Hyperkalemia,hypernatremia, hyponatremia and hypokalemia in detail with proper understanding with photos in medicine MBBS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Here is a complete, MBBS-level guide to all four electrolyte disorders, fully sourced from authoritative medical textbooks with diagnostic flowchart images and ECG diagrams.
Key Takeaways for Each Disorder
Hyponatremia (Na+ <135)
The central concept is volume status + urine Na+. First exclude pseudohyponatremia and hyperosmolar causes. For true hypo-osmotic hyponatremia: hypovolemic = Na lost, hypervolemic = water retained (CHF/cirrhosis/nephrotic), euvolemic = SIADH/hypothyroid/hypoadrenal. The biggest treatment danger is overcorrecting chronic hyponatremia, which causes osmotic demyelination syndrome (ODS) - cap correction at 6-8 mmol/L per 24 hours.
Hypernatremia (Na+ >145)
Almost always reflects free water deficit. Use the volume status + urine osmolality algorithm (shown in the diagram). Patients cannot self-correct if unconscious or elderly - these are the most vulnerable. Central DI (low urine osmolality, responds to DDAVP) vs. nephrogenic DI (does not respond to DDAVP) is the key differentiator for euvolemic cases. Never correct faster than 0.5 mmol/L/hour - too-rapid correction causes cerebral edema.
Hypokalemia (K+ <3.5)
Distinguish redistribution (no true deficit - check for insulin, alkalosis, beta-agonists) from true deficit (check 24-hr urine K+ - renal vs. extrarenal). The ECG hallmark is the U wave. Critically, always check and replace magnesium - hypomagnesemia causes refractory hypokalemia. DKA patients with normal K+ on presentation often have profound total body K+ deficit unmasked by insulin treatment.
Hyperkalemia (K+ >5.0)
First rule out pseudohyperkalemia (hemolysis, WBC >70,000). ECG guides urgency - peaked T waves are the earliest sign, progressing to sine wave and VF. Treatment follows three steps: Stabilize (calcium gluconate) → Shift (insulin+dextrose, salbutamol) → Remove (furosemide, resins, dialysis). In DKA, hyperkalemia with insulin deficiency masks profound total body K+ depletion - watch for hypokalemia as you give insulin.
Generate a comparison poster of all four disorders side-by-side
Generating Image
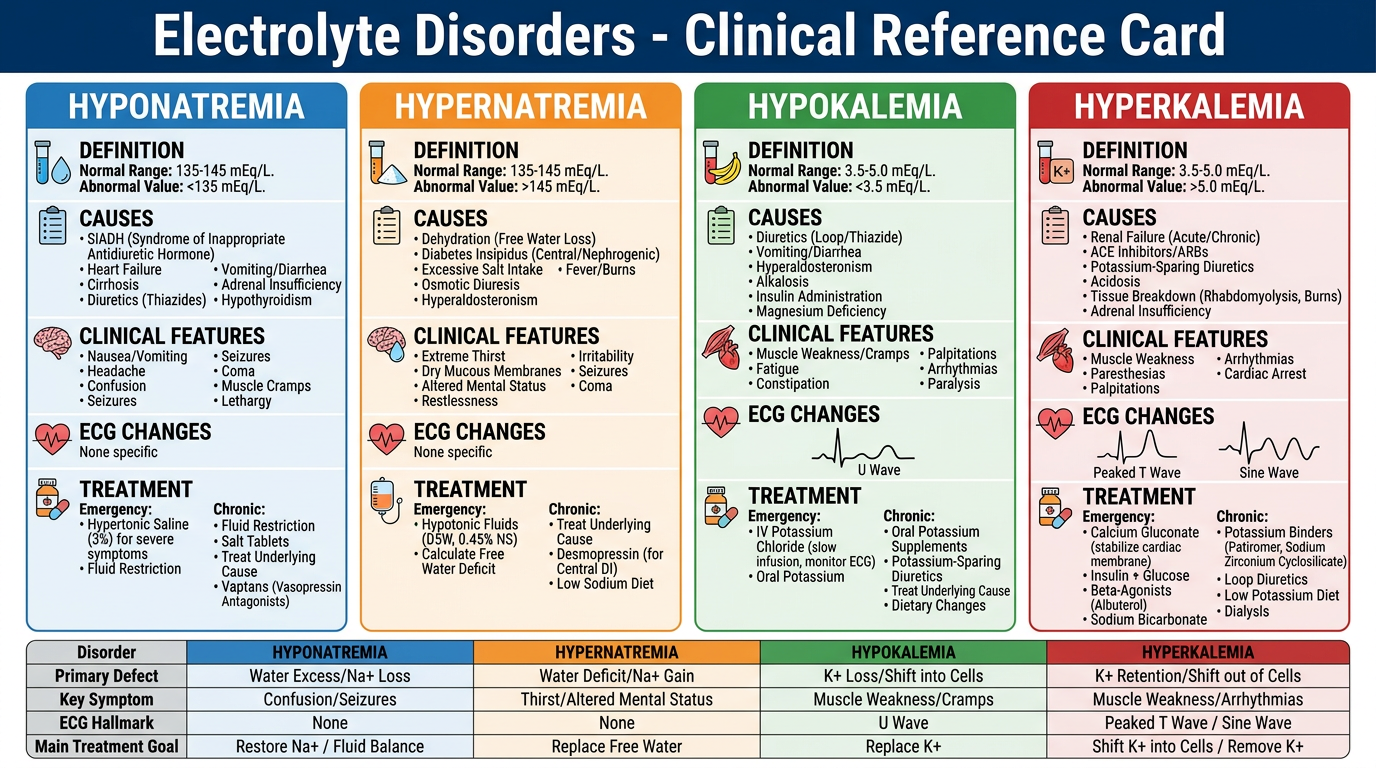
Here is your side-by-side comparison poster covering all four electrolyte disorders. Each column is color-coded and organized into the same sections so you can quickly compare them at a glance:
- Blue - Hyponatremia (Na+ <135): Volume-based approach, SIADH, treatment with 3% NaCl, ODS risk
- Orange - Hypernatremia (Na+ >145): Water deficit approach, DI types, free water replacement
- Green - Hypokalemia (K+ <3.5): U wave on ECG, redistribution vs. true deficit, oral/IV KCl
- Red - Hyperkalemia (K+ >5.0): Peaked T waves → sine wave, three-step treatment (Stabilize → Shift → Remove)
This poster is designed as a quick revision reference card for MBBS clinical exams and ward use. Let me know if you'd like any section expanded, a separate poster for ECG changes only, or a printable PDF version.
Tell me in detail
analyse_media
The analysis was truncated. Let me walk you through every detail of the poster from the content I generated and the full medical knowledge behind it.
Electrolyte Disorders - Clinical Reference Card: Full Detail
HOW THE POSTER IS STRUCTURED
The poster has 4 color-coded columns (one per disorder) and 6 rows of content:
| Row | Content |
|---|---|
| 1 | Header: Name + Definition + Normal Range |
| 2 | Primary Defect / Mechanism |
| 3 | Causes (bulleted) |
| 4 | Clinical Features / Symptoms |
| 5 | ECG Changes |
| 6 | Treatment (Emergency + Chronic) |
| Bottom | Summary Comparison Table |
COLUMN 1 - HYPONATREMIA (Blue)
Header
- Serum Na+ < 135 mmol/L
- Normal: 135-145 mmol/L
- Most common electrolyte disorder in hospitalized patients (15-30%)
Primary Defect
Water excess relative to sodium OR sodium loss exceeding water loss. Result: low plasma osmolality → water shifts INTO brain cells → cerebral edema.
Causes
Step 1 - Check plasma osmolality:
- Normal osmolality (280-295) → Pseudohyponatremia: hyperlipidemia, hyperproteinemia
- High osmolality → Hyperosmolar: hyperglycemia (every 100 mg/dL glucose rise drops Na+ by ~1.6 mmol/L), mannitol, uremia
- Low osmolality → True hypoosmotic hyponatremia (most common - proceed to Step 2)
Step 2 - Check volume status + urine Na+:
| Volume | Urine Na+ | Causes |
|---|---|---|
| Hypovolemic | <10 | Vomiting, diarrhea, burns, sweating, third-spacing |
| Hypovolemic | >20 | Diuretics, Addison's, RTA, salt-losing nephropathy |
| Euvolemic | High (>20) | SIADH, hypothyroidism, hypoadrenalism |
| Hypervolemic | <10 | CHF, cirrhosis, nephrotic syndrome |
| Hypervolemic | >20 | Acute/chronic renal failure |
SIADH causes (very common exam topic):
- CNS: meningitis, encephalitis, stroke, SAH, head trauma
- Pulmonary: pneumonia, TB, COPD, abscess, positive pressure ventilation
- Drugs: SSRIs, carbamazepine, cyclophosphamide, vincristine, chlorpropamide, NSAIDs, opioids
- Malignancy: small cell lung cancer (most common), pancreatic ca, duodenal ca
- Post-surgery (pain/stress → ADH release)
Clinical Features
| Na+ Level | Symptoms |
|---|---|
| 130-135 | Often asymptomatic; nausea, malaise |
| 125-130 | Headache, lethargy, confusion |
| 120-125 | Disorientation, behavioral change |
| <120 | Seizures, stupor, coma |
| <105 | Brain herniation, death |
- Acute drops (within 24-48 hrs) cause symptoms at higher Na+ levels (~125)
- Chronic drops are better tolerated (brain has adapted)
ECG Changes
- No specific ECG pattern for hyponatremia itself
- Note: underlying cause (e.g., Addison's with hyperkalemia) may produce ECG changes
Treatment
Acute symptomatic (seizures/herniation):
- 100 mL of 3% NaCl IV over 10 minutes - repeat up to 3 times
- Target: raise Na+ by 4-6 mmol/L urgently to stop symptoms
- No restriction on rate if truly acute hyponatremia (<24-48 hrs)
Chronic hyponatremia:
- Maximum correction: 6-8 mmol/L per 24 hours (absolute max 10-12 mmol/L/day)
- SIADH: fluid restriction 500-1000 mL/day; salt tablets; furosemide + NaCl
- Vaptans (tolvaptan, conivaptan): V2 receptor antagonists - for euvolemic/hypervolemic SIADH
- Treat underlying cause
⚠️ Osmotic Demyelination Syndrome (ODS / Central Pontine Myelinolysis):
- Caused by overcorrection of chronic hyponatremia
- Risk: Na+ <105 for >48 hrs, hypokalemia, alcohol, malnutrition, liver disease
- Features: locked-in syndrome, pseudobulbar palsy, quadriplegia, ataxia
- MRI: T2 hyperintensity in pons and extrapontine areas
- Prevention: NEVER exceed 10-12 mmol/L/24 hrs
- If overcorrection occurs: re-lower Na+ with hypotonic saline + desmopressin
COLUMN 2 - HYPERNATREMIA (Orange)
Header
- Serum Na+ > 145 mmol/L
- Always = hyperosmolality
- Mortality 40-60% in critically ill patients
Primary Defect
Free water deficit relative to sodium. Brain cells lose water to ECF → neuronal shrinkage → intracranial hemorrhage (tearing of bridging veins in acute severe cases).
In chronic hypernatremia: brain cells generate idiogenic osmoles (taurine, myoinositol) to protect against dehydration - this is why rapid correction causes cerebral edema.
Causes by Volume Status
Hypovolemic Hypernatremia (most common):
- Renal water loss + inadequate replacement:
- Osmotic diuresis: DKA, HHS, mannitol, high-protein tube feeds
- Loop diuretics
- Extrarenal loss:
- Diarrhea, vomiting
- Burns
- Fever, sweating
- Respiratory (tachypnea, mechanical ventilation)
- Urine osmolality >800 mOsm/kg (kidneys concentrating urine appropriately)
Euvolemic Hypernatremia (pure water loss):
- Central Diabetes Insipidus - lack of ADH secretion:
- Trauma, surgery, pituitary tumors, granulomas (sarcoidosis), ischemia, idiopathic
- Urine osmolality <800 (often <300), urine specific gravity <1.005
- Responds to DDAVP (desmopressin)
- Nephrogenic Diabetes Insipidus - kidney resistant to ADH:
- Lithium (most common drug cause), demeclocycline, amphotericin B
- Hypercalcemia, hypokalemia (impair concentrating ability)
- CKD, sickle cell, amyloidosis
- Does NOT respond to DDAVP
- Urine osmolality low despite high plasma osmolality
- Insensible losses: fever, burns, hyperventilation
Hypervolemic Hypernatremia (sodium gain):
- Hypertonic saline administration
- Sodium bicarbonate IV (cardiac arrest resuscitation)
- Hyperaldosteronism (Conn's syndrome)
- Cushing syndrome
- Salt poisoning (rare)
- Mineralocorticoid excess
Distinguishing Central vs Nephrogenic DI (Water Deprivation Test):
| Test | Central DI | Nephrogenic DI |
|---|---|---|
| Urine osmolality after water deprivation | <300 mOsm/kg | <300 mOsm/kg |
| After DDAVP administration | Rises >50% (responds) | No significant rise (<10%) |
| Plasma ADH | Low/undetectable | High (ADH present but no effect) |
Clinical Features
| Na+ Level | Symptoms |
|---|---|
| 145-150 | Often asymptomatic (if chronic) |
| 150-160 | Thirst, irritability, restlessness, lethargy |
| 160-170 | Tremors, ataxia, confusion, muscle twitching |
| >170 | Coma, focal deficits, death |
| >175 (chronic) | May be asymptomatic (brain has adapted) |
Acute (Na+ >160): brain can shrink, tearing bridging veins → subdural/subarachnoid hemorrhage
Children and the elderly are at highest risk.
ECG Changes
- No specific ECG pattern
- Underlying hypervolemia may show signs of the primary condition
Treatment
Step 1 - Calculate free water deficit:
Free water deficit (L) = 0.6 × weight (kg) × [(serum Na / 140) - 1]
Step 2 - Choose replacement fluid:
- Oral water/NG free water (preferred if conscious)
- IV 5% Dextrose (D5W) - free water equivalent
- IV 0.45% NaCl (half-normal saline) - for hypovolemic patients after volume restored
- IV 0.9% NaCl (normal saline) - FIRST if hemodynamically unstable (to restore volume before correcting Na+)
Step 3 - Correction rate:
- Maximum 0.5 mmol/L/hour or 10-12 mmol/L per 24 hours
- Overcorrection → cerebral edema (brain's accumulated osmoles draw in too much water)
Specific treatments:
- Central DI: DDAVP (desmopressin) intranasal/SC/IV + free water
- Nephrogenic DI: Remove causative drug; thiazide diuretics (paradoxically reduce urine output via volume contraction); NSAIDs; low-salt, low-protein diet
- Hypervolemic: loop diuretics + 5% dextrose
COLUMN 3 - HYPOKALEMIA (Green)
Header
- Serum K+ < 3.5 mmol/L
- Normal: 3.5-5.0 mmol/L
- Most of body's K+ is intracellular (98%) - only 2% is extracellular
Primary Defect
Resting membrane potential = -90 mV (maintained by K+ gradient). Hypokalemia hyperpolarizes cells → harder to depolarize → skeletal muscle weakness, but also lowers threshold for spontaneous cardiac depolarization → arrhythmias.
Causes
A. Redistribution INTO cells (no total body deficit, serum K+ drops):
- Insulin (activates Na+/K+-ATPase) - most common in DKA treatment
- Alkalosis (H+ exits cells, K+ enters to maintain electroneutrality)
- Beta-2 agonists (salbutamol, terbutaline, adrenaline) - activate Na+/K+-ATPase
- Catecholamine excess (stress, phaeochromocytoma)
- Hypokalemic periodic paralysis (familial - attack triggered by carbs/exercise/cold)
- Vitamin B12/folate treatment (rapid cell proliferation uses K+)
- Hypothermia, theophylline toxicity
B. Decreased intake:
- Starvation, anorexia nervosa
- Total parenteral nutrition without adequate K+
- Tea-and-toast diet in elderly
C. Renal losses (24-hr urine K+ >25 mmol/day):
- Diuretics - most common drug cause:
- Loop diuretics (furosemide, bumetanide)
- Thiazides (hydrochlorothiazide, chlorthalidone)
- Mineralocorticoid excess - aldosterone increases K+ excretion:
- Primary hyperaldosteronism (Conn's syndrome) - hypertension + hypokalemia
- Secondary hyperaldosteronism (CHF, cirrhosis, renovascular HT)
- Cushing's syndrome / exogenous glucocorticoids
- Congenital adrenal hyperplasia (11β-hydroxylase, 17α-hydroxylase deficiency)
- Apparent mineralocorticoid excess, Liddle syndrome
- Bartter syndrome (autosomal recessive): loop-like salt wasting; normo/hypotension, metabolic alkalosis, very high renin/aldosterone
- Gitelman syndrome: thiazide-like; milder, hypomagnesemia, hypocalciuria; most common inherited renal tubular disorder
- Renal tubular acidosis type 1 (distal) and type 2 (proximal)
- Hypomagnesemia (blocks ROMK channel; K+ leaks out of tubular cells)
- Drugs: aminoglycosides, amphotericin B, cisplatin, penicillins (non-reabsorbable anion effect), capreomycin
D. GI losses (24-hr urine K+ <25 mmol/day - kidneys conserving K+):
- Diarrhea (K+-rich stool fluid - especially secretory diarrhea)
- Laxative abuse
- Vomiting/NG suction (K+ loss + metabolic alkalosis drives renal K+ loss secondarily)
- Enterocutaneous fistulas, ileostomy
- Villous adenoma of rectum (secretes K+-rich mucus)
Clinical Features
| System | Mild (3.0-3.5) | Moderate (2.5-3.0) | Severe (<2.5) |
|---|---|---|---|
| Muscle | Fatigue, cramps | Proximal weakness | Paralysis, rhabdomyolysis |
| Heart | Occasional PVCs | ECG changes, AF | VT, VF, cardiac arrest |
| GI | Constipation | Paralytic ileus | Abdominal distension |
| Kidney | Polyuria | Polydipsia | Hypokalemic nephropathy |
| Metabolic | Mild alkalosis | Glucose intolerance | Growth retardation (children) |
ECG Changes in Hypokalemia (Sequence)
| Finding | Mechanism | When |
|---|---|---|
| Flattened/inverted T waves | Delayed repolarization | K+ <3.5 |
| Prominent U wave (>T wave amplitude) | Delayed M-cell repolarization - HALLMARK | K+ <3.0 |
| ST-segment depression | - | K+ <3.0 |
| Prolonged QU interval | (not true QT prolongation) | K+ <2.5 |
| Increased P-wave amplitude, prolonged PR | - | K+ <2.5 |
| VT (torsades de pointes) / VF | Complete conduction breakdown | K+ <2.0 |
U wave: positive deflection after T wave, best seen in V2-V3. Normal U waves are small; in hypokalemia they become prominent and can exceed T wave height.
Treatment
| Severity | K+ Level | Route | Dose |
|---|---|---|---|
| Mild | 3.0-3.5 | Oral KCl | 40-60 mmol/day divided doses |
| Moderate | 2.5-3.0 | Oral KCl aggressive | 60-80 mmol/day; consider IV |
| Severe/Symptomatic | <2.5 or arrhythmia | IV KCl | 10-20 mmol/hr (central line preferred); max 40 mmol/hr in extreme emergency |
Key rules:
- NEVER give IV K+ as a bolus (can cause cardiac arrest)
- Max peripheral IV: 10 mmol/hr (concentrated K+ causes vein sclerosis)
- Max central IV: 20-40 mmol/hr with continuous cardiac monitoring
- Always replace magnesium first - hypomagnesemia causes refractory hypokalemia (Mg2+ is required to keep K+ inside cells via ROMK channel inhibition)
- For diuretic-induced: switch to K+-sparing diuretic (spironolactone, amiloride) or add K+ supplement
COLUMN 4 - HYPERKALEMIA (Red)
Header
- Serum K+ > 5.0 mmol/L
- Mild: 5.0-5.9 | Moderate: 6.0-6.4 | Severe: ≥6.5
- Life-threatening at >6.5, usually fatal >10.0 mmol/L
Primary Defect
High extracellular K+ partially depolarizes resting membrane potential (less negative). This inactivates Na+ channels → decreased excitability of muscle and nerve cells. In the heart, reduced resting potential = impaired conduction → bradycardia → heart block → VF.
Causes
A. Pseudohyperkalemia (K+ elevated in sample but not in the patient):
- Hemolysis during blood draw (most common) - red cells release K+
- Prolonged tourniquet time or fist-clenching
- Severe leukocytosis (WBC >70,000/mm³) - WBCs release K+ after sample drawn
- Thrombocytosis (platelets >500-1000 × 10⁹/L) - ~1/3 of these patients have pseudohyperkalemia
- Diagnosis: serum K+ >0.3 mmol/L higher than simultaneous plasma K+
- Management: repeat with plasma sample (heparin tube instead of serum tube), free-flowing sample without tourniquet
B. Redistribution OUT of cells:
- Acidosis (H+ enters cells, K+ exits to maintain electroneutrality) - metabolic or respiratory
- Insulin deficiency (normal insulin drives K+ into cells via Na+/K+-ATPase)
- Hyperosmolality (hyperglycemia, mannitol - osmotic water shift out of cells carries K+ with it)
- DKA: insulin deficiency + hyperosmolality → hyperkalemia despite total body K+ deficit
- Beta-blockers (especially non-selective: propranolol) - block beta-2 mediated cellular K+ uptake
- Digoxin toxicity (inhibits Na+/K+-ATPase)
- Succinylcholine (depolarizing NMJ blockade - causes K+ efflux; avoid in burns, denervation, rhabdomyolysis - can cause K+ rise of 0.5-1.0 mmol/L, but up to 5-10 in at-risk patients)
- Hyperkalemic periodic paralysis (hereditary Na+ channel mutation)
- Rhabdomyolysis, tumor lysis syndrome, massive hemolysis, crush injury
C. Increased K+ intake (usually only with co-existing impaired excretion):
- K+ supplements, K+-containing salt substitutes
- High-K+ foods (bananas, oranges, tomatoes, potatoes, beans) in CKD patients
- Blood transfusions (stored blood has high K+ due to hemolysis)
- Enteral/parenteral nutrition
D. Decreased renal K+ excretion (most common cause of chronic hyperkalemia):
- Acute Kidney Injury (AKI) - especially oliguric
- Chronic Kidney Disease (CKD) - GFR <10-20 mL/min
- Obstructive uropathy - bilateral obstruction
- Adrenal insufficiency (Addison's disease) - lack of aldosterone:
- Classic triad: hyperkalemia + hyponatremia + metabolic acidosis
- Check morning cortisol and ACTH stimulation test
- Hyporeninaemic hypoaldosteronism (Type IV RTA) - most common in diabetic nephropathy; low renin → low aldosterone
- Drugs reducing renal K+ excretion (most important clinically):
| Drug Class | Examples | Mechanism |
|---|---|---|
| ACE inhibitors | Enalapril, ramipril, lisinopril | Decrease angiotensin II → decrease aldosterone |
| ARBs | Losartan, valsartan, candesartan | Block AT1 receptor → decrease aldosterone |
| K+-sparing diuretics | Spironolactone, eplerenone | Block aldosterone receptor |
| K+-sparing diuretics | Amiloride, triamterene | Block ENaC directly |
| NSAIDs | Ibuprofen, naproxen | Decrease prostaglandins → decrease renin |
| Heparin (unfractionated + LMWH) | - | Direct adrenal cytotoxicity → decrease aldosterone |
| Trimethoprim | - | Blocks ENaC (amiloride-like effect) |
| Calcineurin inhibitors | Tacrolimus, cyclosporine | Decrease aldosterone effect |
- Pseudohypoaldosteronism type 2 (Gordon syndrome): hypertension + hyperkalemia + normal GFR; WNK kinase mutation → excess NaCl and K+ retention
ECG Changes in Hyperkalemia
| K+ (mmol/L) | ECG Change | Significance |
|---|---|---|
| 4-5 | Normal | - |
| 5.5-6.5 | Peaked (tented) T waves | First sign; narrow base, high amplitude; best in V2-V5 |
| 6.5-7.5 | Flattened/absent P waves, prolonged PR | Atrial standstill |
| 7-8 | Widened QRS (>0.12 sec), ST depression | Ventricular conduction delay |
| >8-9 | Sine wave pattern (QRS merges with T) | Pre-terminal rhythm |
| >9-10 | Ventricular fibrillation / asystole | Cardiac arrest |
Important: ECG changes can appear at any K+ level - a patient with K+ of 6.2 may have a sine wave pattern while another with K+ of 7.0 may have only peaked T waves. Always treat the ECG, not just the number.
Treatment - The Three-Step Approach
STEP 1 - STABILIZE the heart membrane (if ECG changes or K+ >6.5):
| Drug | Dose | Onset | Duration | Mechanism |
|---|---|---|---|---|
| IV Calcium gluconate 10% | 10 mL IV over 2-3 min | 1-3 min | 30-60 min | Raises cardiac resting membrane potential threshold; does NOT lower K+ |
| IV Calcium chloride 10% | 5-10 mL IV | 1-3 min | 30-60 min | More elemental Ca2+; preferred in cardiac arrest |
- Repeat every 5-10 min if ECG changes persist
- Do NOT mix calcium with NaHCO3 (precipitates as CaCO3)
- Give slowly over 20-30 min in digoxin toxicity (hypercalcemia worsens digoxin toxicity)
STEP 2 - SHIFT K+ into cells (temporizing - does not remove K+):
| Drug | Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Insulin 10 units IV + 50 mL of 50% dextrose | IV bolus | 15-30 min | 4-6 hr | Monitor glucose; most reliable agent |
| Salbutamol (albuterol) nebulized | 10-20 mg (high dose) | 30-60 min | 2-4 hr | Synergistic with insulin; tachycardia |
| NaHCO3 50 mmol IV | 50 mL of 8.4% | 15-30 min | 1-2 hr | Only if pH <7.2; AVOID in anuric patients (can worsen K+) |
STEP 3 - REMOVE K+ from the body (definitive):
| Method | Dose | Time to Effect | Notes |
|---|---|---|---|
| Furosemide IV | 40-80 mg IV | 30-60 min | Only if adequate renal function and not oliguric |
| Sodium polystyrene sulfonate (Kayexalate) | 15-60 g orally | 4-6 hr | Exchanges Na+ for K+ in colon; given with sorbitol (avoid in post-op bowel) |
| Patiromer | 8.4-25.2 g/day oral | 4-7 hr | Better tolerated; preferred for chronic management |
| Sodium zirconium cyclosilicate (SZC, Lokelma) | 10 g TID × 48h, then 5 g/day | 1-2 hr | Fastest acting resin; useful in acute setting |
| Hemodialysis | - | Minutes | Most rapid and reliable removal; used in AKI, CKD, or refractory/severe hyperkalemia |
Chronic Management
- Low-K+ diet (<2 g/day in severe cases)
- Optimize acid-base balance (correct metabolic acidosis with NaHCO3)
- Increase renal excretion: loop diuretic (furosemide), fludrocortisone (if adrenal insufficiency)
- Long-term potassium binders: patiromer or SZC
- Review all K+-raising medications - weigh benefit vs. risk (ACEi/ARB in heart failure have mortality benefit)
MASTER COMPARISON TABLE
| Feature | Hyponatremia | Hypernatremia | Hypokalemia | Hyperkalemia |
|---|---|---|---|---|
| Value | Na+ <135 | Na+ >145 | K+ <3.5 | K+ >5.0 |
| Cell Effect | Cells swell (water in) | Cells shrink (water out) | Hyperpolarized | Partially depolarized |
| CNS Effect | Cerebral edema | Cerebral dehydration | Muscle weakness | Weakness, confusion |
| ECG Hallmark | None | None | U wave, flat T | Peaked T waves → sine wave |
| Most Common Cause | SIADH, diuretics | Diabetes insipidus | Diuretics, diarrhea | AKI/CKD, ACEi/ARBs |
| Emergency Rx | 3% NaCl 100 mL bolus | D5W / 0.45% NaCl | IV KCl 20 mmol/hr | IV Calcium gluconate 10 mL |
| Second-line Rx | Treat cause, vaptans | DDAVP (central DI) | Mg2+ replacement | Insulin+Dextrose, Salbutamol |
| Definitive Rx | Fluid restriction (SIADH) | Free water replacement | Oral KCl + treat cause | Dialysis / K+ binders |
| Overcorrection Danger | ODS (demyelination) | Cerebral edema | Hyperkalemia | Hypokalemia |
| Correction Rate | Max 6-8 mmol/L per 24h | Max 0.5 mmol/L per hour | Based on severity/ECG | Based on ECG changes |
| Key Mnemonic | SIADH: Euvolemic, High Urine Na | DI: Polyuria + Hypernatremia | "Hypo K = U wave" | "Hyper K = Peaked T → Sine Wave → VF" |
This is the complete breakdown of every element in the poster. Let me know if you want a deeper dive into any specific disorder, a separate ECG-only diagram, or a flowchart for management steps.
This is a shared conversation. Sign in to Orris to start your own chat.