Clubbing full details for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the material needed for a comprehensive 10-mark MD exam answer on clubbing. Let me compile the full answer.
Clubbing (Digital Clubbing / Hippocratic Fingers)
Definition
Clubbing is the selective bulbous enlargement of the distal segments of the digits (fingers and toes) due to proliferation of connective tissue and an increase in soft tissue, particularly on the dorsal surface, accompanied by increased sponginess of the soft tissue at the base of the clubbed nail. The term is synonymous with "Hippocratic fingers," "drumstick fingers," and "watch-glass nails."
- Harrison's Principles of Internal Medicine 22e, p.41
Clinical Photo
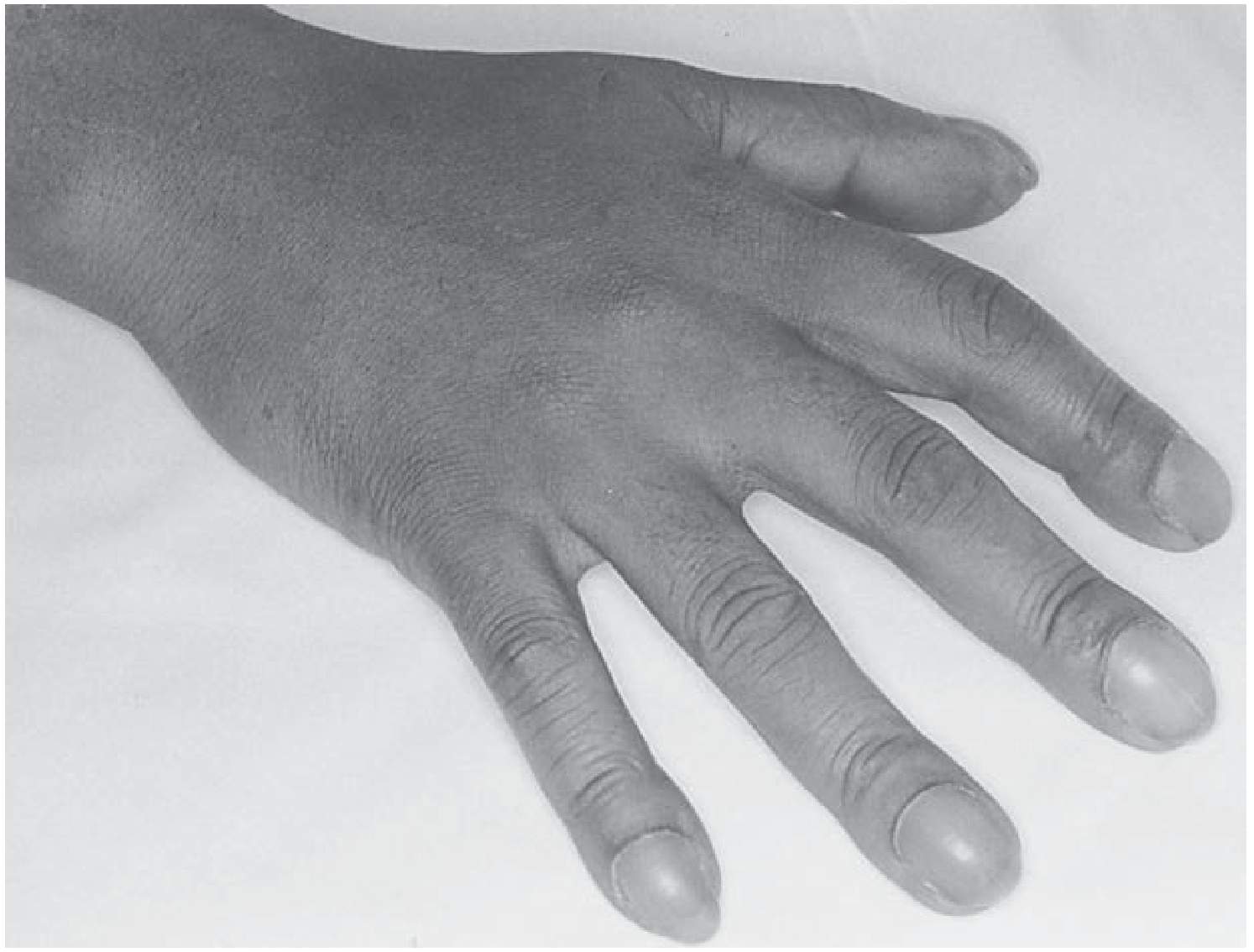
Clubbing of all fingers (Fishman's Pulmonary Diseases and Disorders)

Clubbing in Eisenmenger complex - watch-glass nails (Fitzpatrick's Dermatology)
Historical Note
The association between changes in the fingertips and serious disease was first described by Hippocrates in the context of empyema. It remains one of the oldest-recognized physical signs in medicine.
Clinical Features (Recognition)
When fully developed, clubbing has the following hallmarks (Murray & Nadel):
-
Increased Lovibond angle - The normal angle between the nail plate and the dorsal surface of the distal phalanx (Lovibond/hyponychial angle) is approximately 160 degrees. In clubbing, this angle is obliterated and becomes 180 degrees or greater.
-
Nail bed sponginess - Softening and perilingual erythema of the nail beds; the nail appears to "float" when pressure is applied to the matrix.
-
Bulging of the distal phalanx - Enlargement of the fingertip, which may be warm and erythematous. The undersurface of the terminal digit becomes large and bulbous.
-
Curvature of the nails - The nails become abnormally curved in both longitudinal and coronal (transverse) planes, resembling a watch glass. The lunula may appear enlarged.
-
Schamroth sign (Schamroth window test) - When the dorsal surfaces of the corresponding fingers of each hand are opposed (placed back-to-back at the nail beds), a diamond-shaped window is normally visible. In clubbing, this window is absent, and the angle between the free nail margins is greater than 30 degrees. This is the most practical bedside test; its validity and reliability have been confirmed (JAMA 2010;304:159).
- Andrews' Diseases of the Skin; Fitzpatrick's Dermatology; Murray & Nadel
Grading of Clubbing
| Grade | Features |
|---|---|
| Grade 1 | Fluctuation and softening of the nail bed (increased sponginess) |
| Grade 2 | Loss of normal angle between nail and nail fold (Lovibond angle obliterated, becomes ≥180°); positive Schamroth sign |
| Grade 3 | Increased convexity of the nail; beak-like/parrot-beak appearance |
| Grade 4 | Gross enlargement of the distal phalanx (drumstick/bulbous appearance) with periosteal proliferation - Hypertrophic Osteoarthropathy (HOA) |
Pathogenesis
The exact mechanism remains unknown; no suitable animal model exists. The leading theories are:
1. Humoral / Vascular Theory (most widely accepted)
A humoral vasodilator substance normally inactivated in the pulmonary capillaries escapes inactivation (due to bypass via pulmonary shunts, bronchial circulation, or hepatic arteriovenous fistulas). This substance reaches the digital circulation and causes:
- Vasodilation of digital vessels
- Formation of arteriovenous connections
- Increased hydrostatic pressure in capillaries and venules
- Transudation of fluid into the interstitium - causing the characteristic soft tissue proliferation
This accounts for clubbing in cyanotic congenital heart disease, pulmonary diseases with bronchial circulation proliferation, and hepatic cirrhosis with pulmonary AV anastomoses.
2. Growth Factor Theory (Megakaryocyte Hypothesis)
The prevailing hypothesis in dermatology (Fitzpatrick's): Megakaryocytes are incompletely degraded to normal-size platelets in diseased or bypassed lungs, and strand in the capillary network of the digits where they disintegrate and release platelet-derived growth factors (PDGF), vascular endothelial growth factor (VEGF), and other angiogenic factors, causing soft tissue proliferation and new vessel formation.
Histochemical studies (Atkinson and Fox) have confirmed increased VEGF, PDGF, HIF-1α, and HIF-2α with increased microvessel density in clubbed digits.
3. Neural Theory
Local neural factors: injury to a finger or median nerve can cause single-digit clubbing, suggesting a neural component in some cases.
- Murray & Nadel; Fishman's Pulmonary Diseases; Fitzpatrick's Dermatology
Causes / Etiology
Clubbing may be hereditary or acquired (secondary).
A. Not Associated with Overt Disease
- Hereditary / Familial clubbing - autosomal dominant; mutations in HPGD gene (15-hydroxyprostaglandin dehydrogenase) and SLCO2A1 (prostaglandin transporter)
- Sporadic / idiopathic
- Pachydermoperiostosis (primary hypertrophic osteoarthropathy)
B. Pulmonary (Most Common Cause)
- Lung cancer (most common acquired cause - especially peripheral adenocarcinoma; small cell carcinoma rarely)
- Bronchiectasis
- Lung abscess
- Empyema
- Cystic fibrosis
- Idiopathic pulmonary fibrosis (IPF)
- Asbestosis
- Mesothelioma
- Tuberculosis, sarcoidosis
- Pulmonary Langerhans cell histiocytosis
- Collagen vascular disease with lung involvement
Important: COPD does not cause clubbing. Clubbing in a COPD patient should prompt evaluation for a superimposed lung cancer.
C. Cardiac and Vascular
- Cyanotic congenital heart disease (e.g., Tetralogy of Fallot, Eisenmenger syndrome)
- Subacute bacterial endocarditis (SBE/IE)
- Infected aortic graft
- Pulmonary arteriovenous fistula
- Hereditary hemorrhagic telangiectasia (HHT)
- Takayasu's arteritis, Behçet syndrome
D. Gastrointestinal and Hepatic
- Inflammatory bowel disease (Crohn's disease, Ulcerative colitis)
- Hepatic cirrhosis
- Hepatopulmonary syndrome
- Biliary cirrhosis / hepatoma
- Polyposis coli
- Infectious bowel disease (amebic colitis, bacillary dysentery)
- Esophageal stricture
E. Other Systemic
-
Thyroid acropachy (Graves' disease)
-
Secondary hyperparathyroidism
-
HIV infection (~36% of HIV-infected patients)
-
Hemoglobinopathies, congenital methemoglobinemia
-
Fabry disease
-
Toxic exposure (arsenic, mercury, beryllium)
-
Prostaglandin infusion
-
Occupational (jackhammer operators)
-
Murray & Nadel's Respiratory Medicine; Harrison's 22e; Andrews' Dermatology; Fishman's Pulmonary
Special Patterns - Diagnostic Clues
| Pattern | Associated Condition |
|---|---|
| Differential / Unilateral clubbing | Vascular disorders - subclavian artery aneurysm, brachial AV fistula, median nerve injury, hemiplegia, local trauma, subluxation of shoulder |
| Clubbing of toes only (not fingers) | Patent ductus arteriosus with reversed shunt (differential cyanosis) |
| One-hand clubbing | Ipsilateral pulmonary sulcus (Pancoast) tumor invading brachial plexus |
| Rapid onset (within 2 weeks) | Empyema (also reverses within 2 weeks after treatment) |
Hypertrophic Osteoarthropathy (HOA)
Clubbing may progress to or be accompanied by HOA - a distinct clinical and radiological entity:
- Clinical: Pain and swelling of soft tissues over the distal ends of long bones; symmetric periarthritis at shoulders, knees, ankles, wrists, and elbows
- Radiology: Subperiosteal formation of new bone (periostitis) at the distal diaphyses of the radius, ulna, tibia, and fibula
- Investigations: Bone X-ray, MRI, or bone scan (99mTc-MDP shows periosteal uptake)
- Most common cause: Bronchogenic carcinoma (~5% incidence; peripheral > central; small cell carcinoma rarely)
- Also seen in: bronchiectasis, empyema, lung abscess, cystic fibrosis, mesothelioma, hepatic cirrhosis
- HOA is almost always associated with clubbing but clubbing does not always produce HOA
Investigations for Clubbing
- Chest X-ray - mandatory for all new-onset clubbing
- HRCT thorax - if CXR unrevealing (detect early malignancy or ILD)
- Echocardiography - for cyanotic heart disease, SBE
- Liver function tests / USG abdomen - for hepatic causes
- X-ray of hands - to detect periosteal new bone formation (HOA)
- Bone scan - sensitive for HOA
- Relevant blood tests: CBC, ESR, CRP, ANA, HIV serology
New-onset clubbing always warrants a chest radiograph and, if unrevealing, a CT scan. Clubbing was found in 1% of all medical admissions and was associated with serious disease in 40% of cases. - Murray & Nadel
Reversibility
Clubbing can regress:
- Within ~2 weeks of corrective cardiac surgery
- After successful treatment of empyema
- Following lung transplantation for cystic fibrosis
- After treatment of lung cancer (case reports)
Summary Box (for quick recall)
| Feature | Detail |
|---|---|
| Definition | Bulbous enlargement of distal digits due to connective tissue proliferation |
| Classic signs | Lovibond angle ≥180°, Schamroth window absent, spongy nail bed |
| Most common cause | Lung cancer (adults) |
| Cardiac cause | Cyanotic congenital heart disease |
| GI cause | IBD, hepatic cirrhosis |
| Does NOT cause clubbing | COPD, asthma, simple emphysema |
| Pathogenesis | Humoral vasodilator + growth factors (VEGF, PDGF) from platelets/megakaryocytes |
| Complication | Hypertrophic osteoarthropathy (HOA) |
| Reversible? | Yes - after treating cause |
Sources: Harrison's Principles of Internal Medicine 22e | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Andrews' Diseases of the Skin | Fitzpatrick's Dermatology
This is a shared conversation. Sign in to Orris to start your own chat.