A child present with visual disturbances and delayed growth. Imaging shows suprasellar mass and histopathology shows wet keratin. Most probable diagnosis is ?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Diagnosis: Craniopharyngioma (Adamantinomatous Type)
The triad of suprasellar mass + visual disturbances + delayed growth in a child + wet keratin on histology is classic for adamantinomatous craniopharyngioma. This is one of the highest-yield pathology findings in exam settings.
Why this diagnosis fits perfectly
| Feature | Explanation |
|---|---|
| Child | Adamantinomatous type has a bimodal age peak - one in childhood (5-15 years), one in older adults. The papillary type is almost exclusively adult. |
| Suprasellar location | Most craniopharyngiomas are suprasellar (arising from Rathke's pouch remnants), often encroaching on the optic chiasm and hypothalamus. |
| Visual disturbances | Compression of the optic chiasm produces bitemporal hemianopia - the hallmark visual defect. |
| Delayed/retarded growth | The mass compresses the hypothalamus and anterior pituitary, causing GH deficiency and secondary pituitary hypofunction. |
| Wet keratin | Compact, lamellar "wet keratin" (ghostlike nests of dead keratinocytes) is pathognomonic for adamantinomatous craniopharyngioma. As Robbins states, it is a diagnostic feature even without viable epithelium on biopsy. |
Histopathology of Adamantinomatous Craniopharyngioma
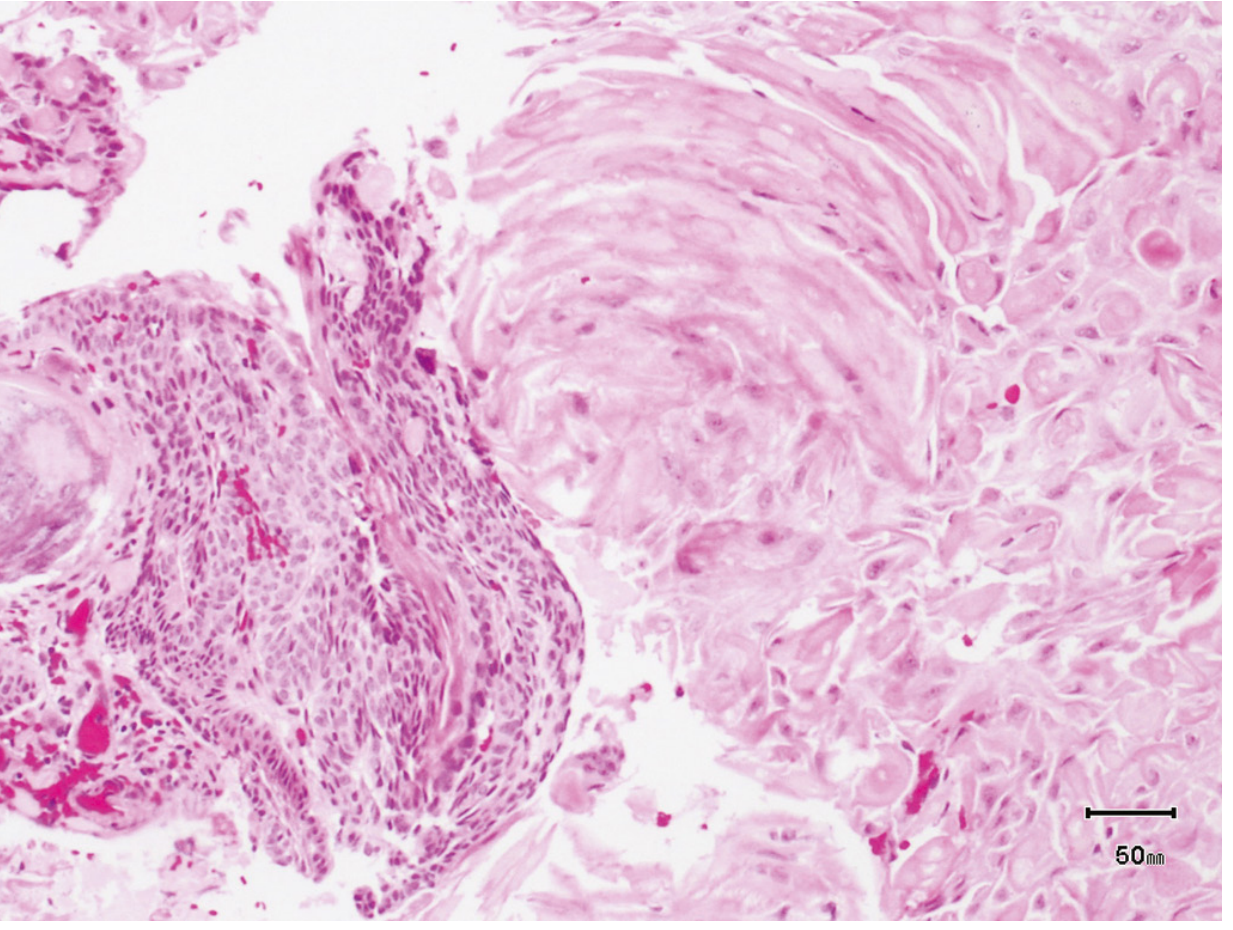
H&E: Left - nests of squamous epithelium with peripheral palisading; Right - the large swirling mass of compact lamellar "wet keratin".
Key microscopic features include:
- Nests/cords of stratified squamous epithelium with peripheral palisading
- Stellate reticulum - central cobweb-like loosening
- Wet keratin - compact, lamellar, ghostlike keratinocyte nests (unique to this tumor)
- Dystrophic calcification (seen in ~75% of cases; radiologically demonstrable)
- Cysts filled with a thick, dark, cholesterol-rich fluid likened to "machine oil"
- Finger-like microscopic extensions into adjacent brain with brisk glial reaction
Wet Keratin - The Pathognomonic Clue
"Wet keratin differs from the dry, flaky keratin of epidermoid and dermoid cysts and is unique to craniopharyngioma. Therefore, it is diagnostic on biopsy, even without the presence of viable epithelium."
- Bradley and Daroff's Neurology in Clinical Practice
Molecular Marker
- CTNNB1 (β-catenin) mutation in ~92-94% of adamantinomatous craniopharyngiomas - leads to aberrant Wnt signaling activation.
- The papillary variant instead carries BRAF V600E mutations and responds to BRAF inhibitors.
Quick Comparison
| Feature | Adamantinomatous | Papillary |
|---|---|---|
| Age | Children (and older adults) | Adults |
| Location | Suprasellar | Often 3rd ventricle |
| Calcification | Common (~75%) | Rare |
| Wet keratin | Yes - diagnostic | No |
| Cysts ("machine oil") | Yes | No |
| Mutation | CTNNB1 (β-catenin) | BRAF V600E |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 882-884; Bradley and Daroff's Neurology in Clinical Practice, p. 431-435
This is a shared conversation. Sign in to Orris to start your own chat.