, and that an S/F ratio of 315 corresponds to a P/F ratio of 300 (the diagnostic cutoff for ARDS)."
S/F Ratio Cutoffs (ARDS Severity):
| Severity | P/F Ratio | Equivalent S/F Ratio |
|---|---|---|
| Mild | 201-300 mmHg | ~240-315 |
| Moderate | 101-200 mmHg | ~148-240 |
| Severe | ≤100 mmHg | ≤148 |
Important caveat: S/F ratio is most accurate when SpO₂ is ≤96%. If the patient is maintaining SpO₂ >97% on oxygen, the non-linear relationship makes this less reliable.
How to Calculate S/F Ratio on the Ward:
| Device | Flow Rate | Approximate FiO₂ |
|---|---|---|
| Nasal cannula | 1 L/min | 0.24 |
| Nasal cannula | 2 L/min | 0.28 |
| Nasal cannula | 4 L/min | 0.36 |
| Nasal cannula | 6 L/min | 0.44 |
| Simple face mask | 6-8 L/min | 0.40-0.50 |
| Non-rebreather mask | 10-15 L/min | 0.60-0.90 |
| Room air | - | 0.21 |
4. Assess the Bilateral Opacities - CXR on the Ward
- Bilateral diffuse alveolar infiltrates/opacities
- Affecting all lung zones
- Not explained by pleural effusions alone, lobar collapse, or nodules
- No features of cardiogenic pulmonary edema (Kerley B lines, cardiomegaly, upper lobe diversion) - though these can coexist
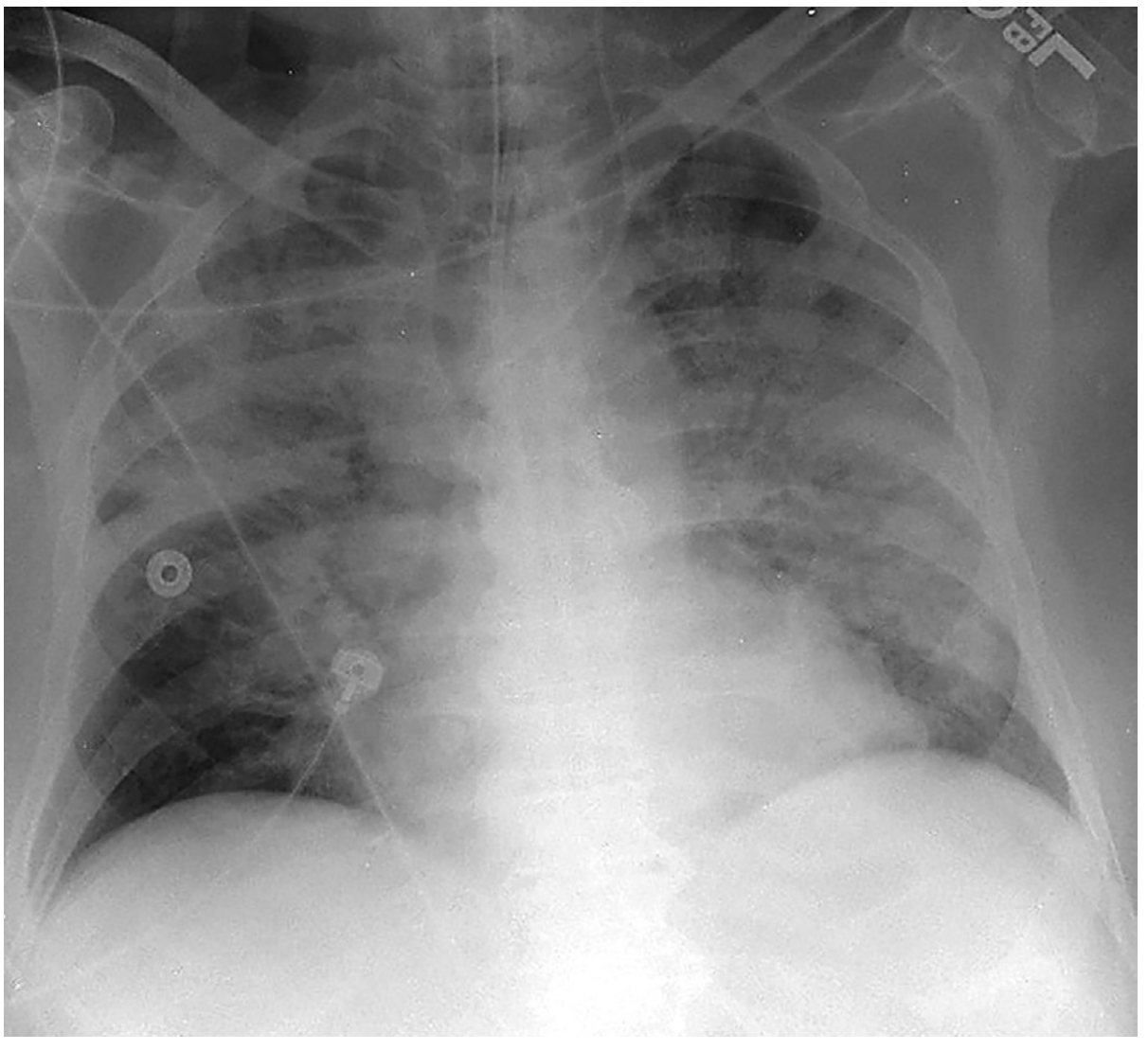
Note: Inter-observer variability for CXR interpretation in ARDS is moderate (kappa ~0.5), so training and experience matter. When in doubt, always discuss with a senior.
5. Exclude Cardiogenic Pulmonary Edema (the Most Important Differential)
- History of heart failure, valvular disease, ACS?
- JVP elevated? S3 gallop on auscultation?
- Respond to diuresis? (Cardiogenic edema responds; ARDS does not)
- BNP/NT-proBNP: A very low level argues against heart failure, but elevated BNP does NOT exclude ARDS (many ARDS patients have concurrent elevated BNP due to RV strain)
- Bedside echo (point-of-care ultrasound): If available, look for LV dysfunction, dilated LA/LV, mitral regurgitation
6. Identify a Precipitating Cause (Always Look!)
- Pneumonia (bacterial, viral - especially COVID-19, influenza)
- Aspiration of gastric contents
- Inhalation injury / near-drowning
- Sepsis (most common overall cause)
- Severe trauma / polytrauma
- Pancreatitis
- Massive transfusion / transfusion-related acute lung injury (TRALI)
- Drug overdose / toxins
7. Lung Ultrasound (LUS) - If Available on Your Ward
- Bilateral B-lines (≥3 B-lines per intercostal space) - highest specificity when bilateral
- Diffuse non-homogeneous B-line pattern (irregular, spared areas)
- Subpleural consolidations
- Pleural line abnormalities (thickened, irregular)
- Absence of A-lines (which would suggest normal aeration)
LUS is particularly useful in resource-limited settings and wards without ABG or ventilators.
8. A Practical Ward Diagnostic Checklist
- Timeline: Did symptoms start within the last 7 days? Is there a known insult (sepsis, pneumonia, trauma, pancreatitis)?
- Bilateral opacities on CXR: Are they present? Are they not explained by collapse or pleural effusion alone?
- Exclude cardiac cause: No clinical evidence of left heart failure as the primary driver? (Bedside echo / BNP helpful)
- Oxygenation: Calculate S/F ratio using SpO₂ and FiO₂. Is S/F ≤315? (Equivalent to P/F ≤300)
- ABG: Get one if possible - a PaO₂ lets you calculate the true P/F ratio and also identifies hypercapnia from respiratory fatigue
- LUS: If available, confirm bilateral B-line pattern
9. Key Points to Remember
- ARDS is a clinical diagnosis - no gold standard test exists
- The S/F ratio (SpO₂/FiO₂) is your best friend on a ward without ABG or ventilator - S/F ≤315 is equivalent to P/F ≤300
- Bilateral CXR opacities + a known risk factor + hypoxemia = suspect ARDS until proven otherwise
- Always exclude cardiogenic pulmonary edema - this is the primary differential
- Lung ultrasound is a validated, radiation-free bedside tool with good diagnostic accuracy
- Recognizing ARDS early on the ward is more important than formal criteria - if you suspect it, act and escalate
- Fishman's Pulmonary Diseases and Disorders, SpO₂/FiO₂ section
- Murray & Nadel's Textbook of Respiratory Medicine, ARDS Diagnosis chapter
- Tintinalli's Emergency Medicine, Table 29B-1 (Berlin Definition)
- Current Surgical Therapy 14e, ARDS section
- Sreedharan JK et al. "Lung ultrasound for ARDS diagnosis: A systematic review and meta-analysis." Respiratory Medicine, 2026. [PMID: 41935702]
How to assess different types of blood transfusion reactions clinically with history, timing, clinical examination in emergency and wards effectively
"transfusion reactions" AND "diagnosis" AND "clinical"
Clinical Assessment of Blood Transfusion Reactions - A Practical Guide for the Ward & Emergency
Epidemiology - Know the Frequencies First
| Reaction | Incidence per Unit |
|---|---|
| Febrile non-haemolytic (FNHTR) | ~1:1,100 (most common) |
| Allergic (mild) | ~1:1,200 |
| Allergic (severe/anaphylaxis) | ~1:15,500 |
| TACO | ~1:9,000 |
| Delayed haemolytic | ~1:32,000 |
| Acute haemolytic (ABO) | ~1:110,000 |
| TRALI | ~1:140,000 |
| Bacterial contamination/Septic | ~1:500,000 (platelets higher risk) |
The Master Framework: Think in Three Axes
Type-by-Type Clinical Assessment
1. Acute Haemolytic Transfusion Reaction (AHTR) - Most Dangerous
- Has the patient had previous transfusions? (prior sensitisation)
- Was there a labelling/identification error? (Ask nursing staff - was the unit checked against wristband?)
- Did symptoms start immediately after the transfusion began?
- Fever (often ≥1-2°C rise within 15 minutes) with rigors
- Chills and flushing
- Chest pain and back/flank pain (very characteristic - from complement activation and renal vasoconstriction)
- Anxiety and sense of impending doom
- Tachycardia and hypotension (shock in severe cases)
- Dyspnoea
- Haemoglobinuria - dark red/brown urine (check urine pad or catheter bag immediately)
- In anaesthetised/unconscious patients: unexplained hypotension, diffuse oozing from wound, haemoglobinuria
- Stop transfusion, return bag to blood bank
- Direct Coombs test (DAT) - will be positive
- Repeat type and crossmatch on fresh sample
- FBC, LFT (unconjugated bilirubin), LDH (elevated), serum haptoglobin (decreased/absent)
- Plasma free haemoglobin (elevated - pink-tinged plasma)
- Urine for haemoglobin (dipstick positive)
- PT, aPTT, fibrinogen (DIC screen)
- U&E/creatinine
Key clinical clue: Back pain + haemoglobinuria + fever starting within minutes of transfusion = AHTR until proven otherwise. This is a medical emergency.
2. Febrile Non-Haemolytic Transfusion Reaction (FNHTR) - Most Common
- Previous transfusions with similar reactions? (increases likelihood of FNHTR)
- Pre-existing fever before transfusion? (must be excluded)
- Which blood product? (platelets more common than RBCs)
- Temperature rise ≥1°C above baseline (or ≥38°C)
- Chills and rigors (sometimes dramatic shaking)
- No skin changes (no urticaria, no flushing)
- Haemodynamics stable (no significant hypotension)
- No haemoglobinuria
Critical point: FNHTR cannot be distinguished from AHTR at the bedside on history and examination alone. Treat as AHTR first, investigate to exclude haemolysis.
3. Allergic Transfusion Reaction - Second Most Common
- Known allergies or atopic history?
- Previous allergic transfusion reactions?
- Prior history of IgA deficiency?
- Which product? (Plasma-containing products - FFP, platelets - more likely than washed RBCs)
| Mild | Moderate/Severe |
|---|---|
| Urticaria (hives) | Generalised urticaria >2/3 body |
| Pruritus | Angioedema (lip/tongue swelling) |
| Flushing | Bronchospasm (wheeze) |
| Normal haemodynamics | Stridor (laryngeal oedema) |
| Hypotension, tachycardia | |
| Shock |
Clinical distinction from AHTR: Allergic reactions typically have urticaria/angioedema and no fever. AHTR has fever, back pain, haemoglobinuria and no urticaria. However, anaphylaxis can mimic AHTR haemodynamically - both can cause severe hypotension.
4. TRALI (Transfusion-Related Acute Lung Injury) - Leading Cause of Transfusion Death
- Which product? (FFP and platelets most common, but any plasma-containing product)
- Did respiratory symptoms start during or within 6 hours of transfusion?
- Any pre-existing lung disease or ARDS risk factors? (Type 1 TRALI vs Type 2 TRALI)
- Acute onset dyspnoea (this is the dominant symptom)
- Hypoxia - rapidly falling SpO₂
- Bilateral coarse crackles on auscultation
- Fever (common)
- Hypotension (in ~50%)
- No signs of fluid overload - JVP NOT elevated, no peripheral oedema (this is the key difference from TACO)
- CXR: bilateral infiltrates (looks just like ARDS)
- New hypoxia (SpO₂ <90% on room air, or PaO₂/FiO₂ <300)
- Bilateral opacities on CXR
- Onset within 6 hours of transfusion
- No pre-existing ALI before transfusion
- No evidence of circulatory overload (TACO)
5. TACO (Transfusion-Associated Circulatory Overload) - Often Missed or Confused with TRALI
- Age >70 years
- Pre-existing cardiac failure, renal failure, low albumin
- Rapid transfusion rate
- Multiple units given in short time (especially >2 units in 6 hours)
- Positive fluid balance >3L
| Feature | TRALI | TACO |
|---|---|---|
| JVP | Normal/low | Elevated |
| BP | Low/normal | Hypertension (common) |
| Response to diuretic | No | Yes - improves |
| Peripheral oedema | Absent | May be present |
| Orthopnoea | Uncommon | Common |
| BNP | Low/normal | Markedly elevated (>1000) |
| CXR | Bilateral infiltrates, no cardiomegaly | Bilateral infiltrates, +/- cardiomegaly, Kerley B lines |
The single most useful clinical bedside test: Elevated JVP + hypertension + orthopnoea during transfusion = TACO. Low/normal JVP + hypotension + fever = TRALI.
6. Septic/Bacterial Transfusion Reaction - Rare but Highly Lethal
- Was the blood bag inspected before transfusion? (purple/black discolouration, gas bubbles, unusual smell are warning signs)
- Was it platelets? (highest risk - stored at 22°C)
- How quickly did the patient deteriorate?
- Fever ≥38°C with rise >1°C (very high - sometimes >40°C)
- Rigors (often violent/dramatic)
- Hypotension and shock (rapid onset)
- Tachycardia
- Nausea, vomiting
- Dyspnoea
- May have warm peripheries early (distributive/septic shock picture)
Key clue: Temperature >40°C + rapid cardiovascular collapse during transfusion, especially with platelets = septic reaction until proven otherwise. Much more dramatic than FNHTR.
7. Delayed Haemolytic Transfusion Reaction (DHTR)
- Previous transfusion 5-14 days ago?
- Haematology patient, sickle cell patient (hyperhemolysis syndrome)?
- Unexplained fever, jaundice, or anaemia worse than expected?
- Often subclinical - found on routine bloods
- Low-grade fever
- Jaundice (new or worsening icterus)
- Pallor (anaemia)
- Dark urine (haemoglobinuria - less dramatic than AHTR)
- Rarely: back pain, flank pain
8. Post-Transfusion Purpura (PTP) and Transfusion-Associated GvHD (TA-GvHD)
- Timing: 5-12 days post-transfusion
- Signs: Sudden-onset petechiae and purpura, thrombocytopenia, gum bleeding
- Mechanism: Anti-platelet antibodies destroy both donor and native platelets
- Timing: 2 days to 6 weeks after transfusion
- Signs: Triad of fever + rash (starts on trunk, spreads peripherally) + diarrhoea, with hepatitis and pancytopenia
- Occurs in immunocompromised patients or if receiving blood from a family member (HLA-similar donor)
- Extremely high mortality (>90%)
Master Summary Table: Timing + Dominant Signs
| Reaction | Timing | Fever | Rash/Urticaria | Dyspnoea | BP | Haemoglobinuria | Dominant Clue |
|---|---|---|---|---|---|---|---|
| AHTR | Minutes-24h | +++, sudden | No | ± | Low (shock) | Yes | Back pain + haemoglobinuria |
| FNHTR | 1-6h | ++, gradual | No | No | Normal | No | Fever only, stable |
| Allergic (mild) | Minutes-2h | No | Yes - hives | No | Normal | No | Urticaria |
| Anaphylaxis | Minutes | No | ± severe | Yes - wheeze/stridor | Very low | No | Stridor + shock |
| TRALI | <6h | ++ | No | Severe | Low | No | Non-cardiogenic pulm. oedema |
| TACO | <12h | ± | No | Yes | High | No | JVP↑ + HT + orthopnoea |
| Septic | During/rapid | +++, >40°C | No | ± | Low (shock) | No | Explosive rigors + shock |
| DHTR | 3-14 days | ± | No | No | Normal | ± | Jaundice + falling Hb |
| PTP | 5-12 days | No | Purpura | No | Normal | No | Petechiae + thrombocytopenia |
| TA-GvHD | 2-42 days | Yes | Rash + diarrhoea | No | Normal | No | Rash + diarrhoea + pancytopenia |
The First 5 Minutes: Universal Ward Response Algorithm
- Stop the transfusion - immediately, no matter what reaction is suspected
- Keep IV line open with 0.9% saline (new line if possible - don't use the same giving set)
- Assess A-B-C: airway, breathing, circulation - vital signs, SpO₂
- Look for haemoglobinuria - inspect urine (catheterise if needed)
- Call for help + notify blood bank immediately, return blood bag
- Assess clinically using the framework above
- Draw blood samples (before giving any IV fluids) for urgent investigations:
- Repeat group and crossmatch (fresh sample, correct labelling)
- Coombs test (DAT)
- FBC, LDH, haptoglobin, indirect bilirubin, plasma free Hb
- U&E, coagulation (PT, aPTT, fibrinogen)
- Blood cultures (if septic reaction suspected)
Practical Memory Aids
- Back pain + dark urine early in transfusion = AHTR (emergency)
- Hives + itch, no fever = Allergic (may be safe to restart after antihistamine if mild)
- Fever only, haemodynamics stable = FNHTR (but exclude AHTR first)
- Acute breathlessness + bilateral infiltrates + low BP + within 6h = TRALI (non-cardiogenic)
- Acute breathlessness + high BP + high JVP + within 12h = TACO (cardiogenic overload)
- Explosive >40°C fever + rapid shock with platelets = Septic reaction
- Jaundice + fever 5-14 days later = DHTR
- Petechiae 5-12 days later = Post-transfusion purpura
- Rash + diarrhoea + pancytopenia weeks later in immunocompromised = TA-GvHD
- Goldman-Cecil Medicine International Edition, Transfusion Reactions chapter (Tables 162-2, 162-3)
- Tintinalli's Emergency Medicine, Table 238-7 (Transfusion Reactions)
- Harrison's Principles of Internal Medicine 22E, Haemolytic Transfusion Adverse Reactions chapter
- Hirayama F et al. "Recent progress in understanding of allergic transfusion reaction." Curr Opin Immunol, 2025. [PMID: 40840009]
- Lowack J et al. "Pulmonary transfusion reactions as an immunological spectrum disorder." Curr Opin Immunol, 2026. [PMID: 41202391]
What is the clinical significance of pancytopenia in a patient with decompensated liver disease? How to proceed further and what differential diagnosis to be kept in mind and how to treat them in each of the differential causes
"pancytopenia" AND "cirrhosis" AND "hematologic"
"pancytopenia" AND "liver cirrhosis"
- Blood film - it's the single most informative, cheapest, fastest test
- Ask: is this proportionate to the liver disease? - if platelet count is <30,000/µL or WBC <1,500/µL, don't just label it hypersplenism
- Look for red flags - lymphadenopathy, massive splenomegaly, bone pain, night sweats, leukoerythroblastic picture → get haematology involved and consider bone marrow biopsy
How to assess different types of shocks clinically in the emergency department, especially if a patient presents in shock with cold peripheries and no other obvious signs of infection, MI is present. What differential diagnosis should be kept in mind and how to proceed and treat each accordingly?
How to assess different types of shocks clinically in the emergency department, especially if a patient presents in shock with cold peripheries and no other obvious signs of infection, MI is present. What differential diagnosis should be kept in mind and how to proceed and treat each accordingly? Especially in resource-limited settings where only simple baselines are available and no invasive procedures can be done
- Feel the neck veins (JVP) - this one sign divides your differential in half immediately
- Listen to the chest (pulmonary oedema vs. clear vs. absent breath sounds)
- Check the ECG - STEMI/LBBB = reperfuse; S1Q3T3/RBBB = PE; electrical alternans = tamponade; bradycardia/complete heart block = pacemaker
How to diagnose pulmonary embolism in ward settings with limited resources and how to treat it when clinical suspicion is high? What is the dosage of anticoagulants, especially heparin and enoxaparin, warfarin given prophylactically in different ward patients for pulmonary embolism, for the patients that are bedridden for a longer period of time and especially when the hospital stay is five or more than five days?
"pulmonary embolism" AND "diagnosis" AND "treatment" AND "guidelines"
| Purpose | Drug | Dose |
|---|---|---|
| Prophylaxis (any bedridden patient ≥5 days, Padua ≥4) | Enoxaparin | 40 mg SC OD |
| Prophylaxis (if renal failure eGFR <30) | UFH | 5,000 units SC BD |
| Treatment (confirmed/strongly suspected PE, haemodynamically stable) | Enoxaparin | 1 mg/kg SC every 12 hours |
| Treatment (unstable/shock/thrombolysis candidate) | UFH | 80 units/kg IV bolus + 18 units/kg/hr infusion |
| Transition to oral (long-term after 5+ days of injectable) | Warfarin | 5 mg OD, target INR 2-3 |
- Never use warfarin alone for acute PE - always bridge with heparin/LMWH for minimum 5 days until INR is ≥2 for 2 consecutive days
- In renal failure - avoid LMWH; use UFH (aPTT-monitored)
- In massive PE with shock - thrombolysis first (streptokinase 1.5 million IU over 2 hours), heparin follows after aPTT normalises
- Prophylaxis starts on admission - do not wait until day 5; the risk accumulates from day 1
How to clinically suspect infective endocarditis if a patient presents with high-grade fever for one month?
"infective endocarditis" AND "diagnosis" AND "criteria"
Clinical Suspicion of Infective Endocarditis in a Patient with High-Grade Fever for One Month
Part 1: Why Think of IE Immediately?
- Fever is present in 80-96% of IE cases - it is the single most common finding (Braunwald's Heart Disease; Goldman-Cecil)
- Subacute IE (classically caused by viridans streptococci) develops insidiously over weeks to months with non-specific symptoms before diagnosis
- Many patients look "not that sick" despite valvular destruction occurring silently
- Embolic complications (stroke, renal infarction, splenic infarction) can be the presenting event
Part 2: The History - What to Ask (Systematic Approach)
A. Characterise the Fever
- Duration, pattern (continuous vs. intermittent remittent), height of fever
- Associated rigors/chills (common in IE)
- Night sweats
- Response to antipyretics (partial improvement is typical in IE)
- Key: Has the fever been investigated anywhere? Any antibiotics given already? (Prior antibiotics reduce blood culture sensitivity by ~30%)
B. Constitutional Symptoms
| Symptom | % Patients |
|---|---|
| Fever/chills | 80-95% |
| Weakness/fatigue | 40-50% |
| Malaise | 20-40% |
| Night sweats | 20-40% |
| Anorexia + weight loss | 20-40% |
| Myalgias/arthralgias | 10-30% |
| Dyspnoea | 20-40% |
| Headache | 20-40% |
| Back pain (presenting complaint) | 5-10% |
| Confusion/delirium | 10-20% |
C. Predisposing Risk Factors - Ask These Directly
- Rheumatic heart disease (most common in South Asia, Africa - mitral stenosis/regurgitation)
- Congenital heart disease (bicuspid aortic valve, VSD, PDA)
- Prosthetic heart valve (mechanical or bioprosthetic)
- Prior history of IE
- Previous cardiac surgery
- Implantable cardiac devices (pacemaker, ICD leads)
- Mitral valve prolapse with regurgitation
- Hypertrophic obstructive cardiomyopathy
- Intravenous drug use (IVDU) - most common risk factor for tricuspid valve IE; ask carefully and non-judgementally
- Recent dental procedures (dental extraction, root canal within 3 months)
- Recent invasive procedures (colonoscopy, cystoscopy, central line, haemodialysis catheter)
- Haemodialysis patients (high-risk due to repeated vascular access)
- Diabetes mellitus (immunocompromised)
- HIV infection
- Organ transplant/immunosuppression
- Poor dentition/gingival disease
D. Embolic/Focal Symptoms to Ask About
- Sudden focal neurological deficit (stroke from septic embolism to MCA or other cerebral arteries)
- Left-sided chest/flank pain (splenic infarction - left upper quadrant)
- Back pain (vertebral osteomyelitis, psoas abscess from septic emboli)
- Haematuria (renal emboli/infarction or immune-complex glomerulonephritis)
- Visual change (retinal embolism, Roth spots)
- Cold, painful extremity (peripheral arterial embolism)
- Cough/haemoptysis/pleuritic pain = right-sided IE (tricuspid) → septic pulmonary emboli
Part 3: Physical Examination - A to Z (Do Not Miss Any System)
General
- Fever (>38°C) - present in 96% of IE cases (Goldman-Cecil)
- Pallor (anaemia of chronic infection, very common in subacute IE)
- Cachexia/weight loss
- Toxic or "not as ill as expected" appearance
Vital Signs
- Temperature: often 38.5-40°C in acute IE; may be low-grade (37.5-38°C) in subacute IE, elderly, or renal failure
- Tachycardia (compensatory, from fever and anaemia)
- Widened pulse pressure → suggests acute aortic regurgitation (valve destruction)
- Hypotension → septic shock or acute severe valve regurgitation causing heart failure
Hands - Examine Carefully (High Yield)
- Linear, non-blanching, dark red/brown streaks in the nail beds
- Parallel to nail growth direction
- Most significant when in the proximal nail bed (distal splinters are common from trauma and non-specific)
- Present in 5-15% of IE cases
- Can be seen in: vasculitis, trauma, psoriasis, antiphospholipid syndrome (less specific)

- Tender, erythematous or violaceous subcutaneous nodules
- Located on the thenar and hypothenar eminences, pulps of fingers and toes
- They wax and wane over hours-days
- Present in 3-10% of IE; when present, very specific
- Mechanism: Mixed - immune complex deposition + microemboli
- Non-tender, erythematous or haemorrhagic macular lesions
- Located on palms and soles (distinct location from Osler's nodes)
- Embolic in origin (microemboli)
- Present in 5-10% of IE
- Memory trick: Janeway = painless, palms/soles; Osler = painful, On the fingers
- Suggests chronic IE (weeks to months of infection)
- Non-specific but supportive in the right context
Eyes - Do Not Skip
- Small red spots on the bulbar conjunctiva (pull down lower eyelid)
- Present in 10-40% of IE
- Caused by microemboli
- Retinal haemorrhages with a pale centre (composed of coagulated fibrin)
- Present in 2-10% of IE
- Best seen with direct ophthalmoscopy; refer to ophthalmology if suspected
- Also seen in: severe anaemia, leukaemia, SLE, diabetes
Skin - Look Everywhere
- Small non-blanching red/purple spots (<2mm)
- Found most commonly on conjunctiva, palate, and extremities
- Present in 10-40% of IE

Cardiovascular Examination
| Murmur finding | Frequency |
|---|---|
| Any murmur present | 75-85% |
| New murmur | 10-50% |
| Changing/worsening murmur | 5-20% |
- Listen carefully for new murmur or worsening of a known murmur on every examination
- Aortic regurgitation (diastolic murmur) → aortic valve IE → widened pulse pressure, water-hammer pulse, head bobbing (de Musset's sign)
- Mitral regurgitation (pan-systolic murmur at apex) → mitral valve IE
- Tricuspid regurgitation → IVDU-associated IE (pansystolic at lower left sternal edge, increases with inspiration - Carvallo's sign)
- Listen in multiple positions (left lateral decubitus for mitral; sitting forward for aortic)
- Elevated JVP
- Bibasal crackles (pulmonary oedema)
- S3 gallop
- Peripheral oedema
- Heart failure in an IE patient = urgent surgical assessment needed
Abdomen
- Present in 10-40% of cases
- More common in subacute IE (weeks of infection)
- Left upper quadrant tenderness may indicate splenic infarction or abscess
- Tender spleen with fever = do CT abdomen
Neurological Examination
- Focal neurological deficit (hemiplegia, aphasia, field defect) → septic embolic stroke
- Cranial nerve palsies
- Visual field defects
- Altered mental status / delirium (toxic-metabolic encephalopathy)
- Meningism (rare - suggests mycotic aneurysm rupture or meningitis)
- Always document a baseline neurological examination
Musculoskeletal
- Joint swelling/tenderness (immune complex arthritis or septic arthritis from emboli)
- Back tenderness → vertebral osteomyelitis (IE can seed vertebral bodies; always examine spine)
- Psoas tenderness/hip pain → psoas abscess
Other
- Dental examination: Poor dentition, gum disease - source identification
- Catheter/line sites: Healthcare-associated IE - look at CVC, peripheral lines, pacemaker pocket
- IVDU signs: Track marks at antecubital fossa, forearms, groins, feet
Part 4: The Modified Duke Criteria - Your Diagnostic Framework
MAJOR Criteria (2 major = Definite IE)
- Typical organism (viridans streptococci, S. aureus, Streptococcus gallolyticus, HACEK organisms, community-acquired Enterococcus) in 2 separate blood cultures OR
- Persistent bacteremia with ANY organism: ≥2 cultures >12 hours apart, OR ≥3 cultures, OR majority of ≥4 cultures >1 hour apart
- Echo findings: Oscillating/mobile mass on valve or supporting structure (vegetation), abscess, new partial dehiscence of prosthetic valve OR
- New valvular regurgitation (new murmur)
MINOR Criteria
- Predisposing condition (IVDU or predisposing cardiac lesion)
- Fever ≥38°C
- Vascular phenomena: Arterial emboli, septic pulmonary emboli, mycotic aneurysm, intracranial haemorrhage, conjunctival haemorrhages, Janeway lesions
- Immunologic phenomena: Glomerulonephritis, Osler nodes, Roth spots, rheumatoid factor
- Echo findings consistent with IE but not meeting major criterion
- Microbiologic evidence not meeting major criterion
Classification:
| Category | Definition |
|---|---|
| Definite IE | 2 Major OR 1 Major + 3 Minor OR 5 Minor |
| Possible IE | 1 Major + 1 Minor OR 3 Minor |
| Rejected | Firm alternative diagnosis OR resolution with ≤4 days antibiotics |
- Fever ≥38°C (1 minor)
- Predisposing cardiac condition or risk factor (1 minor)
- Splinter haemorrhages / Osler nodes / Janeway lesions (vascular/immunologic: 1 minor each)
- This could already constitute "Possible IE" (3 minor criteria) - enough to start workup urgently.
Part 5: Investigations
Blood Cultures - The Single Most Important Test
- Draw at least 3 sets (each = 1 aerobic + 1 anaerobic bottle) from 3 separate venepuncture sites
- Draw them at least 1 hour apart (documents continuous bacteraemia, a hallmark of IE)
- If critically ill: all 3 sets within 30 minutes without delay
- Do NOT start antibiotics before drawing blood cultures (reduces sensitivity by ~30%)
- Incubate for at least 5 days (HACEK organisms grow slowly)
- Label with time, site, and patient details meticulously
Echocardiography
- Transthoracic Echo (TTE): First investigation; 60-80% sensitivity for native valve vegetations
- Transoesophageal Echo (TOE/TEE): 90-100% sensitivity; preferred for prosthetic valves, poor TTE windows, suspected abscess, negative TTE with high suspicion
- Look for: vegetations (oscillating mass on valve), abscess (perivalvular), new regurgitation, leaflet perforation, prosthetic valve dehiscence
Basic Blood Tests
| Test | Expected Finding in IE |
|---|---|
| FBC | Normocytic normochromic anaemia (very common); leucocytosis (acute IE), normal WBC (subacute) |
| ESR | Elevated (61% of cases) |
| CRP | Markedly elevated |
| Serum creatinine | Elevated if embolic nephritis or immune-complex glomerulonephritis |
| Urine dipstick/microscopy | Haematuria (microscopic) + proteinuria → immune complex GN |
| Rheumatoid factor | Positive in up to 50% of subacute IE (minor Duke criterion) |
| LFT | Mildly elevated in sepsis; useful baseline |
| Troponin | Elevated if mycotic coronary embolism or myocarditis |
ECG
- New conduction defects (PR prolongation, new bundle branch block, complete heart block) → perivalvular abscess extending to conduction system - a serious complication requiring urgent surgery
- Check daily in confirmed IE
Imaging (if available)
- CT chest/abdomen/pelvis: Identify embolic complications (splenic/renal/cerebral infarcts, pulmonary septic emboli in right-sided IE)
- MRI brain: Detect clinically silent cerebral emboli (present in up to 80% of IE at autopsy)
- X-ray chest: Pulmonary infiltrates/septic emboli (right-sided IE)
Part 6: Common Causative Organisms and Clinical Clues
| Organism | Clinical Context | Course |
|---|---|---|
| Viridans streptococci (S. mutans, S. sanguinis, S. mitis) | Dental procedures, poor dentition, native valve | Subacute - weeks of symptoms |
| Streptococcus gallolyticus (S. bovis) | Colon cancer/polyps - order colonoscopy | Subacute |
| Staphylococcus aureus | IVDU, healthcare contact, skin/soft tissue source, CVC | Acute - days of severe illness |
| Enterococcus faecalis | GI/GU procedures, elderly, urinary tract source | Subacute |
| HACEK organisms (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) | Dental/oral flora, slow-growing, culture-negative initially | Subacute |
| Coagulase-negative staphylococci | Prosthetic valve (early <2 months post-surgery) | Variable |
| Candida/Aspergillus (Fungal) | IVDU, prolonged antibiotics, TPN, immunocompromised | Subacute, large vegetations |
| Coxiella burnetii (Q fever) | Farm/animal exposure, often culture-negative | Subacute, positive serology |
Important clinical pearl: S. gallolyticus bacteraemia or IE should prompt colonoscopy - there is a strong association with colorectal adenoma/carcinoma.
Part 7: Complications to Identify
| Complication | Clinical Sign | Action |
|---|---|---|
| Heart failure (most common cause of death) | New/worsening dyspnoea, pulmonary oedema, S3 | Urgent surgery consultation |
| Perivalvular abscess | New conduction defect on ECG, fever persisting despite antibiotics | TOE urgent, cardiac surgery |
| Embolic stroke | New focal neurological deficit | CT/MRI brain; anticoagulation is NOT routinely given; surgery before stroke if emboli size increasing |
| Mycotic aneurysm | Severe headache, neck stiffness, neurological deterioration | CT angiography head |
| Splenic abscess | LUQ pain, persistent fever despite appropriate antibiotics | CT abdomen; drainage or splenectomy |
| Septic pulmonary emboli (right-sided IE) | Haemoptysis, pleuritic pain, chest X-ray nodules | Manage right-sided IE (often conservative) |
| Acute renal failure | Rising creatinine, haematuria | Embolic infarction vs immune complex GN; supportive care |
| Vertebral osteomyelitis | Back pain, spinal tenderness | MRI spine |
Part 8: Empirical Antibiotic Treatment (Once Blood Cultures Drawn)
Empirical Treatment (Before Culture Results):
Ampicillin-sulbactam 12 g/day IV (in divided doses) + Gentamicin 3 mg/kg/day IV (divided 8-hourly)
Vancomycin 30 mg/kg/day IV (in 2 divided doses) + Gentamicin 3 mg/kg/day
Vancomycin 30 mg/kg/day IV ± Gentamicin
Targeted Treatment by Organism:
| Organism | Antibiotic | Duration |
|---|---|---|
| Viridans streptococci (penicillin-sensitive) | Benzylpenicillin G 12-18 million units/day IV ± gentamicin | 4-6 weeks (2 weeks if uncomplicated + gentamicin combination) |
| S. aureus (MSSA) - native valve | Flucloxacillin/nafcillin 12 g/day IV | 6 weeks |
| S. aureus (MRSA) | Vancomycin 30 mg/kg/day IV | 6 weeks |
| Enterococcus | Ampicillin 12 g/day + Gentamicin 3 mg/kg/day | 4-6 weeks |
| HACEK | Ceftriaxone 2 g/day IV | 4 weeks |
| Prosthetic valve IE (any organism) | As above + Rifampicin 900 mg/day PO (after 3-5 days) | 6 weeks minimum |
Surgical Indications (When Medical Treatment Is Not Enough):
- Heart failure from severe valve regurgitation (most common indication)
- Perivalvular abscess, fistula, or destructive penetrating lesion
- Persistent fever/bacteraemia despite 7-10 days appropriate antibiotics
- Large mobile vegetation (>10 mm) with recurrent emboli despite antibiotics
- Fungal endocarditis
- Prosthetic valve IE caused by S. aureus (most require surgery)
Quick IE Suspicion Checklist at the Bedside
- Does the patient have a cardiac valve lesion, prosthetic valve, or IVDU history?
- Is there a new or changing heart murmur?
- Are there splinter haemorrhages in proximal nail beds?
- Osler's nodes (tender nodules on fingertips/toe pads)?
- Janeway lesions (painless spots on palms/soles)?
- Petechiae on conjunctiva, palate, or skin?
- Splenomegaly?
- Any embolic event (stroke, flank pain, back pain)?
- Haematuria on dipstick?
- Any recent procedure that could cause bacteraemia (dental, urological, GI)?
- Goldman-Cecil Medicine, Table 61-2 (Physical Findings in IE), Table 61-3 (Modified Duke Criteria)
- Braunwald's Heart Disease, Table 80.1 (Symptoms), Table 80.2 (Physical Findings)
- Frameworks for Internal Medicine, Infective Endocarditis chapter
- Jawetz, Melnick & Adelberg's Medical Microbiology - Antibiotic therapy for IE
How to treat a patient with chronic kidney disease and fluid overload and severe shortness of breath, given furosemide 80mg 3 times daily. What can be done in an emergency to decrease his shortness of breath even when his urine output is about nil? Isosorbide dinitirite is also given at a low dose what other measures can be done. What investigations are to be done for further calling our dialysis?
"acute pulmonary edema" AND "renal failure" AND "treatment"
CKD with Refractory Fluid Overload, Near-Anuria, and Acute Dyspnoea - Emergency Management and Dialysis Decision
Understanding the Problem - Why Furosemide 80mg TDS Is Not Working
- Reduced nephron mass means fewer tubular cells to respond to furosemide
- Furosemide works by being secreted into the tubular lumen via organic acid transporters - in uraemia, accumulated organic acids competitively block this secretion
- Hypoalbuminaemia (very common in CKD) means furosemide remains protein-bound in plasma and cannot reach the tubule
- Sodium avidity - the remaining nephrons avidly reabsorb sodium, overcoming furosemide's effect
- With near-zero urine output, oral/IV furosemide simply cannot remove the fluid burden
Part 1: Immediate Emergency Management - The First 30 Minutes
STOP and THINK: The "LMNOP" Mnemonic for Acute Pulmonary Oedema
M - Morphine - IV for venodilation and anxiety relief
N - Nitrates - Escalate isosorbide dinitrate
O - Oxygen - High flow + non-invasive ventilation
P - Position - Sit the patient upright
Step 1 - Position and Oxygen (IMMEDIATE, within 2 minutes)
- Sit the patient upright at 90° (high Fowler's position) - this alone reduces venous return to the lungs by 30-40% via hydrostatic redistribution of fluid to dependent areas
- Dangle legs over the bedside if possible (further reduces preload)
- High-flow oxygen: 10-15L/min via non-rebreather mask; target SpO₂ ≥94-96%
- Do NOT give oxygen at >96% in known chronic hypercapnic COPD patients - but in pure fluid overload without COPD, high-flow oxygen is appropriate
- IV access × 2, continuous monitoring (ECG, SpO₂, BP, RR)
Step 2 - Escalate Nitrates (Most Effective Drug in This Situation)
- If already on low-dose isosorbide dinitrate orally → Switch to IV glyceryl trinitrate (GTN) / nitroglycerin
- GTN infusion: Start at 10-20 mcg/min IV, titrate up every 5-10 minutes by 10 mcg/min
- Can go up to 200-400 mcg/min if BP tolerates (keep SBP >100 mmHg)
- Sublingual GTN 0.4 mg (or isosorbide dinitrate 5mg SL) can be given while setting up IV - works within 2-3 minutes
- Contraindications: SBP <90 mmHg, use of PDE-5 inhibitors (sildenafil, tadalafil) within 24-48 hours, hypertrophic obstructive cardiomyopathy
Step 3 - Non-Invasive Ventilation (NIV) - Most Powerful Non-Pharmacological Intervention
- Start at 5-7.5 cmH₂O, increase to 10-12.5 cmH₂O
- Keeps alveoli open, prevents alveolar flooding, improves oxygenation
- First choice in pure fluid overload without respiratory muscle failure
- IPAP 12-16 cmH₂O, EPAP 4-8 cmH₂O
- Better if CO₂ is rising (combined respiratory failure)
- Use if CPAP alone insufficient
Step 4 - Morphine (Use Cautiously in Renal Failure)
- 2-5 mg IV slowly - causes venodilation + anxiolysis + reduces the work of breathing sensation
- CAUTION in CKD: Morphine metabolite (morphine-6-glucuronide) accumulates in renal failure → respiratory depression
- Use only if patient is very distressed AND blood pressure is adequate
- Consider low-dose diamorphine (1-2.5 mg IV) as alternative
- Have naloxone ready
Step 5 - Maximise/Escalate Diuretic Strategy
- Oral furosemide bioavailability is only 40-60% in heart failure/CKD (gut oedema reduces absorption)
- IV furosemide is 2× more potent than the same oral dose
- If on 80mg oral TDS → equivalent to giving 40mg IV TDS
- Bolus: 200 mg IV furosemide (yes - high doses are needed in anuric CKD)
- Then: Continuous IV infusion 20-40 mg/hour
- Continuous infusion produces more sustained natriuresis than bolus dosing in diuretic resistance
Metolazone 2.5-5 mg orally 30 minutes BEFORE furosemide
-
This is the classic "sequential nephron blockade" - blocks the distal tubule AND the loop simultaneously
-
Furosemide blocks the loop of Henle; thiazides block the distal convoluted tubule
-
When combined, sodium that "escapes" furosemide's effect is blocked downstream
-
Dramatically increases urine output even in patients previously unresponsive to furosemide alone
-
Start with 2.5 mg metolazone once daily to assess response; can increase to 10 mg
-
Alternative: Hydrochlorothiazide 25-50 mg or Chlorothiazide 500 mg IV (if oral route problematic)
- Spironolactone 25-50 mg blocks aldosterone-driven distal sodium reabsorption
- Caution: Risk of hyperkalaemia in CKD - check K+ first; avoid if K+ >5.5 mmol/L
- Carbonic anhydrase inhibitor - blocks proximal tubular sodium reabsorption
- 500 mg IV daily alongside furosemide (ADVOR trial showed benefit)
- Practical in CKD and may enhance loop diuretic response
Step 6 - Sodium and Fluid Restriction
- Strict fluid restriction: 500-750 mL/24 hours (input - all sources including IV medications, feeds)
- Sodium restriction: <2g sodium/day (no added salt diet)
- Stop all unnecessary IV fluids (D5W, 0.9% saline flushes, etc.)
- Concentrated IV medications (give in minimum volume)
Step 7 - Stop Nephrotoxic and Sodium-Retaining Drugs
- NSAIDs (ibuprofen, diclofenac, naproxen, ketorolac) - worsen renal function and cause sodium retention
- ACE inhibitors/ARBs - consider temporary hold if creatinine rising sharply (may be worsening renal perfusion)
- Contrast-containing medications
- Metformin (accumulates in renal failure → lactic acidosis)
- Potassium-sparing agents if K+ already high
Part 2: Emergency Measures That Work Without Kidney Function (The "Renal-Independent" Toolkit)
1. Non-Invasive Ventilation (CPAP/BiPAP) - already covered above
2. Venesection / Therapeutic Phlebotomy (Resource-Limited Settings)
- Remove 250-500 mL of blood from a large peripheral or central vein
- Immediately reduces preload and pulmonary congestion
- Indicated when:
- No other means of fluid removal available
- Patient haemodynamically stable enough (SBP >110)
- Emergency bridge to dialysis
- Not done if patient is anaemic (Hb <8 g/dL)
- A historical technique still valid in resource-limited settings
3. Rotating Tourniquets (Historical; Rarely Used Now)
- Apply BP cuffs to 3 of 4 limbs, inflate to mid-diastolic pressure
- Rotates every 15 minutes (one limb free at a time)
- Traps venous blood in peripheral vasculature, reduces preload
- Labour-intensive; largely replaced by NIV and nitrates
4. Inotropes (if Cardiogenic Component Contributing)
- If the fluid overload is partly from low cardiac output (heart not pumping well):
- Dobutamine 2-10 mcg/kg/min IV → improves cardiac output → better renal perfusion → may improve diuretic response
- Only if hypotensive or low-output state suspected
5. Ultrafiltration (if available)
- Isolated ultrafiltration can be done even without full dialysis setup
- Removes 100-300 mL/hour of pure water
- Available in nephrology units with basic equipment
- The most effective bridge when diuretics fail and dialysis not yet started
Part 3: Preparing for Dialysis - What Investigations Are Needed
Investigations Required Before Initiating Dialysis
Immediate Bloods (Within 1 Hour)
| Test | What You Are Looking For |
|---|---|
| Serum potassium (K+) | Hyperkalaemia >6.5 mmol/L = emergency indication for dialysis |
| Serum creatinine + eGFR | Quantify renal function; trend over days |
| Blood urea nitrogen (BUN/urea) | Uraemia (urea >35-40 mmol/L = symptomatic threshold); serum urea >50 mmol/L with symptoms = urgent dialysis |
| Arterial blood gas | pH <7.1 or bicarbonate <12 mmol/L = severe metabolic acidosis → urgent dialysis |
| Serum bicarbonate | If <15 mmol/L, dialysis indicated even without other criteria |
| Serum sodium | Hypo or hypernatraemia affecting treatment approach |
| Serum phosphate | Elevated in CKD; causes vascular calcification |
| Serum calcium | Hypocalcaemia (common in CKD); hyperkalaemia treatment (calcium gluconate) |
| Serum albumin | Hypoalbuminaemia worsens oedema; nutritional status |
| Lactate | >4 mmol/L = tissue hypoxia, critical illness severity |
| FBC | Anaemia (uraemic anaemia), leucocytosis (infection), thrombocytopenia |
| Coagulation (PT, aPTT) | Uraemic coagulopathy |
| LFT + total bilirubin | Rule out hepatic cause of oedema; assess for hepatorenal |
| Blood cultures × 2 | Before inserting dialysis catheter; rule out sepsis as precipitant |
| Serum uric acid | Gouty nephropathy; also marker of cell turnover |
| HbA1c | If diabetic nephropathy suspected |
| Troponin + ECG | Rule out ACS precipitating acute decompensation |
| CXR (chest) | Pulmonary oedema severity; cardiac size; rule out infection |
Investigations for Dialysis Planning
| Test | Purpose |
|---|---|
| Renal ultrasound | Kidney size (small, echogenic = chronic CKD; normal size = AKI or AKI-on-CKD); obstruction (hydronephrosis - must rule out!); asymmetry (renovascular disease) |
| ECG (12-lead) | Hyperkalaemic changes (peaked T waves, widened QRS, sine wave - emergency); arrhythmias; pericarditis (uraemic pericarditis - friction rub = urgent dialysis) |
| Echocardiogram | LV function (cardiorenal syndrome type); pericardial effusion (uraemic); valvular disease; uraemic cardiomyopathy |
| Urine protein:creatinine ratio | Quantify proteinuria (even small volumes); nephrotic syndrome assessment |
| Urine microscopy | Red cell casts (GN), granular casts (AKI), renal tubular cells (ATN) |
| Urine sodium | <20 mmol/L = pre-renal; >40 mmol/L = intrinsic renal failure |
| Serology (if not known CKD aetiology): ANA, ANCA, Anti-GBM, complement (C3, C4), Anti-dsDNA, hepatitis B/C serology, HIV | Glomerulonephritis workup; secondary causes of CKD |
| Hepatitis B, C, HIV | Mandatory before dialysis (infection control; antiviral prophylaxis) |
| Parathyroid hormone (PTH) | Secondary hyperparathyroidism in CKD; renal osteodystrophy |
| Serum iron, TIBC, ferritin | Uraemic anaemia; iron deficiency (for EPO therapy planning) |
| Chest X-ray | Before inserting any central access; baseline cardiothoracic ratio |
| Vascular access assessment | Doppler of arm vessels if AV fistula planned; avoid peripheral cannulae in non-dominant arm (preserve vascular access) |
The AEIOU Indications for Emergency Dialysis
| Letter | Indication | Threshold |
|---|---|---|
| A - Acidosis | Metabolic acidosis refractory to medical management | pH <7.1 or bicarbonate <12 mmol/L |
| E - Electrolytes | Hyperkalaemia unresponsive to medical treatment | K+ >6.5 with ECG changes, or K+ >7.0 regardless |
| I - Intoxication | Dialysable toxins/drugs (lithium, salicylates, methanol, ethylene glycol) | Any severe toxicity |
| O - Overload | Fluid overload refractory to diuretics causing respiratory failure | Your patient's situation - this is an indication for emergency dialysis |
| U - Uraemia | Symptomatic uraemia | Pericarditis, uraemic encephalopathy, uraemic bleeding, nausea/vomiting |
Part 4: Types of Renal Replacement Therapy - Choose What Is Available
Haemodialysis (HD)
- Standard intermittent HD: 4-hour sessions, 3-4 times/week
- Best for rapid electrolyte correction and fluid removal
- Requires stable haemodynamics (can drop BP)
- Continuous ambulatory peritoneal dialysis (CAPD) as alternative if available
Peritoneal Dialysis (PD) - Important in Resource-Limited Settings
- Can be started emergently with an acute PD catheter (Tenckhoff or rigid PD catheter)
- Does NOT require haemodialysis machine
- Gentle, continuous fluid removal - good for haemodynamically unstable patients
- Avoid if: recent abdominal surgery, peritonitis, abdominal adhesions, diaphragmatic defects
- Highly relevant in resource-limited settings where HD machines are unavailable
Continuous Renal Replacement Therapy (CRRT)
- Continuous veno-venous haemofiltration (CVVHF) or haemodiafiltration (CVVHDF)
- Best for haemodynamically unstable ICU patients
- Gentle, continuous fluid removal (100-300 mL/hour)
- Requires ICU, trained staff, specialised equipment
Part 5: While Preparing for Dialysis - Emergency Treatment of Hyperkalaemia (If Present)
Stepwise Treatment:
Calcium gluconate 10% - 10-20 mL (1-2 ampoules) IV over 5-10 minutes (or calcium chloride 10% - 6.8 mL)
- Works within 1-3 minutes; lasts 30-60 minutes
- Does NOT lower K+ - only protects the heart from arrhythmia
Insulin + Dextrose: 10 units soluble insulin IV + 50 mL 50% dextrose (or 125 mL 20% dextrose) IV
- Lowers K+ by 0.5-1.5 mmol/L; lasts 4-6 hours
Salbutamol (albuterol) 10-20 mg nebulised (can also be given IV)
- Lowers K+ by 0.5-1 mmol/L; works within 30 minutes
- Especially useful as it also treats bronchospasm from fluid overload
- Contraindicated in tachyarrhythmias
Sodium bicarbonate 8.4% - 50-100 mL IV if pH <7.2
- Shifts K+ intracellularly; also treats acidosis
Calcium resonium (sodium polystyrene sulphonate) 15g oral/rectal
- Slow K+ removal via GI tract (hours-days)
- Less effective in acute emergency
Patiromer or Sodium Zirconium Cyclosilicate (ZS-9) if available
- Newer K+ binders, more rapid and reliable than calcium resonium
Part 6: Full Management Summary (Checklist Format)
In the First 15 Minutes:
- Sit patient upright at 90°, legs dependent
- High-flow oxygen 10-15 L/min NRM; target SpO₂ 94-98%
- IV access × 2 (avoid antecubital fossa/forearm of non-dominant arm - preserve for AV fistula)
- Continuous monitoring: ECG, SpO₂, BP every 5 minutes
- Sublingual GTN 0.4 mg (or isosorbide dinitrate 5 mg SL) immediately
- Start NIV: CPAP 7.5-10 cmH₂O (or BiPAP if hypercapnic)
- Urgent bloods: K+, creatinine, urea, ABG, FBC, troponin, LFT
- 12-lead ECG immediately (rule out ACS + check for hyperkalaemia changes)
- Catheterise patient (accurate hourly urine measurement)
In the First Hour:
- IV GTN infusion at 20 mcg/min, titrate up (keep SBP >100)
- IV furosemide 200 mg bolus (or continuous infusion 20-40 mg/hour)
- Add metolazone 5 mg oral (sequential nephron blockade) - give 30 minutes before furosemide
- If hyperkalaemia (K+ >6.0 + ECG changes): calcium gluconate + insulin/dextrose immediately
- Strict fluid restriction: 500 mL/24h input only
- Stop all NSAIDs, nephrotoxins, unnecessary IV fluids
- CXR (portable)
- Morphine 2 mg IV (if still severely distressed, SpO₂ maintained, not hypercapnic)
In the First 4-6 Hours (While Awaiting Dialysis):
- Repeat K+, creatinine, ABG after 2-4 hours
- Renal ultrasound (rule out obstruction - easily missed and treatable!)
- Nephrology consultation for emergency dialysis
- Hepatitis B/C, HIV testing (mandatory before dialysis)
- Blood cultures before any central line placement
- Assess for uraemic pericarditis (listen for friction rub), encephalopathy, bleeding
- Echocardiogram if available (cardiac function, pericardial effusion)
- Insert temporary dialysis catheter (internal jugular or femoral vein) and commence dialysis/ultrafiltration
Key Messages to Remember
-
In an anuric CKD patient with pulmonary oedema - nitrates and NIV are your most powerful immediate tools, not diuretics. Don't waste time waiting for diuretic response that won't come.
-
Metolazone + furosemide (sequential nephron blockade) is the most effective oral combination to break diuretic resistance - always try this before abandoning medical therapy.
-
"AEIOU" - your patient meets "O" (overload) for emergency dialysis. Check for A (acidosis) and E (electrolytes - K+) which may be present simultaneously.
-
Always do renal ultrasound first - obstructive uropathy (bilateral hydronephrosis, full bladder) is the one completely reversible cause of oliguria/anuria that is easily missed and easily fixed with a catheter or nephrostomy.
-
In resource-limited settings: peritoneal dialysis is a valid and immediately available alternative to haemodialysis - it does not require a machine, can remove fluid gently, and can be life-saving.
-
Preserve vascular access - avoid cannulae in the forearm/antecubital of the non-dominant arm; this is the site for a future AV fistula.