DKA Secondary spontaneous pneumothorax in COPD Methanol intoxication Closed abdominal trauma emergency topics make osce station cases
Generate a comparison poster (DKA vs Hyperosmolar Hyperglycemic State)
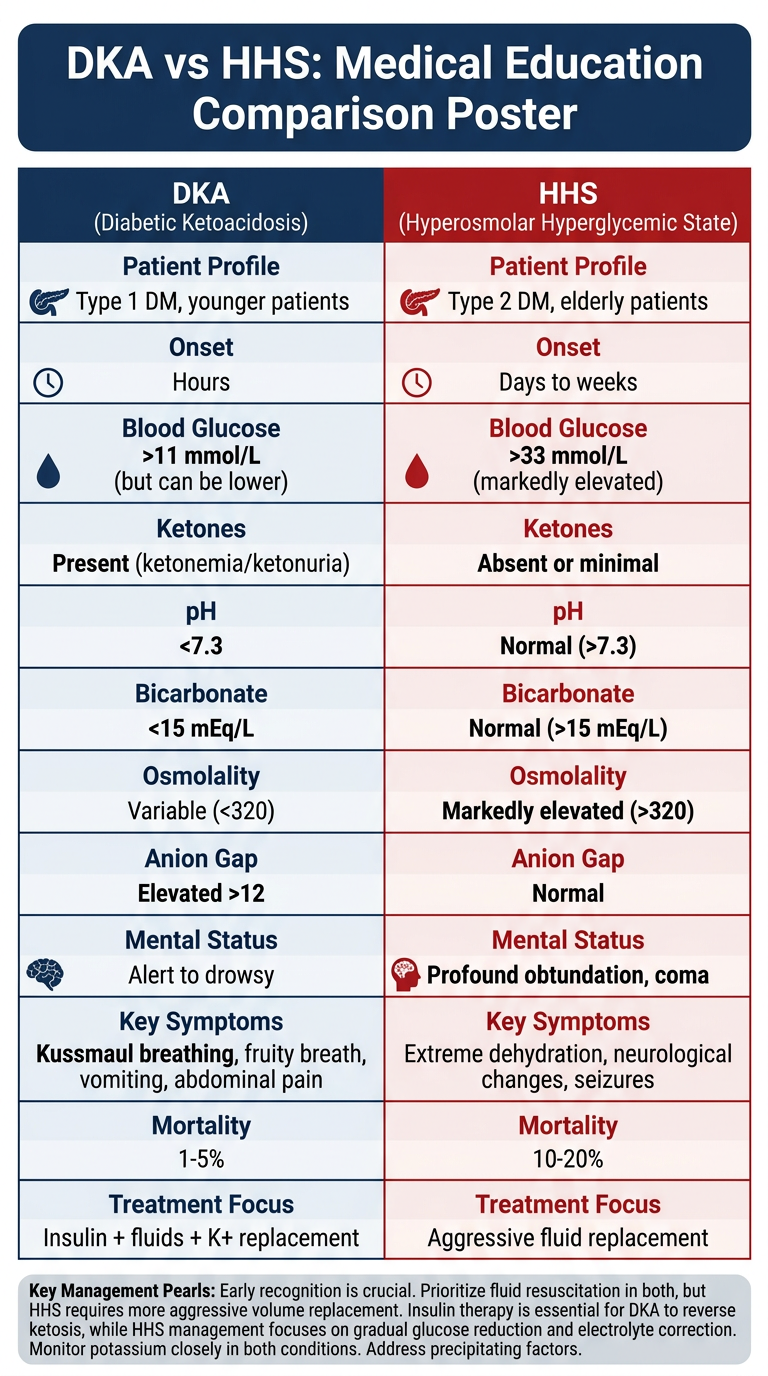
Medical education comparison poster: DKA (Diabetic Ketoacidosis) vs HHS (Hyperosmolar Hyperglycemic State). Clean clinical reference poster with two clearly divided columns, one for DKA and one for HHS. Include these comparison categories as rows: Patient Profile, Onset, Blood Glucose, Ketones, pH, Bicarbonate, Osmolality, Anion Gap, Mental Status, Key Symptoms, Mortality, Treatment Focus. DKA column data: Type 1 DM, younger patients; Hours; >11 mmol/L (but can be lower); Present (ketonemia/ketonuria); <7.3; <15 mEq/L; Variable (<320); Elevated >12; Alert to drowsy; Kussmaul breathing, fruity breath, vomiting, abdominal pain; 1-5%; Insulin + fluids + K+ replacement. HHS column data: Type 2 DM, elderly patients; Days to weeks; >33 mmol/L (markedly elevated); Absent or minimal; Normal (>7.3); Normal (>15 mEq/L); Markedly elevated (>320); Normal; Profound obtundation, coma; Extreme dehydration, neurological changes, seizures; 10-20%; Aggressive fluid replacement. Use a professional medical poster style with a navy blue and red color scheme for the two columns, clear section headers, bold values for critical differences, and a title banner at the top. Add a footer with key management pearls.
| Feature | DKA | HHS |
|---|---|---|
| Patient | Type 1 DM, younger | Type 2 DM, elderly |
| Onset | Hours | Days to weeks |
| Blood Glucose | >11 mmol/L (variable) | >33 mmol/L (markedly high) |
| Ketones | Present +++ | Absent or trace |
| pH | <7.3 (acidosis) | >7.3 (normal) |
| Bicarbonate | <15 mEq/L | >15 mEq/L |
| Osmolality | Variable (<320) | >320 mOsm/kg |
| Anion Gap | Elevated (>12) | Normal |
| Mental Status | Alert to drowsy | Profound obtundation / coma |
| Key Symptoms | Kussmaul breathing, fruity breath, vomiting, abdominal pain | Extreme dehydration, focal neuro deficits, seizures |
| Mortality | 1-5% | 10-20% (higher - older patients, delayed presentation) |
| Treatment Focus | Insulin + fluids + K+ replacement | Aggressive fluid replacement first |
- DKA: The problem is lack of insulin - correct the ketoacidosis with insulin. Potassium management is critical (K+ <3.3 = hold insulin; replace first).
- HHS: The problem is profound dehydration (fluid deficit 8-12 L) - correct with fluids first. Insulin plays a secondary role. Transition slowly to avoid cerebral edema.
- Overlap: A mixed DKA/HHS picture can occur, especially in Type 2 DM patients under severe physiologic stress.
Generate a step-by-step insulin dosing and potassium replacement protocol
Medical clinical protocol flowchart poster titled "DKA: Insulin Dosing & Potassium Replacement Protocol" for hospital emergency use. Dark navy background with bright white and yellow text. Professional, clean, clinical style. The poster has the following clearly structured flow: TOP SECTION - "STEP 1: CHECK POTASSIUM FIRST (before starting insulin)" with a large decision diamond shape: - K+ LESS THAN 3.3 mEq/L → RED box: "HOLD INSULIN. Give IV KCl 20-40 mEq/hr. Recheck K+ before starting insulin" - K+ 3.3 to 5.5 mEq/L → GREEN box: "START INSULIN. Give 20-40 mEq KCl per liter of IV fluid concurrently" - K+ GREATER THAN 5.5 mEq/L → ORANGE box: "START INSULIN. Hold potassium supplementation. Recheck K+ every 2 hours" MIDDLE SECTION - "STEP 2: INSULIN INFUSION PROTOCOL" - Starting dose: Regular insulin IV infusion 0.1 units/kg/hour (NO IV bolus) - Target glucose drop: 2.8 to 3.9 mmol/L (50-70 mg/dL) per hour - If glucose NOT falling by 50-70 mg/dL in first hour → double the infusion rate - When glucose reaches 11-14 mmol/L (200-250 mg/dL) → ADD dextrose to IV fluid (D5W or D5 0.45% NaCl) to maintain glucose 8-11 mmol/L - KEEP insulin infusion running (do not stop) until ketoacidosis resolves LOWER SECTION - "STEP 3: RESOLUTION CRITERIA (when to transition off IV insulin)" Three criteria in green checkboxes: Blood glucose less than 11 mmol/L AND Bicarbonate greater than 15 mEq/L AND pH greater than 7.3 Then transition arrow: "Overlap IV insulin with subcutaneous insulin by 1-2 hours before stopping infusion" BOTTOM - "MONITORING FREQUENCY" table: - Glucose: every 1 hour - Electrolytes (K+, Na+, bicarb): every 2 hours for first 4 hours, then every 4 hours - ABG/VBG: every 2-4 hours - Urine output: hourly via catheter (target more than 0.5 mL/kg/hr) Footer warning box in red: "CAUTION: Serum K+ does NOT reflect total body K+. All DKA patients are total-body K+ depleted regardless of initial serum level. Aggressive K+ replacement is mandatory." Use clear arrows, boxes, and color coding. Make it readable as a wall-mounted clinical reference poster.