Lymphatic drainage of tongue in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"tongue" AND "lymphatic drainage" AND "sentinel lymph node"
Searching the Web
lymphatic drainage of tongue Scott Brown Cummings Dhingra detailed anatomy RGUHS ENT
Finding Sources
Finding Sources
Searching PubMed
"oral tongue" AND "lymph node" AND "metastasis" AND "level"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9942923
Reading File
Finding Sources
Reading File
Reading Article
PMID: 39218959
Here is the complete 20-mark answer, structured as expected for RGUHS ENT examinations:
LYMPHATIC DRAINAGE OF THE TONGUE
20-Mark Answer | RGUHS University ENT Examination
INTRODUCTION
The tongue has the richest lymphatic supply of any head and neck structure relative to its size. Its lymphatic drainage is complex, clinically variable, and of immense surgical significance - particularly in oral cavity and oropharyngeal carcinomas. Understanding the drainage patterns determines neck dissection levels, bilateral vs. unilateral neck management, sentinel node identification, and prognosis.
RELEVANT ANATOMY
The tongue is divided by the circumvallate (vallate) papillae into:
- Oral tongue (anterior 2/3): mobile, anterior to the linea terminalis (oral cavity)
- Base of tongue / lingual root (posterior 1/3): part of the oropharynx
The tongue is separated at the midline by the median fibrous lingual septum - a partial (not absolute) barrier to midline lymphatic crossover.
LYMPHATIC VESSEL GROUPS OF THE TONGUE
(Scott-Brown's Otorhinolaryngology, 8th ed, p.684)
The tongue's lymphatics are divided into three main vessel groups:
1. MARGINAL VESSELS
- Arise from the apex and lingual frenulum area
- Descend under the mucosa
- Drain to submental nodes and jugulo-omohyoid nodes
- Some vessels cross under the frenulum → contralateral nodes (bilateral drainage for tip)
2. CENTRAL VESSELS
- Drain the central/medial body of the tongue
- May drain to either or both sides into deep cervical nodes
- Principal nodes: jugulodigastric (Level II) and jugulo-omohyoid (Level IV)
3. DORSAL VESSELS
- Drain the posterior tongue (behind circumvallate papillae)
- Drain bilaterally into upper deep cervical nodes (Level II-III)
REGION-BY-REGION DRAINAGE
| Region | Primary Nodes | Laterality | AJCC Level |
|---|---|---|---|
| Tip | Submental | Bilateral | Level IA |
| Lateral anterior 2/3 | Submandibular | Ipsilateral | Level IB |
| Medial anterior 2/3 | Deep cervical (jugulodigastric) | Ipsilateral (mainly) | Level II-III |
| Ventral surface | Submental → deep cervical | Bilateral | IA, II |
| Posterior 1/3 (Base) | Jugulodigastric, mid-deep cervical | Bilateral | Level II, III |
| Posteriormost / Vallecula | Upper deep cervical, lateral pharyngeal | Bilateral | Level II, retropharyngeal |
(Cummings Otolaryngology, 7th ed, p.1655; KJ Lee Essential Otolaryngology, 12th ed, p.847)
DIAGRAM: Lymphatic Drainage of Oral Tongue and Oropharynx
(KJ Lee's Essential Otolaryngology, 12th ed - Figure 45-3)
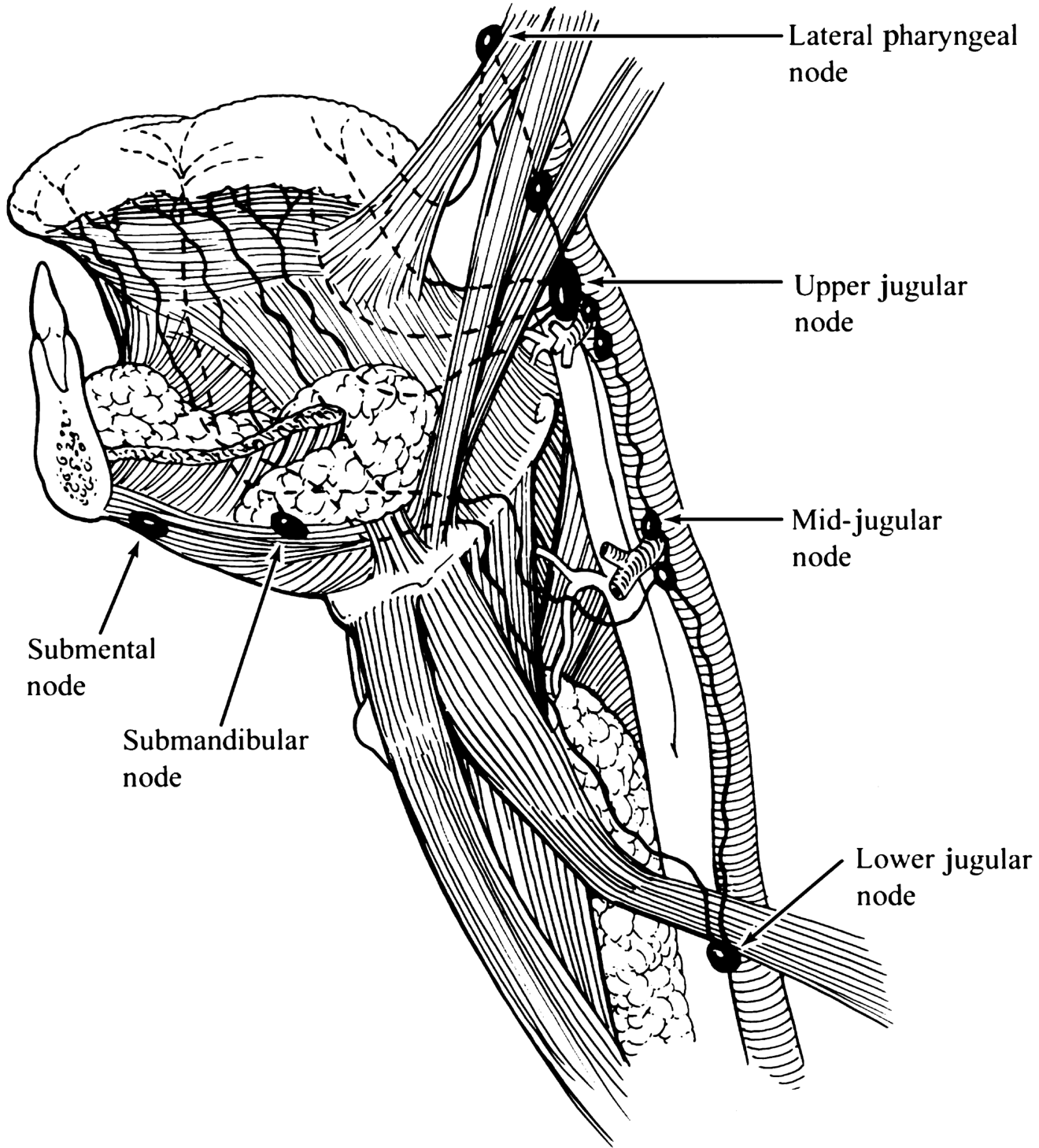
Fig. 1 - KJ Lee: Lymphatic drainage of the oral tongue and oropharynx. Primary nodal drainage is to Levels I-III. Note submental, submandibular, upper/mid/lower jugular, and lateral pharyngeal nodes.
DIAGRAM: Base of Tongue - Primary Echelon
(Cummings Otolaryngology, 7th ed - Fig. 96.5)

Fig. 2 - Cummings: Lymphatics of the base of the tongue with the jugulodigastric nodes as primary echelon.
DIAGRAM: Bilateral Base of Tongue Drainage
(Cummings Otolaryngology, 7th ed - Fig. 96.6)
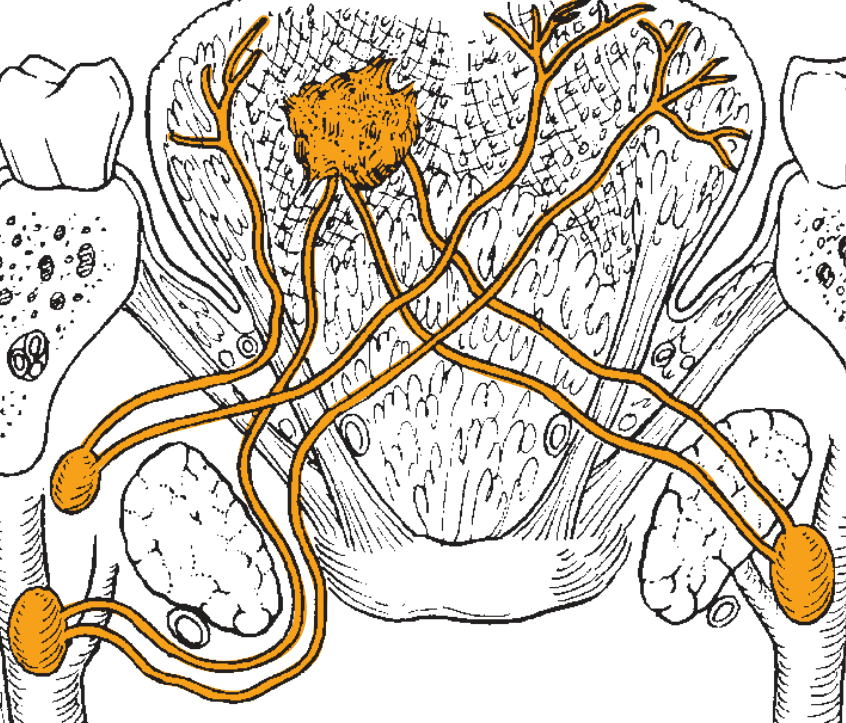
Fig. 3 - Cummings: Bilateral base of tongue lymphatic drainage showing crossover channels - the basis for bilateral nodal disease in base-of-tongue carcinomas.
FLOWCHART 1: Oral Tongue Lymphatic Pathway
ORAL TONGUE
│
├─ TIP ──────────────→ SUBMENTAL NODES (Level IA) [Bilateral]
│ ↓
│ DEEP CERVICAL (Level II)
│
├─ LATERAL BORDER ───→ SUBMANDIBULAR (Level IB) [Ipsilateral]
│ ↓
│ JUGULODIGASTRIC (Level II)
│ ↓
│ JUGULO-OMOHYOID (Level III-IV)
│
├─ MEDIAL/CENTRAL ───→ JUGULODIGASTRIC (Level II) [Bilateral possible]
│ JUGULO-OMOHYOID (Level III)
│
└─ DORSAL SURFACE ───→ JUGULODIGASTRIC (Level II) [Ipsilateral mainly]
FLOWCHART 2: Base of Tongue Lymphatic Pathway
BASE OF TONGUE (Post 1/3)
│
├──────────────────→ JUGULODIGASTRIC NODES (Level II) [PRIMARY ECHELON]
│ ↓
├──────────────────→ LATERAL PHARYNGEAL / PARAPHARYNGEAL NODES
│
├──────────────────→ MID-DEEP CERVICAL (Level III)
│
└─ BILATERAL DRAINAGE → BOTH SIDES (ipsi + contralateral)
↓
EXPLAINS HIGH RATE OF BILATERAL NODAL DISEASE
FLOWCHART 3: Final Common Lymphatic Pathway
ALL TONGUE LYMPHATICS
↓
SUBMENTAL (IA) → SUBMANDIBULAR (IB) → JUGULODIGASTRIC (II)
↓
JUGULO-OMOHYOID (III-IV)
↓
LOWER DEEP CERVICAL (IV-V)
↙ ↘
THORACIC DUCT RIGHT LYMPHATIC DUCT
(Left side) (Right side)
↓
SUBCLAVIAN VEIN JUNCTION
↓
VENOUS SYSTEM
TEXTBOOK-BY-TEXTBOOK SYNTHESIS
CUMMINGS OTOLARYNGOLOGY (7th Ed, Ch. 91, p.1655)
- Tip → submental; lateral tongue → Levels I-II; base → upper cervical
- Skip metastasis to Level III/IV (bypassing I/II) is recognized
- Anterior lymphatics have no free anastomoses → ipsilateral drainage
- Base of tongue lymphatics → crossover → bilateral spread more readily
SCOTT-BROWN'S OTORHINOLARYNGOLOGY (8th Ed, p.684)
- Three vessel groups: marginal, central, dorsal
- Lateral borders → ipsilateral cervical nodes
- Midline, tip, base → bilateral
- Drainage is variable; no precise single description
- Marginal vessels from apex/frenulum → submental + jugulo-omohyoid nodes
KJ LEE'S ESSENTIAL OTOLARYNGOLOGY (12th Ed, p.847, Fig. 45-3)
- Regional metastasis: primary drainage to Levels I-III
- Midline dorsum or ventral surface → greater risk of bilateral metastases
- 25-33% clinically detectable; 20-25% occult nodal disease in cN0 neck
DHINGRA'S ENT (7th Ed)
- Tip → Submental (bilateral)
- Lateral anterior 2/3 → Submandibular (ipsilateral); central fibers bilaterally
- Posterior 1/3 → Jugulo-omohyoid (bilateral)
- Posteriormost → Upper deep cervical (bilateral)
HAZARIKA'S ENT & HEAD-NECK SURGERY
- Jugulo-omohyoid node = "tongue node" - key sentinel for tongue tip pathology
- Tongue has richest lymphatic supply in head and neck
- Posterior tongue lesions → mandatory bilateral neck treatment
- Free midline communication in posterior tongue; absent anteriorly
STELL AND MARAN'S HEAD AND NECK SURGERY (4th Ed)
- Submental nodes → tip and floor of mouth
- Submandibular nodes → anterior 2/3 lateral
- Jugulodigastric = sentinel/primary echelon for posterior tongue
- Jugulo-omohyoid = "tongue node" for tip drainage via long lymphatic channel
- Deep cervical chain = final common pathway
ZAKIR HUSSAIN (Indian ENT)
- Lingual nodes (inconstant intramuscular nodes) as first-order nodes
- Subsequent drainage → jugular chain (Levels I-IV)
- Bilateral neck dissection mandatory for midline and posterior tongue tumors
GRAY'S ANATOMY FOR STUDENTS (4th Ed)
- Lingual nodes primarily drain tongue
- Submental nodes drain tip of tongue, floor of mouth, lower lip
- All drain via submandibular nodes (first and second filtering stations)
- Final drainage → deep cervical nodes → jugular trunk → venous system
CLINICAL SIGNIFICANCE
1. Neck Dissection Planning
| Tumor Site | Recommended Neck Treatment |
|---|---|
| Tip (midline) | Bilateral Level IA, IB, II |
| Lateral oral tongue | Ipsilateral Level I-III elective (END) |
| Posterior 1/3 / Base | Bilateral Level II-IV |
| Midline dorsum/ventral | Bilateral Level I-III |
2. Skip Metastasis
- Direct Level III/IV spread WITHOUT involvement of Level I/II
- Incidence: 10-15% of oral tongue SCC
- Risk factors: depth of invasion >4mm, perineural invasion, lymphovascular invasion
- Clinical implication: Elective neck dissection must include Level III (not just I-II)
- (Bailey & Love's Surgery, 28th ed; Yang et al., Clin Oral Investig, 2024, [PMID: 39218959])
3. Occult Nodal Metastasis (ONM)
- 20-25% of cN0 oral tongue cancers harbor microscopic nodal disease
- ONM significantly reduces disease-free survival (P<0.001)
- Tumor thickness ≥6.4mm on MRI predicts ONM preoperatively
- Elective neck dissection of Level I-III sufficient for early OTSCC
- (Yang et al., 2024, PMID: 39218959)
4. Depth of Invasion (DOI) - AJCC 8th Edition (2017)
- DOI (not tumor thickness) incorporated in T-staging:
- T1: ≤2cm and DOI ≤5mm
- T2: ≤2cm with DOI 5-10mm, OR >2cm with DOI ≤10mm
- T3: >4cm OR any tumor DOI >10mm
- DOI >4mm = elective neck treatment even in cN0
5. Extranodal Extension (ENE)
- Formally incorporated in AJCC 8th Edition nodal staging
- ENE → adverse prognosis in ALL oral cavity tumors
- (Bailey & Love's Surgery, 28th ed)
RECENT ADVANCES (2020-2025)
1. ICG Near-Infrared Fluorescence SLNB
- Indocyanine green injected peri-tumorally → detected by NIR camera intraoperatively
- Real-time sentinel node mapping; identifies nodes missed by Tc-99m
- Validated for early tongue cancer and oropharyngeal cancer
- (Zhou et al., 2022, PMID: 36748378)
2. SPIO-Enhanced MRI for SLN Mapping
- Superparamagnetic iron oxide (SPIO) nanoparticles → taken up by sentinel nodes → visible on MRI
- Non-invasive, non-radioactive, preoperative SLN identification
- Feasibility study published in 2025
- (Heldens et al., 2025, PMID: 41241690)
3. Machine Learning for Predicting Occult LN Metastasis
- Explainable ML model using MRI + clinical parameters
- Multi-center validated for early-stage OTSCC
- May guide objective decision for elective neck dissection
- (Zhu et al., 2025, Int J Surg, PMID: 40479496)
4. SPECT-CT for Contralateral Lymphatic Mapping
- Preoperative SPECT-CT delineates bilateral drainage patterns
- Guides bilateral vs. unilateral neck dissection in lateralized tumors
- (Berania et al., 2022, PMID: 36575528)
5. Dense Mucosal Lymphatic Network - Histological Insight
- Denser lymphatic capillary network in mucosa than tongue musculature
- 5-7 collecting vessels between genioglossal muscles carry midline lymph bilaterally
- Base of tongue drains predominantly to Levels II and III
- (Physiology of the Tongue, PMC9942923, 2023)
EXAMINATION QUICK-RECALL POINTS
- Tip → Bilateral submental (Level IA) - "tip tip: both sides"
- Lateral tongue → Ipsilateral Level I-II
- Base of tongue → BILATERAL Level II-IV (always both necks)
- Jugulo-omohyoid = "Tongue node" (Sentinel for tip)
- Jugulodigastric = Primary echelon for posterior tongue/base
- Skip metastasis (10-15%) → Levels III-IV direct, bypassing I-II
- Occult nodal disease = 20-25% in cN0 oral tongue cancer
- DOI >4mm = Elective neck dissection recommended
- Final drainage: Thoracic duct (L) / Right lymphatic duct (R)
- Midline septum is NOT a complete barrier - crossover possible
REFERENCES
- Flint PW et al. Cummings Otolaryngology Head and Neck Surgery, 7th ed. Elsevier. Ch. 91, p.1655; Ch. 96.
- Watkinson JC, Clarke RW. Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed. CRC Press. p.684-685.
- Lee KJ. Essential Otolaryngology, 12th ed. McGraw-Hill. Ch.45, p.847, Figure 45-3.
- Dhingra PL. Diseases of Ear, Nose and Throat, 7th ed. Elsevier India.
- Hazarika P. Textbook of ENT and Head-Neck Surgery. Elsevier India.
- Stell PM, Maran AGD. Stell and Maran's Head and Neck Surgery, 4th ed. Butterworth-Heinemann.
- Schunke M et al. Color Atlas of Human Anatomy Vol 2 (Thieme), p.150.
- Gray's Anatomy for Students, 4th ed. Elsevier.
- Yang X et al. Risk factors and occult/skip metastasis in OTSCC. Clin Oral Investig 2024. [PMID: 39218959]
- Zhou B et al. ICG fluorescence in sentinel LN biopsy for tongue cancer. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2022. [PMID: 36748378]
- Heldens GTN et al. SPIO-enhanced MRI for sentinel LN mapping. Eur Radiol Exp 2025. [PMID: 41241690]
- Berania I et al. Contralateral neck failure in OPSCC with SPECT-CT mapping. J Otolaryngol Head Neck Surg 2022. [PMID: 36575528]
- Zhu R et al. ML model for predicting occult LN metastasis in OTSCC. Int J Surg 2025. [PMID: 40479496]
This is a shared conversation. Sign in to Orris to start your own chat.