Investigation for hypocortisolism
Reading File
Finding Sources
Finding Sources
Searching PubMed
"adrenal insufficiency" AND "diagnosis"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, authoritative information to construct a thorough answer. Let me compile this.
Investigation for Hypocortisolism (Adrenal Insufficiency)
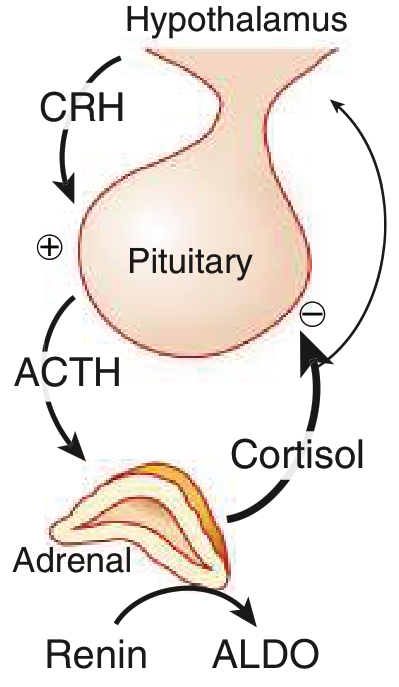
Hypocortisolism is categorized by the site of dysfunction within the hypothalamic-pituitary-adrenal (HPA) axis:
- Primary (adrenal gland failure — Addison disease)
- Secondary (pituitary ACTH deficiency)
- Tertiary (hypothalamic CRH deficiency)
The key clinical distinction is that primary disease causes mineralocorticoid deficiency (↑ renin, hyperkalemia, hyponatremia, hyperpigmentation), while central causes do not.
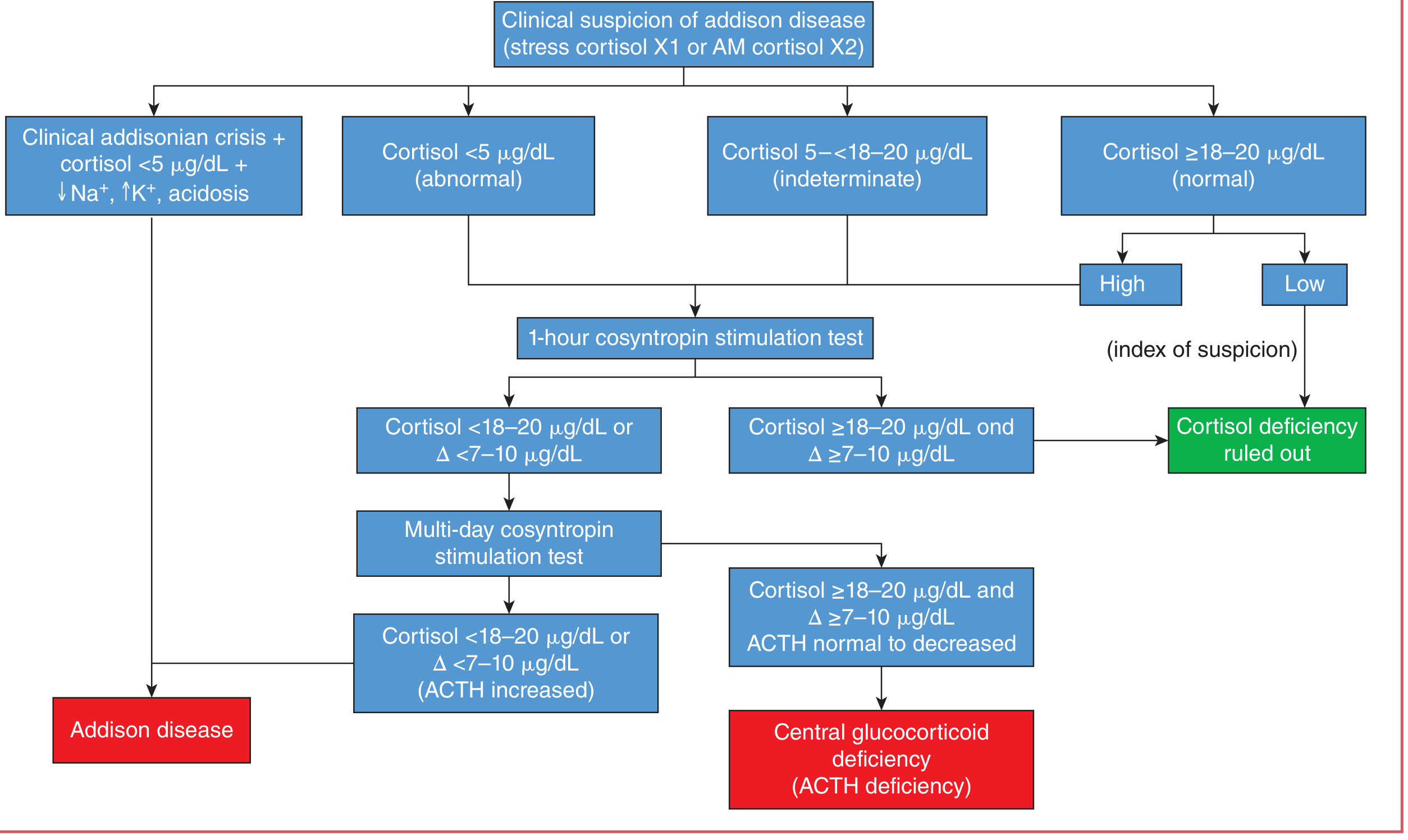
Step 1: Initial Screening — Morning Serum Cortisol
An 8–9 AM serum cortisol is the first-line screen:
| Result | Interpretation |
|---|---|
| > 18 μg/dL (500 nmol/L) | Adrenal insufficiency virtually excluded (low suspicion) |
| < 3 μg/dL (83 nmol/L) | Adrenal insufficiency highly likely — no further stimulation needed |
| 3–18 μg/dL | Indeterminate — proceed to dynamic testing |
In critical illness: random cortisol > 25 μg/dL makes adrenal insufficiency unlikely; < 10 μg/dL is strongly suggestive. — Henry's Clinical Diagnosis and Management by Laboratory Methods
Note: More specific assays (tandem mass spectrometry or monoclonal antibody-based immunoassays) use a lower "normal" cutoff of ~14 μg/dL post-stimulation. — Goldman-Cecil Medicine
Step 2: Standard (High-Dose) ACTH Stimulation Test (Short Synacthen Test)
The most convenient and widely used dynamic test. Can be performed at any time of day.
Protocol:
- Draw baseline serum cortisol (± plasma ACTH)
- Administer 250 μg cosyntropin (ACTH 1-24) IV or IM
- Measure serum cortisol at 30 and 60 minutes
Interpretation:
- Peak cortisol ≥ 18–20 μg/dL (500–550 nmol/L) = normal
- Peak cortisol < 18–20 μg/dL = adrenal insufficiency confirmed
- Also assess: increment (Δ) ≥ 7–10 μg/dL over baseline
Baseline plasma ACTH distinguishes type:
- High ACTH (> 50–100 pg/mL) → Primary adrenal insufficiency
- Low/normal ACTH (< 10 pg/mL) → Secondary or tertiary
Aldosterone response also helps: failure to increase aldosterone by > 4 ng/dL over baseline suggests primary adrenal dysfunction. — Henry's Clinical Diagnosis and Management by Laboratory Methods
Diagnostic Flowchart
Step 3: Low-Dose ACTH Stimulation Test (1 μg)
A 1 μg dose (given in the morning) is equally good for establishing the diagnosis but is less commonly used due to formulation difficulties that increase the risk of a falsely normal result. It may be more sensitive for mild or early secondary/tertiary adrenal insufficiency, where the adrenal gland retains some capacity to respond to a supraphysiologic dose (250 μg) but not a physiologic dose (1 μg). — Goldman-Cecil Medicine
Step 4: Prolonged (3-Day) ACTH Stimulation Test
Used when the standard test is abnormal but the cause (primary vs central) is uncertain:
- ACTH is administered daily for 3 days
- In secondary/tertiary adrenal insufficiency, the atrophied adrenals can be "primed" and will show a delayed but rising cortisol response
- In primary disease, no response occurs regardless — Henry's Clinical Diagnosis and Management by Laboratory Methods
Step 5: Tests for Secondary/Tertiary Adrenal Insufficiency
Insulin Tolerance Test (ITT) — Gold Standard for HPA Axis Integrity
- Insulin (0.1–0.15 U/kg IV) induces hypoglycemia (blood glucose < 2.2 mmol/L)
- Normal: cortisol rises to > 18–20 μg/dL
- Contraindicated in: epilepsy, ischemic heart disease, severe hypopituitarism
- Requires close medical supervision
- The cortisol response to hypoglycemia can be reliably predicted by the ACTH stimulation test — a safer, cheaper alternative — Henry's Clinical Diagnosis and Management
Overnight Metyrapone Test
- Metyrapone inhibits 11β-hydroxylase, blocking the final step of cortisol synthesis
- Cortisol ↓ → HPA axis is stimulated → 11-deoxycortisol (compound S) should rise
- Protocol: Metyrapone 30 mg/kg orally at midnight; measure cortisol + 11-deoxycortisol at 8 AM
- Normal: 11-deoxycortisol > 7 μg/dL (200 nmol/L)
- Abnormal (central AI): 11-deoxycortisol < 7 μg/dL + cortisol < 5 μg/dL
- Useful for mild/recent secondary AI that may respond normally to pharmacologic 250 μg ACTH
- ⚠️ May precipitate Addisonian crisis — use with caution; currently available only on compassionate basis in many countries — Henry's Clinical Diagnosis and Management by Laboratory Methods
CRH Stimulation Test
- Useful for localizing the defect (pituitary vs hypothalamic)
- 100 μg ovine CRH IV → measure ACTH and cortisol every 15 min for 60–90 min
- Normal: cortisol > 20 μg/dL; ACTH peaks at 15–30 min
- In pituitary disease: blunted ACTH and cortisol response
- In hypothalamic disease: ACTH may still rise (pituitary intact), cortisol may be subnormal — Henry's Clinical Diagnosis and Management by Laboratory Methods
Step 6: Localisation and Aetiology Workup
For Primary Adrenal Insufficiency:
| Test | Purpose |
|---|---|
| 21-hydroxylase antibodies | Confirms autoimmune adrenalitis (most common cause in West) |
| Plasma very long chain fatty acids (C26:0) | Screens for adrenoleukodystrophy (especially in males with negative antibodies) |
| CT/MRI adrenals | Enlarged glands → TB, fungal infection, hemorrhage, metastases; Small glands → autoimmune |
| Renin + aldosterone | Elevated renin, low aldosterone confirms mineralocorticoid deficiency in primary AI |
| APS screening | For confirmed autoimmune AI: screen thyroid (TSH), blood glucose (T1DM), calcium (hypoparathyroidism) |
For Secondary/Tertiary Adrenal Insufficiency:
| Test | Purpose |
|---|---|
| MRI pituitary/hypothalamus | Exclude structural lesion (tumor, infiltration, pituitary stalk disruption) |
| Full pituitary hormone panel | TSH/fT4, LH/FSH, GH/IGF-1, prolactin — exclude panhypopituitarism |
| Drug history | Prolonged glucocorticoid use (most common cause), opiates, ketoconazole, etomidate, rifampicin |
Additional Biochemical Pointers
| Finding | Suggests |
|---|---|
| Hyponatremia + hyperkalemia | Primary AI (mineralocorticoid deficiency) |
| Hyponatremia alone (without hyperkalemia) | Secondary AI (SIADH-like picture) |
| Hypoglycemia | Both primary and secondary AI |
| Eosinophilia | Classically associated with primary AI |
| Hyperpigmentation | Primary AI (↑↑ ACTH → MSH activity) |
HPA Axis Physiology (Normal)
Special Situations
Critical illness: Total serum cortisol may be misleadingly low due to reduced CBG. Free cortisol index (FCI) or calculated free cortisol (CFC) better reflect true cortisol status. Withhold formal testing, give dexamethasone (does not cross-react with cortisol assays), and test within 72 hours.
Pregnancy: Cortisol-binding globulin rises progressively; higher cutoffs apply — morning cortisol < 11/16/22 μg/dL and post-ACTH cortisol < 25/29/32 μg/dL (1st/2nd/3rd trimester) are diagnostic thresholds. — Henry's Clinical Diagnosis and Management by Laboratory Methods
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods | Goldman-Cecil Medicine | Tietz Textbook of Laboratory Medicine, 7th ed. | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.