Management for Coronary artery disease drugs
Reading File
Finding Sources
Searching PubMed
"coronary artery disease"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
coronary artery disease pharmacological management guidelines 2024 2025 ACC AHA
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full, well-organized response:
Pharmacological Management of Coronary Artery Disease (CAD)
CAD management is divided into two goals: (1) symptom relief (antianginal drugs) and (2) prognosis improvement (preventing MI, death, and progression). The approach also differs between chronic/stable CAD and acute coronary syndromes (ACS).
A. Drugs for Prognosis (Reduce MI, Death, Stroke)
1. Antiplatelet Agents
Aspirin (acetylsalicylic acid)
- Low-dose aspirin (75-100 mg/day) is the cornerstone antiplatelet for all CAD patients.
- Irreversibly inhibits COX-1, reducing thromboxane A2-mediated platelet aggregation.
- Reduces risk of MI and cardiovascular death in stable CAD.
P2Y12 Inhibitors (for ACS and post-PCI)
Dual antiplatelet therapy (DAPT) = Aspirin + a P2Y12 inhibitor is standard after ACS or PCI.
| Drug | Class | Notes |
|---|---|---|
| Clopidogrel | Thienopyridine (prodrug) | Standard for stable CAD, after PCI; requires hepatic activation |
| Ticagrelor | Cyclopentyltriazolopyrimidine | Faster onset, more potent; preferred in ACS (PLATO trial) |
| Prasugrel | Thienopyridine (prodrug) | Most potent; used in PCI for ACS; avoid in prior stroke/TIA |
- DAPT duration after drug-eluting stent: minimum 6-12 months; may extend to 12+ months in high-ischemic/low-bleeding risk patients.
- A 2025 meta-analysis (PMID: 40467090) confirms P2Y12 inhibitor monotherapy after PCI is non-inferior to aspirin monotherapy for some outcomes post-DAPT.
Glycoprotein IIb/IIIa Inhibitors (eptifibatide, tirofiban, abciximab)
- Used IV in high-risk ACS/PCI settings; block the final common pathway of platelet aggregation.
2. Statins (HMG-CoA Reductase Inhibitors)
- High-intensity statins (atorvastatin 40-80 mg, rosuvastatin 20-40 mg) are indicated for ALL CAD patients, regardless of baseline LDL-C.
- Goal: LDL-C <1.4 mmol/L (<55 mg/dL) with ≥50% reduction from baseline (European guidelines); high-intensity statin therapy for all (US/ACC/AHA approach).
- In patients with recurrent events within 2 years despite max statin, LDL-C goal <1.0 mmol/L (<40 mg/dL).
- Benefit: plaque stabilization, anti-inflammatory effects, mortality reduction.
Add-on lipid-lowering agents (if LDL goal not met):
- Ezetimibe (10 mg/day): inhibits intestinal cholesterol absorption; IMPROVE-IT trial showed 6.4% relative risk reduction in composite CV events added to statin in post-ACS patients.
- PCSK9 inhibitors (evolocumab, alirocumab): monoclonal antibodies; FOURIER trial showed 15% relative reduction in CV events vs. placebo in patients on max-dose statin; initiated 8-12 weeks after event if LDL goal not met.
3. Beta-Blockers (β-Adrenergic Antagonists)
- Mechanism: Reduce heart rate, myocardial contractility, and oxygen demand; also antiarrhythmic.
- Indicated: All post-MI patients, especially with LVEF ≤40% or HF (Class I, LOE A).
- For LVEF >40%: Recommended routinely after MI (Class IIa).
- IV Metoprolol: IV then oral in hemodynamically stable STEMI patients undergoing primary PCI (Class IIa). Metoprolol is the IV beta-blocker of choice (unique cardioprotective effect on β1 receptor).
- Carvedilol: Proven mortality reduction in post-MI patients with reduced LVEF (CAPRICORN trial).
- For stable angina: beta-blockers are first-line antianginal AND prognostic agents.
4. ACE Inhibitors / ARBs / ARNi
ACE Inhibitors (ramipril, lisinopril, enalapril, perindopril)
- Indicated (Class I): Post-MI with HF, LV systolic dysfunction (LVEF ≤40%), diabetes, or anterior infarct.
- Should be started within 24 hours of STEMI in the absence of contraindications (hypotension, hypersensitivity, pregnancy).
- Consider (Class IIa) in ALL post-MI patients without contraindications.
ARBs (valsartan, candesartan)
- Alternative when ACE inhibitors are not tolerated (VALIANT trial for valsartan).
Mineralocorticoid Receptor Antagonists (MRA) - eplerenone, spironolactone
- Added on top of ACE inhibitor + beta-blocker in post-MI patients with LVEF ≤40% AND HF or diabetes (EPHESUS trial).
- Reduces CV mortality and hospitalization.
- Contraindicated if serum creatinine >2.5 mg/dL (men) or >2.0 mg/dL (women), or K+ >5.0 mEq/L.
B. Antianginal Drugs (Symptom Relief)
5. Nitrates
| Drug | Route | Duration | Use |
|---|---|---|---|
| Sublingual nitroglycerin | SL tablet/spray | 3-5 min onset | Acute angina relief |
| Isosorbide dinitrate | Oral | Intermediate | Prophylaxis |
| Isosorbide mononitrate | Oral | Long-acting | Prophylaxis |
| GTN patch | Transdermal | 24h | Prophylaxis |
- Mechanism: Release NO → venodilation → reduced preload → reduced myocardial O2 demand; also coronary vasodilation.
- Tolerance: Nitrate-free interval of 8-12 hours required to avoid tolerance.
- Contraindication: Absolutely contraindicated with PDE5 inhibitors (sildenafil, tadalafil) - risk of severe hypotension; do not use within 24-48 hours.
- Nitrates relieve angina but have not been shown to reduce mortality as monotherapy in CAD.
6. Calcium Channel Blockers (CCBs)
Dihydropyridines (amlodipine, nifedipine, felodipine)
- Primarily vasodilators; reduce afterload.
- Amlodipine: commonly used, well tolerated, also reduces angina frequency.
- Nifedipine immediate-release: avoid as monotherapy in unstable angina (reflex tachycardia).
Non-dihydropyridines (diltiazem, verapamil)
- Reduce heart rate AND vasodilate - useful when beta-blockers are contraindicated.
- Avoid in HF with reduced LVEF (negative inotrope).
- Verapamil: most negative chronotropic/inotropic.
7. Ivabradine
- Mechanism: Selectively inhibits the If (funny) current in the sinoatrial node - pure heart rate reduction without negative inotropy or vasodilation.
- Indicated for stable angina in sinus rhythm when beta-blockers are contraindicated or poorly tolerated, or as add-on.
- Also used in HF with reduced EF + resting HR ≥70 bpm on maximum tolerated beta-blocker.
8. Ranolazine
- Mechanism: Inhibits late inward sodium current (INa) → reduces intracellular Ca2+ → reduces myocardial oxygen demand; no significant effect on HR or BP.
- Used as add-on antianginal therapy in patients inadequately controlled on beta-blockers and/or CCBs.
- Available in some countries; CARISA trial showed improved exercise tolerance when added to atenolol, amlodipine, or diltiazem.
9. Other Antianginal Agents
- Nicorandil: Potassium channel opener + nitrate-like effect; reduces both preload and afterload; available in Europe and Asia; not US.
- Trimetazidine: Metabolic agent (inhibits fatty acid oxidation, favors glucose metabolism); used in some countries as add-on; safety in HF uncertain.
- Molsidomine: Nitric oxide donor; alternative to nitrates.
C. Anticoagulants in ACS
| Drug | Setting |
|---|---|
| Unfractionated heparin (UFH) | Most common during PCI for STEMI (70-100 U/kg bolus) |
| Enoxaparin (LMWH) | Alternative to UFH; more predictable; preferred in NSTEMI medical management |
| Bivalirudin (direct thrombin inhibitor) | Alternative in patients with heparin-induced thrombocytopenia |
| Fondaparinux | NOT recommended as sole anticoagulant during primary PCI (excess catheter thrombosis) |
D. Drug Overview by CAD Setting
Stable Chronic CAD
| Drug Class | Purpose |
|---|---|
| Aspirin 75-100 mg/day | Antiplatelet, prognosis |
| High-intensity statin | LDL lowering, plaque stabilization |
| Beta-blocker | Antianginal + prognostic post-MI |
| ACE inhibitor | Prognostic (esp. if EF reduced, DM, HTN) |
| Nitrates (SL PRN) | Acute angina relief |
| CCB or Ivabradine | Add-on antianginal if beta-blocker insufficient |
Acute Coronary Syndrome (STEMI / NSTEMI-UA)
| Drug | Role |
|---|---|
| DAPT (Aspirin + Ticagrelor or Prasugrel) | Antiplatelet x 12 months |
| Anticoagulant (UFH/Enoxaparin) | Acute antithrombotic |
| IV Metoprolol → oral beta-blocker | Rate control, cardioprotection |
| High-intensity statin (early, Day 1) | LDL goal, plaque stabilization |
| ACE inhibitor / ARB | RAAS blockade (24h if EF ↓ or anterior MI) |
| MRA (eplerenone) | If EF ≤40% + HF or DM |
| Ezetimibe / PCSK9i | If LDL target not met at 4-6 weeks |
E. STEMI Pharmacological Timeline
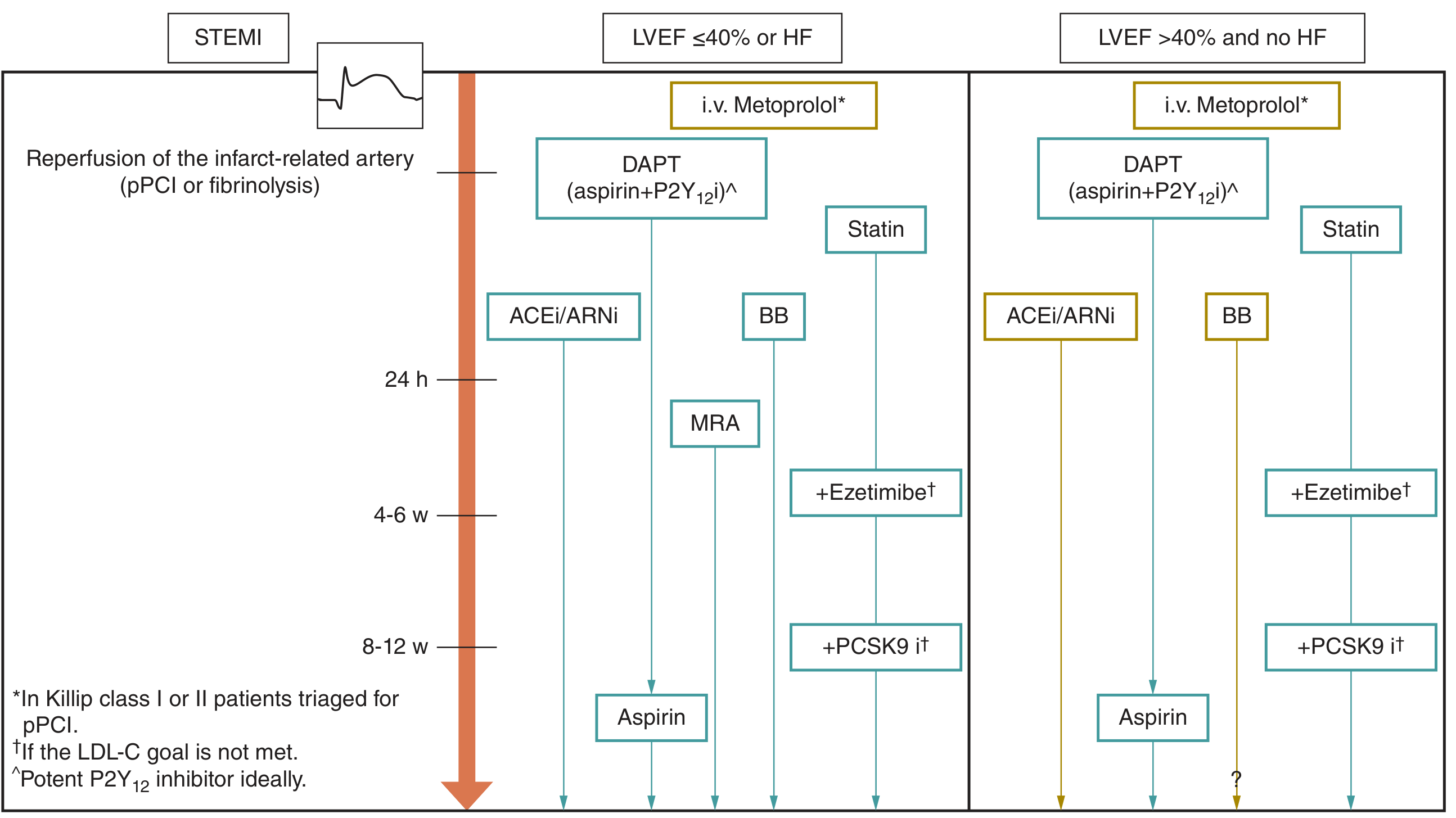
Recent Evidence Updates (2024-2025)
- PMID 39567875 (2024): Low/moderate statin + ezetimibe combination is comparable in safety and efficacy to high-intensity statin monotherapy - a consideration for statin-intolerant patients.
- PMID 39918465 (2025, JACC): In AF + stable CAD, anticoagulation alone (without antiplatelet) is generally preferred after PCI; combination therapy increases bleeding.
- PMID 40467090 (2025, BMJ): P2Y12 inhibitor monotherapy after PCI is superior to aspirin monotherapy for reducing MACE - may change post-DAPT strategy.
- 2025 ACC/AHA ACS Guideline (PMID 40014670): Updated comprehensive guideline replacing 2013 STEMI and 2014 NSTEMI guidelines.
Sources: Fuster and Hurst's The Heart, 15th Ed. | Goldman-Cecil Medicine | Fuster & Hurst's Heart (Cardiovascular Medicine)
Evaluate these hand writ notes and explain me everything
Reading File
Running Command
Excellent - I've extracted all 30 pages. These are polyclinic/clinical notes from a medical student (Sonya Chawla) covering multiple topics taught by different professors. Let me now provide a thorough explanation of everything covered in these notes.
Sonya Chawla - Polyclinic Notes: Full Explanation
These are 30 pages of clinical polyclinic notes covering 6 major topics across multiple teaching sessions. Here is everything explained clearly and systematically.
📘 TOPIC 1: DIABETES MELLITUS (Days 1, 2 & 10)
1.1 Diagnosis of Diabetes
| Test | Value | Interpretation |
|---|---|---|
| Fasting plasma glucose | < 6.1 mmol/L | Normal |
| Fasting plasma glucose | 6.1-6.9 mmol/L | Pre-diabetes (impaired fasting glucose) |
| Fasting plasma glucose | ≥ 7.0 mmol/L | Diabetes |
| Postprandial (2h) glucose | ≥ 11.1 mmol/L or ≥ 200 mg/dL | Diabetes |
| HbA1c | < 5.6% | Normal |
| HbA1c | 5.6 - 6.4% | Pre-diabetes |
| HbA1c | ≥ 6.5% | Diabetes |
| Capillary glucose | 5.5 mmol/L (baseline) | Normal reference |
- Glucometer - NOT used for diagnosis; only used for monitoring/control
- HbA1c - reflects average blood glucose over the last 2-3 months (lifespan of RBC = 120 days); it is attached to glucose molecules on hemoglobin
When HbA1c CANNOT be used for diagnosis:
- Hemolytic anemia (RBCs destroyed faster - falsely low HbA1c)
- Iron deficiency anemia
- Sickle cell disease / hemoglobinopathies
Confirming diagnosis: HbA1c + Fasting glucose, OR Fasting + Postprandial glucose
1.2 Risk Factors for Type 2 Diabetes
- BMI ≥ 25 kg/m², waist > 80 cm (women)
- Age ≥ 28
- Family history
- Previous pregnancy with macrosomia (baby > 4 kg)
- Ethnicity (South Asian, etc.)
- Previous gestational diabetes
1.3 Pathogenesis of Type 2 Diabetes
The core problem is insulin resistance + relative insulin deficiency.
Insulin resistance involves GLUT-4 receptors (primarily on muscle and fat tissue). The 3 main tissues affected:
- Adipose tissue - reduced glucose uptake
- Skeletal muscle - reduced glucose uptake (GLUT-4 dependent)
- Liver - increased gluconeogenesis (liver keeps making sugar even when not needed)
- Fatty liver disease is BOTH a cause and consequence of insulin resistance
- Treatment: increase physical activity to reduce muscle insulin resistance
- Pioglitazone (thiazolidinedione) acts on GLUT-4 receptors, improves insulin sensitivity
1.4 Gestational Diabetes
Pathogenesis:
- Placental hormones (progesterone, cortisol, GH, placental lactogen) → increase insulin resistance
- Progesterone also increases aldosterone production → increases BP
Screening:
- Glucose Tolerance Test (75g in non-pregnant, 100g in pregnant)
- Done at 24-28 weeks gestation
- After 2 hours: target < 7.8 mmol/L
- If 8.5 mmol/L after 2h → abnormal → repeat test
Diagnostic thresholds in pregnancy:
- Fasting: 5.1 mmol/L = borderline
- Fasting 5.1-5.3 = gestational diabetes
- Fasting 5.3-5.6 = also abnormal range
Management:
- First 12-14 weeks: control by diet + progesterone
- Check sugar 7 times a day
- Metformin can be used
- If < 36 weeks and need steroids → give corticosteroids (for fetal lung maturity) but they worsen glucose
1.5 Insulin Therapy
Types of Insulin:
| Insulin | Onset | Duration | Notes |
|---|---|---|---|
| Regular (soluble) | 30 min | 6-8h | Short-acting; take 30 min before meal |
| Aspart / Lispro | 10-15 min | 3-5h | Ultra-short; take just before/after meal |
| NPH (Neutral Protamine Hagedorn) | 1-2h | 12h | Intermediate acting |
| Glargine (Lantus) | Slow | 22-24h | Long-acting; no peak |
| Detemir | 1-2h | 18-24h | Long-acting |
| Degludec | Slow | >40h | Ultra-long; once daily |
Starting doses:
- Total dose: 0.5 units/kg/day
- Long:Short ratio = 50:50 (e.g., 20 units long + 20 units short)
- Never start full dose - start at half dose (10:10)
- Long-acting (Glargine): 10 units morning OR evening
Bread Unit (BU) system:
- 1 BU = 12g of carbohydrates
- In the morning: 1.5 units insulin per 1 BU (cortisol + GH spike in morning increases insulin requirement)
- Type 2 DM: 1 BU = 1 unit insulin
- Target blood glucose: 5-6 mmol/L fasting; ≤ 6 after meals
Dose adjustments:
- If cortisol is high → increase dose
- If no food planned → decrease dose
- If increased physical activity → decrease dose
Meal distribution for sugar monitoring:
- After breakfast (dose often higher than dinner)
- Before lunch
- After lunch
- Before dinner
- After dinner (target ~6.5)
1.6 Antidiabetic Drug Classes
① DPP-4 Inhibitors (Gliptins)
- Sitagliptin 100 mg
- Mechanism: Inhibit DPP-4 enzyme → prolong GLP-1 and GIP activity → increase insulin secretion
- Advantage: Do NOT cause hypoglycemia
- Safe in CKD (do not use if GFR < 15)
- Note: May increase risk of lymphogranulomatous disease, sarcoidosis
② Metformin (Biguanide)
- Dose: Start 500 mg, maintenance 1000 mg, max 1800-2200 mg/day
- Mechanism:
- Decrease hepatic gluconeogenesis
- Increase insulin sensitivity
- Decrease gut glucose absorption
- Indications: Type 2 DM, pre-diabetes, PCOS
- Advantages: No hypoglycemia (liver keeps working), no weight gain
- Contraindications: GFR < 30 (use small dose if GFR 30-45), heart failure (severe), liver cirrhosis, alcoholism
- Side effects: Lactic acidosis (rare, in hypoxic states), GI upset, B12 deficiency, anemia
- Stop Metformin 48-72 hours before and after contrast studies (risk of AKI + lactic acidosis)
③ GLP-1 Agonists
- Drugs: Liraglutide, Dulaglutide, Semaglutide, Tirzepatide (dual GLP-1/GIP agonist)
- Mechanism: Mimic GLP-1 → increase insulin secretion, decrease glucagon, slow gastric emptying, reduce appetite
- Benefits: Weight loss, reduce CV events (LEADER trial for liraglutide)
- Side effects:
- Nausea, vomiting, diarrhea (malabsorption syndrome)
- Pancreatitis risk
- Gallstones (biliary stones)
- Thyroid C-cell tumors (check calcitonin) - contraindicated in medullary thyroid cancer
- Kidney stones
- Depression, menstrual irregularity
- Tachyphylaxis (drug stops working over time)
- Skin problems
- Tirzepatide: Dual GLP-1/GIP agonist - also causes weight loss, used in DM + obesity
④ Thiazolidinediones (Glitazones)
- Pioglitazone 30 mg
- Mechanism: PPAR-γ agonist → improves insulin sensitivity in fat, muscle, liver
- Benefits: Nephroprotective, treats fatty liver disease (with Vitamin E), not just antidiabetic
- Also used in: Alopecia (hair loss), heart failure management (controversial)
- Side effects: Fluid retention (edema), risk of heart failure, bladder cancer risk, weight gain, arrythmia risk
- Combination: Glargine + Lixisenatide (insulin + GLP-1 combo pen)
⑤ Sulfonylureas
- Better options: Gliclazide, Glimepiride (newer, safer)
- Mechanism: Stimulate pancreatic beta cells to release insulin
- Risk: Hypoglycemia (most dangerous class for hypoglycemia; more dangerous than insulin in some)
- Contraindicated: GFR < 60 (Gliclazide) or GFR < 30 (Glimepiride)
⑥ SGLT-2 Inhibitors (Gliflozins)
- Drugs: Canagliflozin, Empagliflozin (Empa), Dapagliflozin (Dapa)
- Mechanism: Block SGLT-2 transporters in proximal tubule → glucose excreted in urine after meals
- Benefits:
- Weight loss
- Reduce CV mortality (especially Empagliflozin - EMPA-REG trial)
- Nephroprotective (slow CKD progression)
- Reduce HF hospitalizations
- Can be used in Type 1 DM (off-label)
- Contraindicated: GFR < 30 (Canagliflozin), GFR < 45 (some)
- Side effects: UTI, genital mycotic infections, DKA (euglycemic DKA), polyuria
- Do NOT cause hypoglycemia (unless combined with insulin/sulfonylurea)
Special note - CKD + DM:
- Finerenone (Kerendia) - Non-steroidal mineralocorticoid antagonist, 10 mg, max dose - used in DM + CKD (GFR ≥ 25); reduces albuminuria and CV events
1.7 Complications of Diabetes
Acute Complications:
1. Hypoglycemia (glucose < 2.8 or < 3 mmol/L)
Symptoms:
- Dizziness, confusion (like alcohol intoxication)
- Tremors, sweating, vomiting, palpitations
- Nocturnal sweating
- Coma (if severe)
- Can mimic: TB (night sweats), hyperthyroidism (palpitations), cancer, pre-menopause
Causes of hypoglycemia (not just from DM drugs):
- Insulinoma (insulin-producing tumor - usually tail of pancreas)
- Sulfonylureas, insulin overdose
- Antipsychotic drugs
- Adrenal insufficiency (cortisol deficiency)
- Liver cirrhosis (liver can't do gluconeogenesis)
- Pituitary adenoma (↓ ACTH → ↓ cortisol)
- Corticosteroids > 2 weeks → don't taper → adrenal insufficiency
- Tumor (intestine/kidney/radiation-induced)
- Liver transplant complications
2. DKA (Diabetic Ketoacidosis) - occurs in Type 1 DM, insulin deficiency
- Pathogenesis: Insulin deficiency → ketogenesis (β-oxidation of FFA) → ketone bodies → metabolic acidosis
- Triggers: Missed insulin, infection, surgery, pregnancy
- Symptoms: Vomiting, N/V, sweet/fruity breath (ketones), high blood glucose, dehydration
- Management: IV insulin pump + fluids + electrolytes
3. HHS (Hyperosmolar Hyperglycemic State) - occurs in Type 2 DM, very high glucose
- No ketones (residual insulin prevents ketosis)
- Extreme hyperglycemia, severe dehydration, altered consciousness
4. Lactic Acidosis - rare, associated with Metformin in hypoxic states
- Causes: Hypoxia + Metformin intake; liver cirrhosis; alcohol toxicity; B12 deficiency anemia; GFR < 30 + Metformin
Chronic Complications:
Microvascular:
- Nephropathy (diabetic kidney disease)
- Retinopathy (vision loss)
- Neuropathy (peripheral sensory loss, numbness)
Macrovascular:
- CVD (coronary artery disease)
- Stroke
- Peripheral arterial disease (PAD)
- Rhabdomyolysis
📗 TOPIC 2: INFLAMMATORY BOWEL DISEASE (IBD) - Day 13
2.1 Ulcerative Colitis (UC) vs Crohn's Disease (CD)
| Feature | Ulcerative Colitis | Crohn's Disease |
|---|---|---|
| Location | Colon only (rectum always involved) | Whole GIT (mouth to anus) |
| Pattern | Continuous | Skip lesions |
| Depth | Mucosa + submucosa only (superficial) | Transmural (full wall thickness) |
| Histology | Non-granulomatous, crypt abscesses, pseudopolyps | Caseating granulomas, cobblestone appearance, aphthous ulcers |
| Complications | Toxic megacolon, perforation | Fistulas, strictures, abscesses |
| Bleeding | Fresh blood (lower GIT) | Less frequent bleeding |
UC Localisation (Montreal Classification):
- Proctitis (rectum only)
- Proctosigmoiditis
- Left-sided colitis
- Total colitis (pancolitis)
Disease Severity (Truelove & Witts Classification):
Based on:
- Number of bloody stools per day
- Temperature
- Heart rate
- Hemoglobin
- ESR/CRP
Diagnosis:
- Colonoscopy + biopsy (gold standard)
- Mayo score (endoscopic severity)
- Signs on endoscopy: loss of vascular pattern, contact bleeding, superficial ulcers, pseudopolyposis, edema, hyperemia
- Irrigoscopy (barium enema X-ray)
- Capsule endoscopy (NOT done if stenosis/strictures - capsule can get stuck; capsule works for 24h)
- Deep endoscopy (long probe, under anesthesia)
- Hydro MRI (patient drinks mannitol) - good for small bowel
- CT scan
Differential Diagnoses of liquid stool + blood:
- Hemorrhoids, anal fissure
- Dysentery, Salmonella
- Ischemic colitis (vessel thrombosis)
- Diverticulitis
- Pseudomembranous colitis (C. difficile) - presents with fever
- Colorectal neoplasia
- Microscopic colitis
2.2 IBD Treatment
According to attack severity and localisation:
Mild-Moderate (left-sided/proctitis):
- Oral Prednisolone
- Rectal: foam enemas, suppositories
Moderate Attack:
- Oral Prednisolone (reduce dose as improves → stop)
- 5-ASA (mesalazine) for maintenance
Severe:
- IV steroids from the start
Steroid dependence/resistance:
- Azathioprine (immunosuppressant; SE: thrombocytopenia)
- Monitor IBD granule level (thiopurine metabolites)
- Prednisolone course: 12 weeks
Biologics (Monoclonal Antibodies - MAb):
- Vedolizumab (anti-integrin - gut specific)
- Ustekinumab (anti-IL-12/23)
- Before giving biologics: check viral hepatitis serology + TB test (Mantoux) + CXR
Pseudomembranous Colitis (C. difficile):
- Mild: Metronidazole 100 mg 4 times/day orally
- Severe: Vancomycin orally
Crohn's Disease:
- 70% affects ileum → risk of Vitamin B12 deficiency (ileum absorbs B12)
- If ileum affected → do genetic test for CD
- Rule out: Celiac disease, Whipple's disease
- Diagnosis of small bowel CD: Duodenoscopy + biopsy
IBD Complications (Extraintestinal):
- PSC (Primary Sclerosing Cholangitis) - intrahepatic bile ducts affected
- Erythema nodosum (skin - bluish/red nodules on legs)
- Arthritis (large joints)
- Uveitis (eye)
📙 TOPIC 3: THYROID DISEASE - Day 23
3.1 Hypothyroidism
Causes:
- Hashimoto's thyroiditis (autoimmune, antibodies against TPO - anti-TPO)
- Postpartum thyroiditis
- Atrophic thyroiditis
- Pituitary adenoma (secondary hypothyroidism, ↓ TSH)
- Iodine deficiency
- Subacute thyroiditis (after viral infection, starts with thyrotoxicosis → then hypothyroidism)
- Drugs: Amiodarone, Interferon, Lithium, PTU, Methimazole, Tyrosine kinase inhibitors
- Riedel's thyroiditis
- Sarcoidosis, amyloidosis, hemochromatosis
Symptoms by system:
| System | Manifestations |
|---|---|
| CNS | Memory loss, depression, slow reflexes |
| CVD | AV block (any type), pericarditis, arrhythmia, resistant HTN |
| Musculoskeletal | Weakness, pain, ↑ CK (creatine kinase) |
| GI | ↓ appetite, constipation, bilestasis |
| Dermatology | Dry skin, subcutaneous edema, myxedema |
| Eye | Periorbital edema |
| Gynecology | Amenorrhea, menstrual irregularity, infertility |
| Hematology | Anemia (pale, fatigue), hypochromic anemia (due to malabsorption) |
| Other | Polyneuropathy, carpal tunnel syndrome |
Why edema in hypothyroidism?
- Accumulation of GAGs (glycosaminoglycans) + hyaluronic acid in tissues → attract water → myxedema (non-pitting edema)
- Diuretics do NOT work in myxedema
Why high cholesterol in hypothyroidism?
- ↓ LDL clearance from blood (liver receptors reduced)
- ↓ Lipoprotein lipase activity
- ↓ Cholesterol breakdown
- ↓ Hepatic metabolism of lipids
- ↓ Fat metabolism overall
Lab findings:
- TSH ↑ (primary hypothyroid)
- T3/T4 ↓
- ↑ Cholesterol
- Anemia
Treatment (L-thyroxine / T4):
- Dose: 1.6 mcg/kg/day (calculate according to weight)
- Start LOW especially in elderly, cardiac patients
- Example: Patient with cardiomyopathy, EF = 15%, atrial fibrillation/ventricular tachycardia → start 6.25 mcg, check after 1 week → increase to 12.5 mcg → titrate up
- If patient given 50 mcg wrongly → drug-induced thyrotoxicosis → stop L-thyroxine → level drops to subclinical hypothyroidism
Warfarin interaction: L-thyroxine increases metabolism → increases PT ratio → risk of bleeding → need to adjust warfarin dose after thyroid normalizes
Radioactive iodine therapy - indicated for toxic adenoma, Graves' disease (after methimazole)
3.2 Thyrotoxicosis (Hyperthyroidism)
Symptoms:
- Cardiovascular: Tachycardia, paroxysmal AF, palpitations
- Neurological: Tremor, insomnia, anxiety, mood swings, emotional lability
- GI: Belly pain, diarrhea, spastic pains
- Eyes: Exophthalmos, proptosis, dry eyes, vision problems (ophthalmopathy)
- Musculoskeletal: Muscle weakness, myopathy
- Other: Weight loss despite normal appetite, hyperhidrosis
Note: Elderly patients on beta-blockers may mask symptoms (just dry eyes may be the only complaint)
Complications:
- Atrial fibrillation (Afib) - most common cardiac complication
- Dyshormohal cardiomyopathy, heart failure (hypertrophy of LV walls)
- Thyroid storm (crisis) - can occur after contrast iodine injection (e.g., post coronary angiography)
- HTN (Grade 2)
- Osteoporosis (long-standing thyrotoxicosis)
- Paralysis
- Ophthalmopathy: Proptosis, exophthalmos, retroorbital tissue hyperplasia
- Seizures (low K+)
- Gynecological problems (menstrual irregularity)
Hashimoto's Disease (15-H):
- TSH: 2.5 mIU/L
- Start L-thyroxine if: antibody positive + TSH elevated + symptoms
Treatment of Thyrotoxicosis:
- Methimazole / Carbimazole - total 18 months to 2 years of treatment
- Side effects: Agranulocytosis (if fever → check WBC), anemia, hepatitis
- After treatment: check thyroid size
- Subclinical thyrotoxicosis from subacute thyroiditis: starts with thyrotoxicosis → use NSAIDS first, then Prednisolone if needed
Thyroid storm treatment: Stop L-thyroxine, restart at very low dose; PTU acutely
Iodine deficiency (goitre):
- Start iodine supplements
- If want to get pregnant → give thyroxine even with iodine supplement
- Selenium + Zinc: reduce nodule size, reduce anti-TPO antibodies, reduce thyroid size
📒 TOPIC 4: CKD (Chronic Kidney Disease) - Day 28
4.1 Why Males Have Higher Risk of CKD
- Men have FEWER nephrons than women to begin with
- Women: lose nephrons after age 20 progressively
- Boys have higher UTI risk after age 11
- Male risk factors: smoking, alcohol, drugs
4.2 Causes / Risk Factors for AKI and CKD Progression
- NSAIDs (nephrotoxic)
- Aminoglycosides (gentamicin)
- Cyclosporine, Antivirals (Tenofovir), Chemotherapy (Cisplatin)
- PPI long-term use
- Radiocontrast agents (toxic → stop Metformin 48-72h before and after contrast)
- Gadolinium (MRI contrast) - toxic in CKD; use only if GFR > 30
- Thiazide diuretics can cause dehydration → AKI
- Uncontrolled DM, uncontrolled HTN, elderly age
4.3 Definition of CKD
- GFR < 60 mL/min for > 3 months, AND/OR
- Albumin/creatinine ratio elevated (albuminuria) even if GFR is normal
4.4 Functions of the Kidney
- Osmoregulation (water balance)
- Electrolyte regulation (Na, K, Ca, Phosphate)
- Filtration (1801 L/day through 25 km of capillaries)
- Blood pressure regulation (renin, prostaglandins)
- Erythropoiesis (EPO production) → anemia if CKD
- Phosphorus-Calcium metabolism
- Vitamin D activation (1-alpha hydroxylation in kidney → active calcitriol)
- Fibrinolysis (urokinase, tPA - alteplase given in STEMI)
4.5 CKD Mineral Bone Disease (Vitamin D Pathway)
- Kidney disease → cannot produce 1-alpha hydroxylase
- → Cannot convert 25-OH Vitamin D → active 1,25-OH2 Vitamin D
- → ↓ Ca2+ absorption from gut
- → ↓ Ca2+ stimulates ↑ PTH (parathyroid hormone) - secondary hyperparathyroidism
- PTH tries to raise calcium:
- Pulls Ca2+ from bones → osteoporosis
- Stimulates phosphate excretion from kidney (but kidney already damaged)
- → ↑ Phosphate accumulates
Treatment of mineral bone disease in CKD:
- Vitamin D supplements (50,000 IU / 12 weeks) → suppress PTH
- Active Vitamin D (Paricalcitol) = VDR activator; used if GFR < 30
- Phosphate binders (sevelamer) - months to start working; give before meals; check ALP when giving (bone disorder marker)
- Eladetinib (new agent)
- Cinacalcet (calcimimetic) → activates calcium-sensing receptors → suppresses PTH
- Denosumab (if GFR < 30; for osteoporosis)
- Bisphosphonates - contraindicated if GFR < 30
4.6 Anemia of CKD
Pathogenesis:
- ↓ EPO production by kidney → ↓ RBC production
- ↑ Hepcidin (acute phase reactant) → traps iron in macrophages → iron-restricted erythropoiesis
- ↓ Ferroportin → iron cannot exit macrophages
- ↑ Cytokines (chronic inflammation) → suppress bone marrow
Features: Normochromic, normocytic anemia (anemia of chronic disease - ACD)
Target Hb: 110-115 g/L
Treatment:
- EPO analogues / ESAs (Erythropoiesis-stimulating agents) - if patient agrees
- Roxadustat (HIF-PH inhibitor) - oral, 2x/week; alternative to EPO injections
- Iron: only if transferrin saturation is low (don't give iron if normochromic ACD without iron deficiency)
4.7 HTN in CKD Treatment
Step-up approach:
- RAAS blockade (ACE inhibitor or ARB):
- If GFR > 15: Telmisartan (ARB - Valsartan is stronger than Losartan)
- If GFR < 30: be cautious
- Sacubitril/Valsartan (Neprilysin inhibitor): used in uncontrolled HTN + HF
- Loop diuretics (GFR < 30)
- Cardioselective beta-blockers: Carvedilol, Metoprolol (NOT non-selective; avoid non-selective)
- Spironolactone / Eplerenone / Finerenone - for resistant HTN (caution with K+)
- Moxonidine 0.3 mg - central alpha-2 agonist; used in last-stage resistant HTN
Drugs that raise K+ (hyperkalemia risk):
- Spironolactone, Eplerenone, Finerenone
- ACE inhibitors / ARBs
- Non-selective beta-blockers
- NSAIDs
- Statins (via rhabdomyolysis → cell damage → K+ release)
- ATT (anti-tuberculosis therapy)
- Anti-cancer drugs
Managing hyperkalemia (K+ > 5.5 mEq/L):
- Stop the offending drug if possible
- Diuretics
- Calcium gluconate (IV for cardiac protection - K+ > 6.5-7)
- Patiromer (potassium binder)
- Polystyrene sulphonate (K+ binder)
4.8 Dyslipidemia in CKD
Targets:
- LDL < 1.8 mmol/L (< 1.2 mmol/L in dialysis)
- TG < 1.7 mmol/L
- HbA1c < 7%
Drugs:
- Fenofibrate: if GFR > 60 (for TG)
- Rosuvastatin 10-20 mg: safe in CKD; before/after dialysis, with meals
- PCSK9 inhibitors (Inclisiran): most potent LDL-lowering option
- Ezetimibe: before/after dialysis
4.9 CKD Diet
- Protein restriction: 0.8 g/kg/day (but not < 0.6/kg - risk of sarcopenia)
- ↓ Sodium (not just ↓ salt)
- Vegetarian diet: creatinine comes out low (vegetarians have less muscle mass) → use Cystatin C for GFR if creatinine is unreliable
4.10 Indications for Dialysis
| Indication | Notes |
|---|---|
| pH < 7.1 (severe acidosis) | |
| Very high K+ | Life-threatening |
| Fluid overload | Pulmonary edema |
| Uremic encephalopathy | |
| GFR < 15 | Or < 20 in cardiac patients |
Peritoneal dialysis - less expensive, home-based, but risk of peritonitis
Hemodialysis - more expensive, 3x/week
Renal Transplant: Patient must take 2 cytostatic drugs for life to prevent rejection
4.11 Urine Analysis Interpretation (from the lab notes)
| Finding | Meaning |
|---|---|
| Proteinuria > 3.5 g/day | Nephrotic syndrome |
| Hematuria + Proteinuria + Hypertension | Nephritic syndrome |
| WBC casts + Bacteria +++ | Pyelonephritis / UTI |
| RBC casts | Glomerulonephritis |
| Granular/waxy casts | CKD / serious nephron damage |
| Glucosuria + Proteinuria | DM nephropathy |
| Red wine colored urine (cloudy) | Hemolytic anemia |
📔 TOPIC 5: HEPATOBILIARY SYSTEM - Day 14
5.1 Chronic Cholecystitis & Biliary Dyskinesia
Types of gallbladder dysfunction:
- Functional disorder (Biliary dyskinesia): Abnormal motility, contraction, sphincter of Oddi spasm
- Non-calcular cholecystitis: Inflammation without gallstones
Symptoms:
- Biliary pain in right hypochondrium (radiates to right shoulder, back)
- Belt-like pain
- Bitter taste, bloating
- Dyspeptic syndrome (nausea, more epigastric → need to differentiate from cardiac pain)
- Severe episodic pain if stone stuck in GB neck
Difference from cardiac pain:
- Cardiac: pressing, retrosternal, NOT relieved by Nitroglycerin... wait - actually GB pain is NOT relieved by Nitroglycerin (cardiac pain IS relieved by nitro)
Diagnosis:
- USG: wall thickness > 4-5 mm, dense bile/sludge, polyps
- USG after fatty food (yoghurt/fatty meal) → check GB contraction
- Biliary scintigraphy (IV contrast + fatty food) → assess bile flow
- MRCP / ERCP (for bile duct stones/strictures)
Types of Jaundice:
- Mechanical/Obstructive: All LFTs elevated, ↑ ALP, itching; caused by tumor of pancreas, stone
- Hemolytic: Indirect bilirubin elevated; reticulocytes high; haemolytic anemia
- Hepatic: Viral hepatitis, any etiology; ↑ transaminases
Gilbert's Syndrome: Genetic ↑ bilirubin (indirect); no jaundice; benign; polyps remain; treat with UDCA
5.2 Metabolic Syndrome + Fatty Liver
Metabolic Syndrome criteria:
- Obesity (BMI > 30, or visceral obesity)
- Glucose intolerance / DM
- Dyslipidemia
- HTN (≥ 130/80)
NAFLD / Metabolic Liver Disease:
- Grade 1: ALT elevated < 5x normal (Degree 1: mild steatosis)
- Progresses to steatohepatitis → cirrhosis
Treatment of Fatty Liver:
- Pioglitazone + Vitamin E (improves histology)
- UDCA (ursodeoxycholic acid) - dissolves cholesterol stones, protects liver, 3 months then recheck USG
- Dietary changes + healthy lifestyle + exercise
- Atorvastatin 80 mg (if bad cholesterol / LDL high)
- Hepatoprotectors:
- Ademetionine (Heptral): 800 mg IV; good for alcoholic hepatitis; also oral 1-2 months
- Used for cytolytic syndrome (high ALT/AST)
- Antibiotics (if bacterial exacerbation):
- Mild: Metronidazole (no major side effects)
- Strong: Ciprofloxacin 500 mg, OR Ceftriaxone (7 days)
- Intestinal antiseptic (e.g., Rifaximin) for dysbiosis
- Prokinetics: Trimebutine (also helps biliary motility - 2-3 times/day)
- Hemochromatosis (iron overload): improves sphincter of Oddi function; improves bile flow; improves pancreatic flow
📕 TOPIC 6: HEMATOLOGY - Day 17 (Lab Interpretation)
6.1 Hepatic Syndromes (Lab-based)
| Syndrome | Markers |
|---|---|
| Cytolytic | ↑ ALT, ↑ AST, ↑ LDH |
| Cholestatic | ↑ ALP, ↑ GGT, ↑ Direct bilirubin, ↑ Cholesterol |
| Hepatic insufficiency | ↓ Albumin, ↓ Prothrombin index (↑ INR), ↑ Globulins |
| Mesenchymal inflammation | ↑ Globulins, ↑ IgG |
| Portal HTN / Hypersplenism | ↓ Platelets, ↓ RBC |
6.2 CBC Interpretation & Blood Disorders
Normal values used in notes:
- RBC: 4.5-5.5 (men), 4-5 (women) x10¹²/L
- Hb: 130-175 (men), 120-155 (women) g/L
- Color Index (CI): 0.85-1.05
- Reticulocytes: 1-2% (regenerative marker)
- Platelets: 150-400 x10⁹/L
- WBC: 4-9 x10⁹/L
Anemia staging by Hb:
- Stage I: Hb 90-120 (women) / 100-130 (men) - mild
- Stage II: Hb 70-90 - moderate
- Stage III: Hb < 70 - severe
Key blood picture patterns:
| Pattern | Likely Diagnosis |
|---|---|
| ↑ Myelocytes + Metamyelocytes (normally 0) + ↑ WBC + Immature myeloid cells | CML (Chronic Myeloid Leukemia) |
| If blasts > 20% | Blast crisis (AML transformation) |
| Lymphocytosis 90% + Immature cells | CLL (Chronic Lymphocytic Leukemia) - Botkin |
| Microspherocytosis + hyperregenerative anemia | Hereditary spherocytosis / Hemolytic anemia (Coombs test - anti-IgG) |
| Normochromic anemia + ↓ Reticulocytes + ↓ PLT + ↓ WBC (pancytopenia) | Aplastic anemia (BMD - bone marrow destruction) |
| Plasma cells + M-gradient | Multiple Myeloma |
| Basophilia + Eosinophilia association with CML | |
| WBC 4 + Lymphocytes 90% (immature) | ALL (Acute Lymphocytic Leukemia) - lymphoblasts |
Pyelonephritis/UTI urine (noted in class):
- WBC +++, RBC casts, bacteria +++, mucus +++, cloudy urine
🔬 CLINICAL CASES DISCUSSED IN NOTES
Case 1 (Page 12) - 42-year-old Track Driver
- Complaints: 2 months fatigue, episodes of loss of consciousness, cramping leg pain, flank pain, poor eating (gastric), going to work, blurry vision, UTI 7 days, on PPI 1 month, NSAIDs for cramps
- Examination: BP 130/90, weight 95 kg, waist 105 cm, HR 80, liver enlarged (4 cm)
- Likely diagnoses:
- Type 2 DM (polyuria, polydipsia, hyperglycemia signs)
- Stage 1 HTN
- Obesity (BMI > 30)
- Fatty liver disease
- Peripheral arterial disease (leg pain, vascular examination needed)
- COPD (smoker, 1 pack/day, 40 years)
- Polyneuropathy (loss of sensation)
- Dyspeptic syndrome
- Investigations needed: Blood glucose, HbA1c, TSH, biochemistry (Sr.Cr, AST, ALT, GGT), CBC, urinalysis, Vitamin B12, ECG
Case 2 - Thyroid Cardiomyopathy
- Ejection fraction 15%, cardiomyopathy
- Started on 6.25 mcg L-thyroxine very cautiously due to severe cardiac compromise
- Private clinic had wrongly given 50 mcg → drug-induced thyrotoxicosis → stop → revert to subclinical hypothyroid level
🩺 PRACTICAL EXAMINATION SKILLS (from Yulia Ma'am - Day 22)
Percussion of Lungs
- Comparative percussion: both sides, 3 times, start from right side
- Zigzag pattern: upper clavicle → on clavicle → 3rd intercostal space → zigzag paravertebral
- Sounds: Resonance (normal lung), Dullness (consolidation, pleural effusion, liver), Tympanic (hollow/air-filled organs)
- Emphysema: Hyperresonance (large thorax, barrel chest)
- Pleural effusion, abscess: Dull sound
Vocal Fremitus (Voice Vibration)
- Patient says "33" (in Russian) while you feel vibration on chest wall
- Pneumonia: ↑ vibration
- Abscess: ↓ vibration (initially), then ↑ when draining
- Bronchus open: ↑ vibration
Cardiac Borders Percussion
- Rt border: Mid-clavicular line (move from lung → dullness = cardiac border)
- Left border: 5th ICS - 2 cm from mid-clavicular line
- Upper border: 3rd ICS, parasternal line
- Parasternally from above/below
Cardiac Auscultation
- Apex (Mitral Valve): 5th ICS, mid-clavicular
- 2nd ICS R (Aortic)
- 2nd ICS L (Pulmonary)
- 4th ICS L (Tricuspid) - Erb's point
- Young people: may have functional murmur (due to connective tissue dysplasia → extra myofibrils, trabeculation)
- Not serious - functional
Pulse Examination
- Check both hands (important for coarctation of aorta, AVblock)
- AF: irregular pulse
- Pulse deficit: AF - difference between apical and radial pulse
- Extrasystole: extra contraction
- Character: regularity, amplitude, shape
BP Measurement
- Cuff above elbow, 2-finger loose placement
- Hand position: palm up, at heart level
- Also in popliteal fossa (leg BP)
Liver Palpation (Kurlov's Method)
- Start from mid-clavicular line
- Find lower border of liver by percussion from umbilicus going up
- Kurlov lines: 10-9-8 cm (normal)
- Palpate during inspiration (hand supports from back)
Gallbladder Points
- Murphy's sign: Inspire + palpate right hypochondrium → pain on inspiration = positive
- McKenzie point: GB intersection with right hypochondrium
- Boas point: 10th-11th vertebrae left (posterior)
- Mayo-Robson point: Pancreatic tail (intersection of spinal cord and 2nd rib at back)
Abdomen
- Superficial palpation: rigidity, tension, pain, mass, hernias
- Compare 9 points: Start from flank
- Go from your right side, cycle around: hypochondrium R → epigastrium → hypochondrium L → etc.
✅ Summary Table: Key Drug Reminders from Notes
| Drug | Key Clinical Pearl |
|---|---|
| Metformin | Stop 48-72h before contrast; max 2200 mg; CI in severe HF, GFR<30 |
| Tirzepatide | Dual GLP-1/GIP; check calcitonin (thyroid risk); check for thyroid cancer |
| Pioglitazone + Vit E | Treatment of NAFLD (improves histology) |
| SGLT-2i | Do NOT cause hypoglycemia; protect kidney; good for HF |
| Sulfonylureas | Most dangerous for hypoglycemia; CI if GFR < 60 (gliclazide) |
| L-thyroxine | Start very low in cardiac patients; adjust Warfarin |
| Methimazole | SE: agranulocytosis → fever = check WBC; course = 18-24 months |
| UDCA | Dissolves cholesterol stones; hepatoprotective; 3 months treatment |
| Ademetionine (Heptral) | Hepatoprotector; good for alcoholic hepatitis; 800 mg IV |
| Rosuvastatin | Safe in CKD; can be given before/after dialysis |
| Finerenone | Non-steroidal MRA; used in DM + CKD; reduces albuminuria |
| Sevelamer | Phosphate binder in CKD; takes months to work; give before meals |
| Roxadustat | HIF inhibitor; oral EPO alternative; 2x/week |
| Azathioprine | Immunosuppressant for IBD; SE: thrombocytopenia |
| Vancomycin (oral) | Severe C. difficile colitis |
These notes cover a comprehensive clinical curriculum including endocrinology (DM + thyroid), gastroenterology (IBD + hepatobiliary), nephrology (CKD), and practical clinical examination skills. The level of detail suggests these are 4th-5th year medical student polyclinic rotation notes.
How to differentiate infiltrative & dissemination TB
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.