PREPATELLAR BURSITIS USG
Reading File
Finding Sources
Finding Sources
Searching PubMed
"prepatellar bursitis" AND ultrasound
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
I now have comprehensive information. Let me compile the full detailed answer.
Prepatellar Bursitis - Ultrasound (USG)
Anatomy
The prepatellar bursa lies between the patella and the overlying skin (subcutaneous layer). It is a superficial bursa that does not communicate with the knee joint space - a point of major diagnostic importance on USG. The image below shows its exact location relative to the other bursae of the knee:
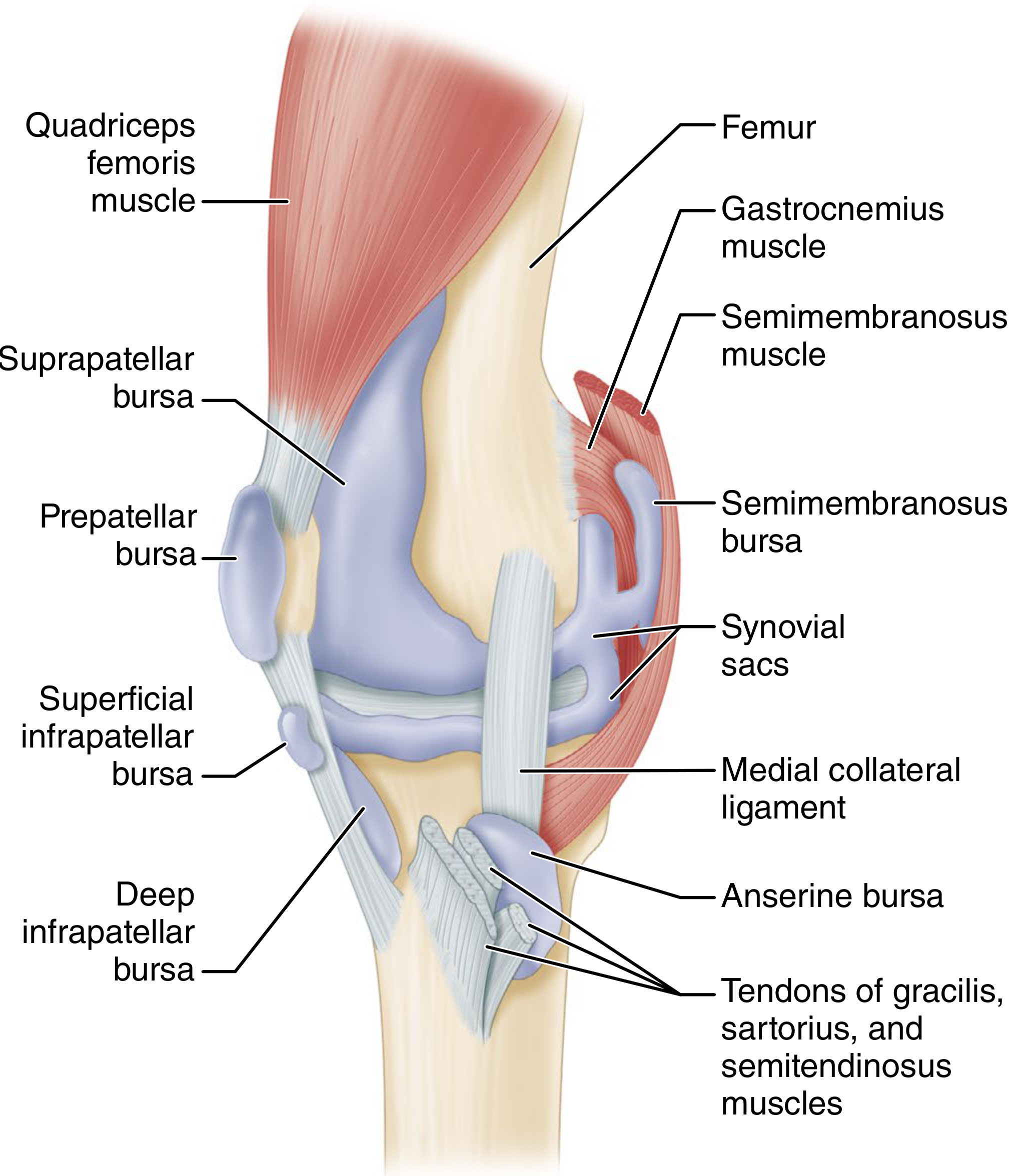
Fig. 10.6 - Multiple bursae around the knee that may become acutely or chronically inflamed (Campbell's Operative Orthopaedics, 15th Ed)
USG Technique
- Transducer: High-frequency linear probe - 7.5 to 10 MHz (maximum resolution for superficial structures)
- Position: Longitudinal orientation, indicator pointing toward the patient's head, placed over the anterior aspect of the knee
- Key landmark: The patella appears as a brightly echogenic (white) arcing line with posterior acoustic shadowing just beneath the surface
"Locating the patella is key to distinguishing prepatellar bursitis, which will appear as a dark, fluid-filled collection superficial to the patella, and a joint effusion, which will appear as a dark, fluid-filled collection deep to the patella."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
USG Findings in Prepatellar Bursitis
1. Fluid Collection (Anechoic/Hypoechoic)
- Appears as a dark gray to black (anechoic/hypoechoic) fluid-filled collection located superficial to the patella
- This is the hallmark finding distinguishing it from a joint effusion (which is deep to the patella)
- Simple uncomplicated fluid = anechoic (purely black)
2. Septic / Infective Bursitis Findings
- Excess fluid in the bursa (may appear more echogenic/complex due to debris, pus, or fibrin)
- Wall thickening of the bursal sac
- Increased colour Doppler flow within and around the bursal wall - due to hyperaemia and inflammatory changes
- The image below shows infective bursitis with colour Doppler:
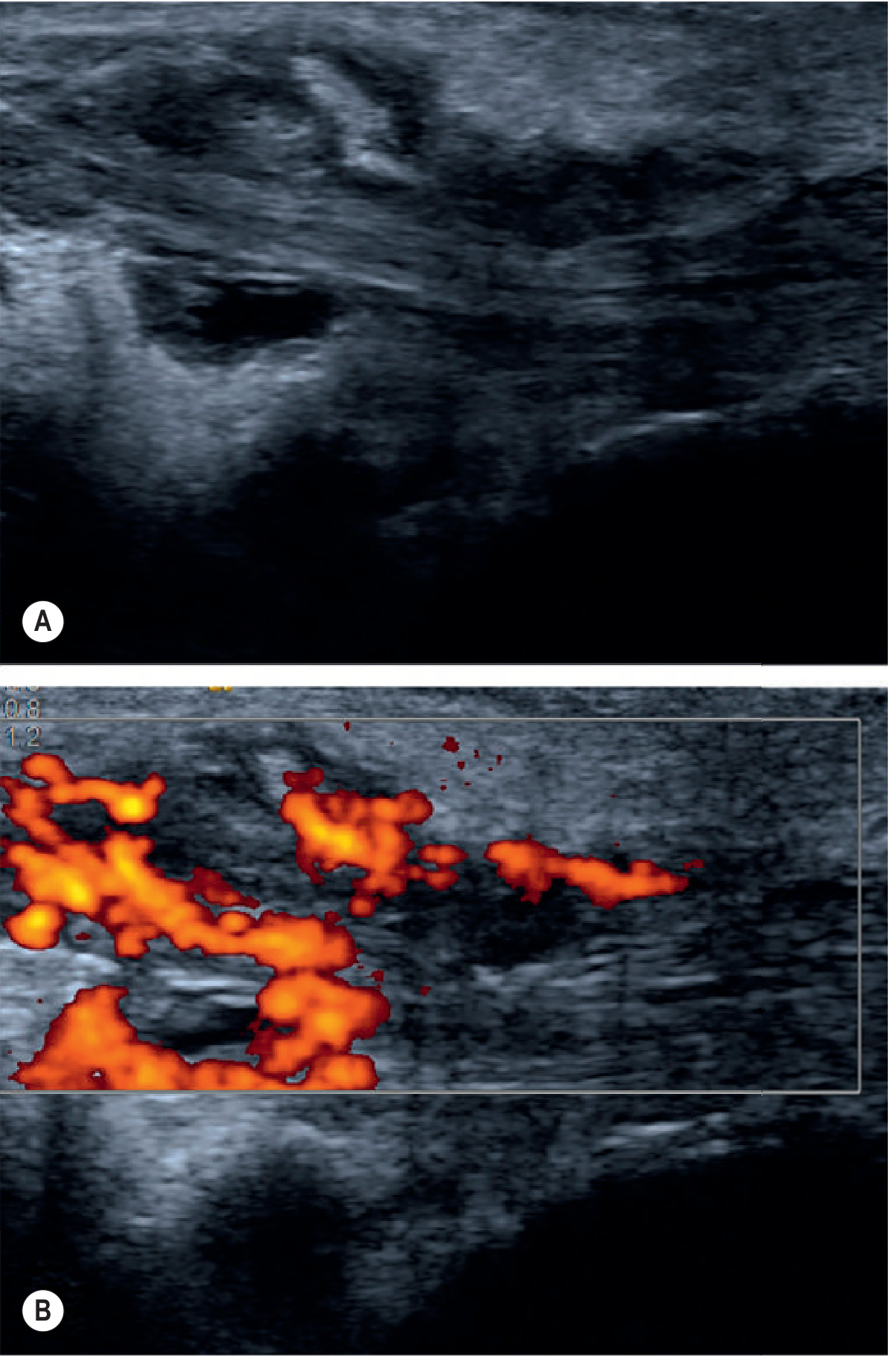
Fig. 46.8 - Ultrasound of inflammatory/infective bursitis: (A) grayscale - irregular fluid collection; (B) colour Doppler - markedly increased flow indicating active inflammation (Grainger & Allison's Diagnostic Radiology)
3. Chronic / Traumatic Bursitis Findings
- Bursal wall thickening and synovial proliferation
- Fluid may contain internal echoes (fibrin strands, debris)
- Possible nodules within the bursa (fibrotic synovial nodules)
- Compressibility of the collection on pressure
4. Calcific Bursitis
- Presence of hyperechoic foci (bright spots) with or without posterior shadowing within the bursa
- Associated with chronic or crystal-related disease (gout, CPPD)
USG Differential Diagnosis at the Patella
| Feature | Prepatellar Bursitis | Joint Effusion | Cellulitis |
|---|---|---|---|
| Location | Superficial to patella | Deep to patella (suprapatellar) | Subcutaneous tissue |
| Echogenicity | Anechoic/complex fluid | Anechoic fluid | Cobblestone pattern (echogenic strands in oedematous tissue) |
| Wall | Bursal sac visible | Synovial lining | No sac |
| Doppler | Increased in septic | Variable | Increased in superficial vessels |
| Communication with joint | No | Yes | No |
Cellulitis appears as oedema and thickening of subcutaneous tissues creating a "cobblestone pattern" due to anechoic strands randomly traversing the subcutaneous tissues - Grainger & Allison's
USG-Guided Aspiration
USG plays a dual role - diagnostic and therapeutic:
- Guides needle aspiration of bursal fluid for Gram stain, culture, and crystal analysis (to distinguish septic from non-septic bursitis)
- Approximately one-third of patients with prepatellar bursitis have septic bursitis, making this distinction clinically important
- Aspiration fluid should be sent for: WBC count, Gram stain, culture, and polarized microscopy for crystals
- Colour Doppler can identify vascular supply before needle placement
- Real-time guidance reduces risk of inadvertent joint penetration
Key Points Summary
| Parameter | Finding |
|---|---|
| Transducer | High-frequency linear, 7.5-10 MHz |
| Location of fluid | Superficial to patella (anterior surface) |
| Simple fluid | Anechoic (black) |
| Complex/septic fluid | Echogenic with debris, wall thickening |
| Colour Doppler (active inflammation) | Markedly increased peribursal flow |
| Key differentiating point | Superficial (not deep) to patella |
| USG role | Diagnosis + guided aspiration |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Knee USG section
- Grainger & Allison's Diagnostic Radiology, p. 1187
- Harrison's Principles of Internal Medicine 22E (2025), Bursitis
- Campbell's Operative Orthopaedics 15th Ed (2026), p. 593
- Rosen's Emergency Medicine, Olecranon and Prepatellar Bursitis
PREPATELLAR BURSITIS USG IMGAES
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the key images. Let me compile the full image-rich response.
Prepatellar Bursitis - USG Images
IMAGE 1: Anatomy - Location of the Prepatellar Bursa
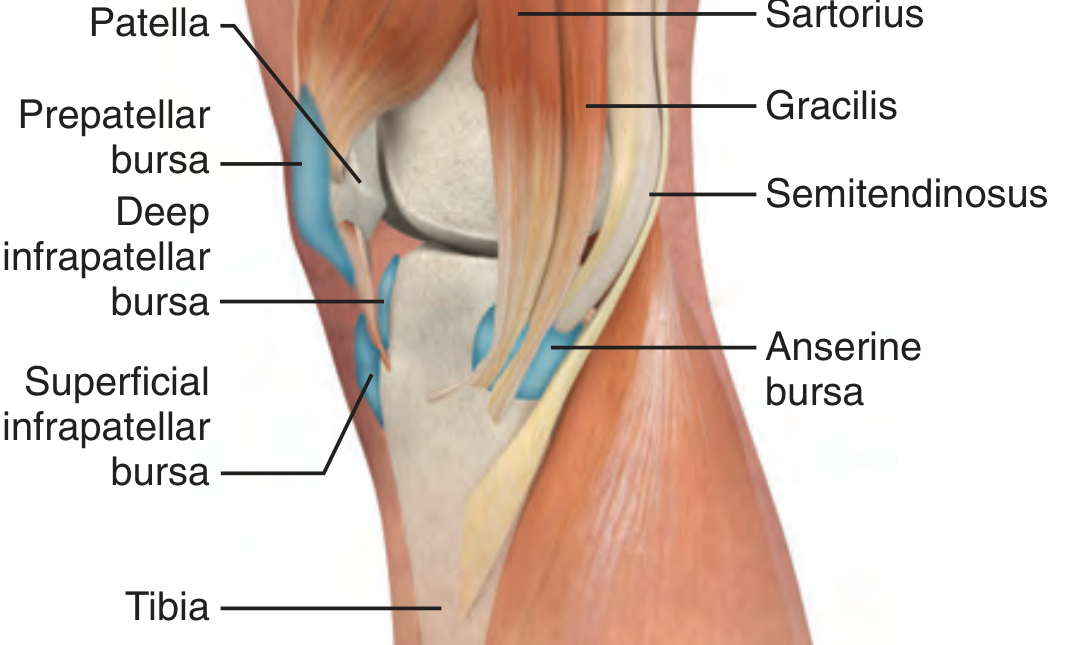
Fig. 52.26 - Bursae of the knee (medial view). The prepatellar bursa lies anterior to the patella between the skin and the patellar surface. Note its superficial position compared to the deep infrapatellar and anserine bursae.
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
IMAGE 2: Clinical Appearance - Septic Prepatellar Bursitis

FIGURE 284-12 - Septic prepatellar bursitis. This patient presented with obvious purulence of the right prepatellar bursal sac. Aspiration confirmed septic bursitis. Note the well-circumscribed, tense swelling localized anterior to the patella - the hallmark clinical feature that distinguishes it from a joint effusion.
(Tintinalli's Emergency Medicine)
IMAGE 3: USG Appearance - Infective Bursitis (Greyscale + Colour Doppler)
Fig. 46.8 - Infective bursitis on USG:
- (A) Greyscale B-mode: Irregular, predominantly hypoechoic/anechoic fluid collection within the bursa. Wall thickening is visible at the margins.
- (B) Colour Doppler: Markedly increased colour Doppler flow in the bursal wall and peribursal tissue - indicates active inflammation/infection (hyperaemia). This is the key feature distinguishing infective from simple traumatic bursitis.
(Grainger & Allison's Diagnostic Radiology)
IMAGE 4: Step-by-Step Aspiration Procedure
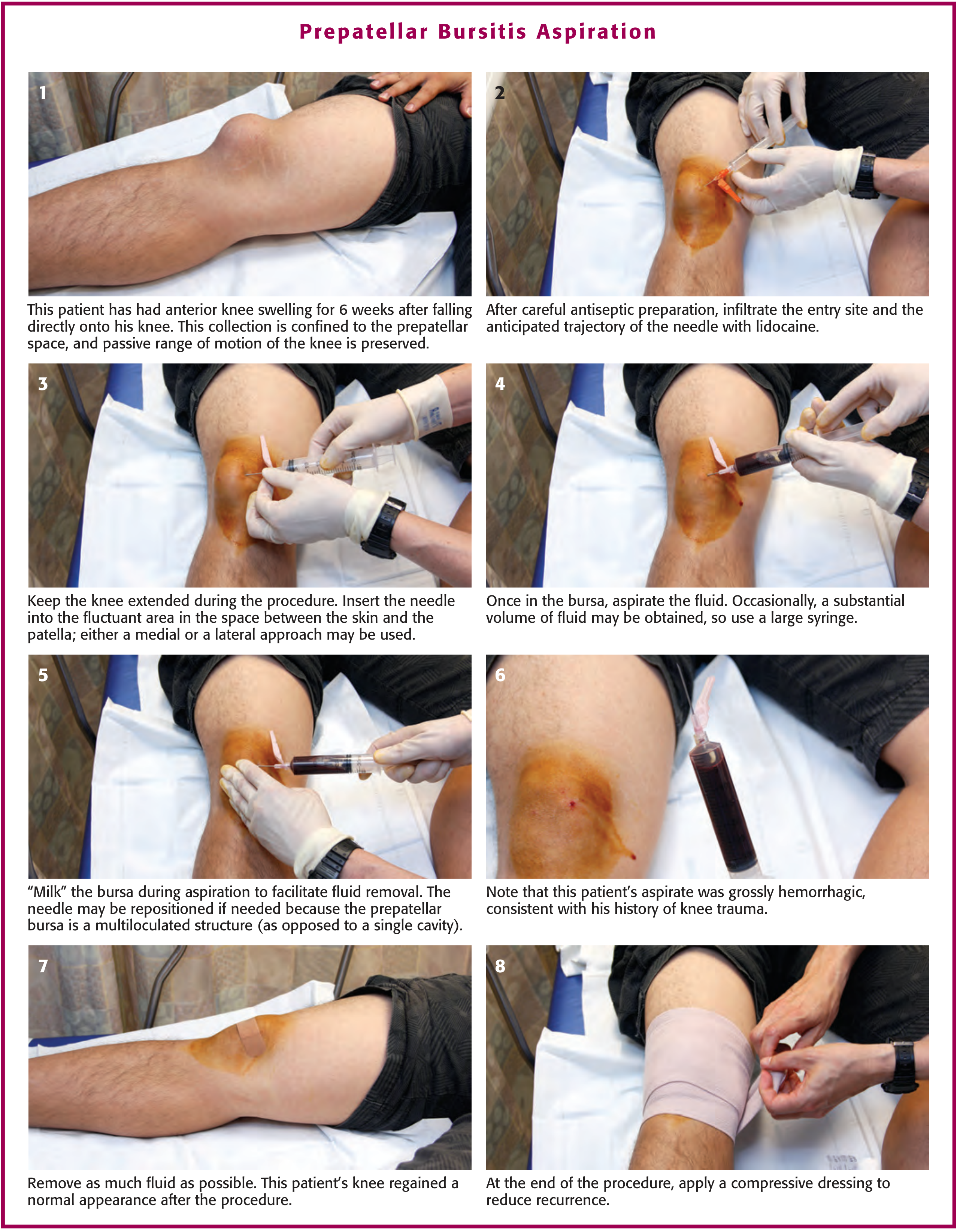
Figure 52.27 - Prepatellar Bursitis Aspiration (step-by-step):
- Anterior knee swelling confined to the prepatellar space, passive ROM preserved
- Antiseptic prep + lidocaine infiltration of entry site
- Knee extended, needle inserted into the fluctuant prepatellar space (medial or lateral approach)
- Aspiration - use large syringe (substantial fluid volume possible)
- "Milk" the bursa during aspiration - the prepatellar bursa is multiloculated, not a single cavity
- Aspirate may be hemorrhagic (post-trauma) or purulent (septic)
- Knee regains normal contour post-aspiration
- Apply compressive dressing to reduce recurrence
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
USG Key Findings Summary (What to Look for on Scan)
| Feature | Finding |
|---|---|
| Probe | High-frequency linear 7.5-10 MHz |
| Location of fluid | Superficial to patella (skin-patella space) |
| Simple/traumatic fluid | Anechoic (black), thin-walled, compressible |
| Complex/septic fluid | Hypoechoic with internal echoes, debris, fibrin strands |
| Wall | Thickened bursal wall in chronic/septic cases |
| Colour Doppler | Markedly increased flow in septic/inflammatory bursitis |
| Key differential | Joint effusion = fluid deep to patella (suprapatellar pouch) |
| Compressibility | Bursal fluid is compressible; a solid mass is not |
"The patella can be seen as a brightly echogenic (white) object with posterior shadowing. Prepatellar bursitis will appear as a dark, fluid-filled collection superficial to the patella, and a joint effusion will appear as a dark, fluid-filled collection deep to the patella."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Sources: Grainger & Allison's Diagnostic Radiology | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Tintinalli's Emergency Medicine | Campbell's Operative Orthopaedics 15th Ed (2026)
INFRAPATELLAR BURSITIS USG
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the key images and content. Let me compile the comprehensive image-rich answer.
Infrapatellar Bursitis - USG Images & Findings
Types of Infrapatellar Bursae
There are two distinct infrapatellar bursae - each with different anatomy, USG appearance, and clinical significance:
| Superficial Infrapatellar Bursa | Deep Infrapatellar Bursa | |
|---|---|---|
| Location | Anterior to the mid-portion of patellar tendon, in superficial soft tissues | Between the posterior margin of the distal patellar tendon and the anterior proximal tibia, inferior to Hoffa's fat pad |
| Communication with joint | No | No |
| Common cause | Friction/repetitive trauma | Osgood-Schlatter disease, overuse, spondyloarthritis |
| Also called | "Clergyman's knee" | "Deep patellar bursitis" / "Jumper's bursa" |
IMAGE 1: Anatomy - Both Infrapatellar Bursae in Context
Fig. 10.6 - Anatomy of knee bursae. Note the superficial infrapatellar bursa (anterior to the mid-patellar tendon) and the deep infrapatellar bursa (posterior to the distal patellar tendon, between tendon and tibial tuberosity). Both are separate from the prepatellar bursa above.
(Campbell's Operative Orthopaedics, 15th Ed 2026)
IMAGE 2: USG - Normal Patellar Tendon with Trace Deep Infrapatellar Fluid (Longitudinal View)
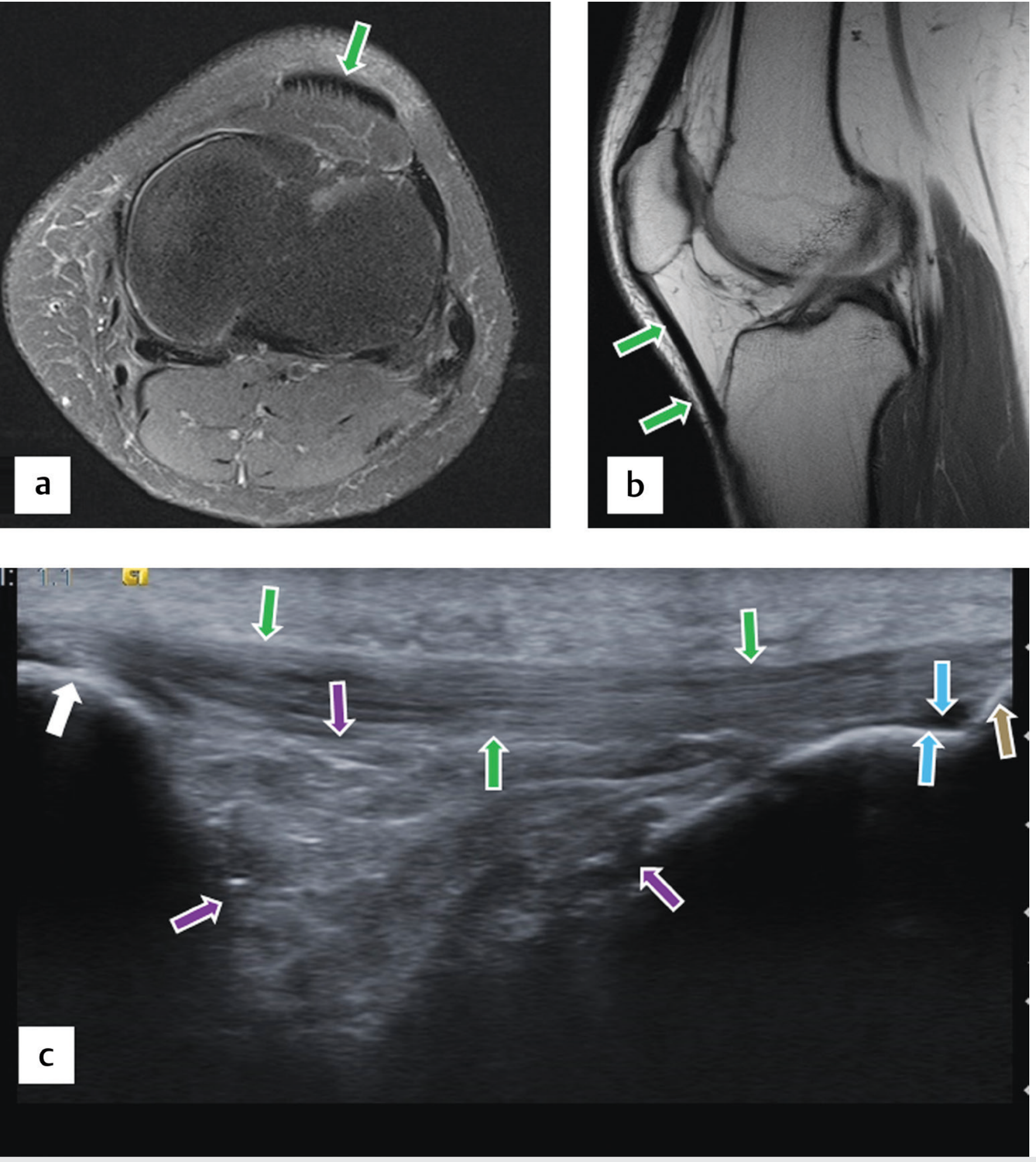
Fig. 21.34 - (a) Axial T2FS MRI, (b) Sagittal PD MRI, (c) Longitudinal USG of patellar tendon (key USG image):
On the USG scan (image c):
- Green arrows = patellar tendon - appears as multiple hyperechoic (bright) fibrillar bundles running longitudinally
- White arrow = patella (at left/proximal end) - brightly echogenic with acoustic shadowing
- Brown arrow = tibial tuberosity (at right/distal end) - echogenic bony landmark
- Purple arrows = Hoffa's infrapatellar fat pad - intermediate echogenicity, sits deep to the tendon
- Blue arrows = trace fluid in the deep infrapatellar bursa - small anechoic/hypoechoic collection at the posterior aspect of the distal patellar tendon, just above the tibial tuberosity
"The patellar tendon is visible as multiple hyperechoic bundles extending from the patella toward the tibial tuberosity. Hoffa's infrapatellar fat pad and trace fluid in the deep infrapatellar bursa are also present." (Imaging Anatomy: Bones, Joints, Vessels and Nerves)
IMAGE 3: Fat Pads and Normal Deep Infrapatellar Bursa - MRI Reference
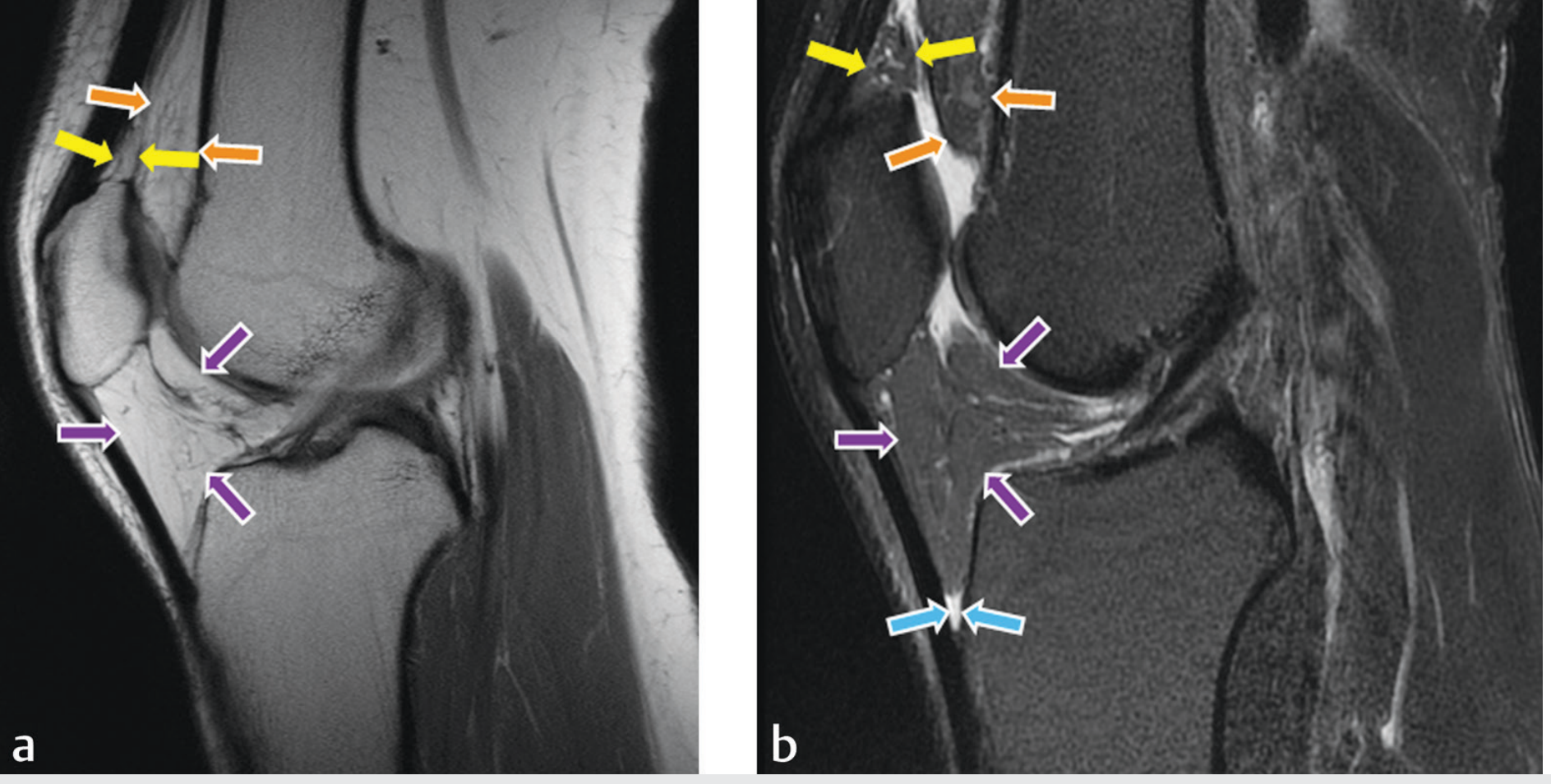
Fig. 21.35 - Sagittal MRI views showing normal fat pads and the deep infrapatellar bursa (blue arrows) located between the patellar tendon and proximal tibia:
- Yellow arrows = suprapatellar fat pad
- Orange arrows = prefemoral fat pad
- Purple arrows = infrapatellar (Hoffa's) fat pad
- Blue arrows = normal deep infrapatellar bursa - the small potential space that becomes distended in bursitis
(Imaging Anatomy: Bones, Joints, Vessels and Nerves)
IMAGE 4: Superficial Infrapatellar Bursitis - MRI
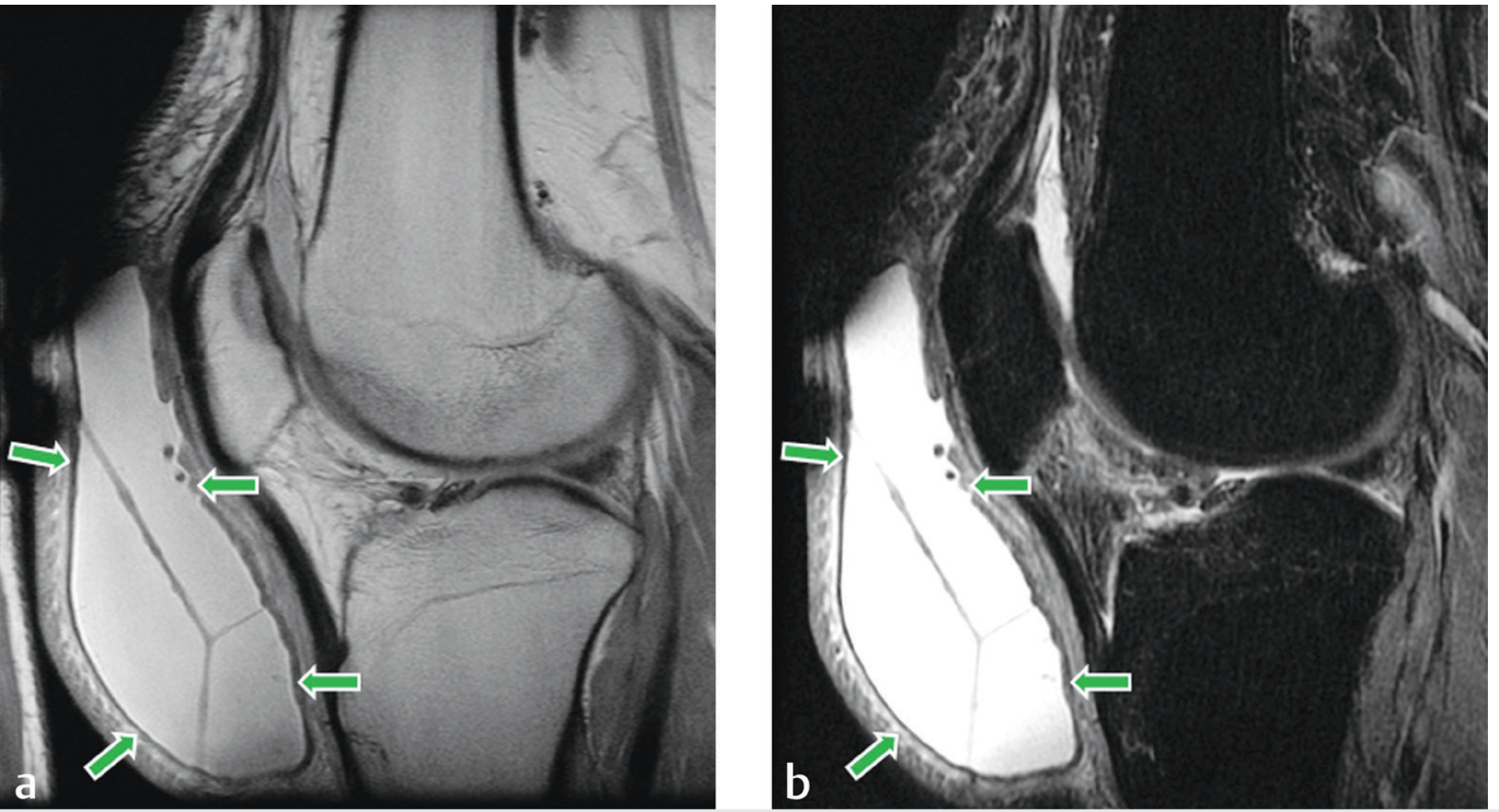
Fig. 21.38 - Superficial infrapatellar bursitis (green arrows):
- (a) Sagittal PD: fluid collection anterior to the mid-portion of patellar tendon, with internal septations visible
- (b) Sagittal STIR: bright high-signal fluid confirms active bursitis with septations
"When large, this bursitis can be indistinguishable from prepatellar bursitis."
On USG: appears as a compressible, hypoechoic/anechoic fluid collection anterior to the patellar tendon, with possible internal echoes and septations in chronic cases.
(Imaging Anatomy: Bones, Joints, Vessels and Nerves)
IMAGE 5: Deep Infrapatellar Bursitis - MRI
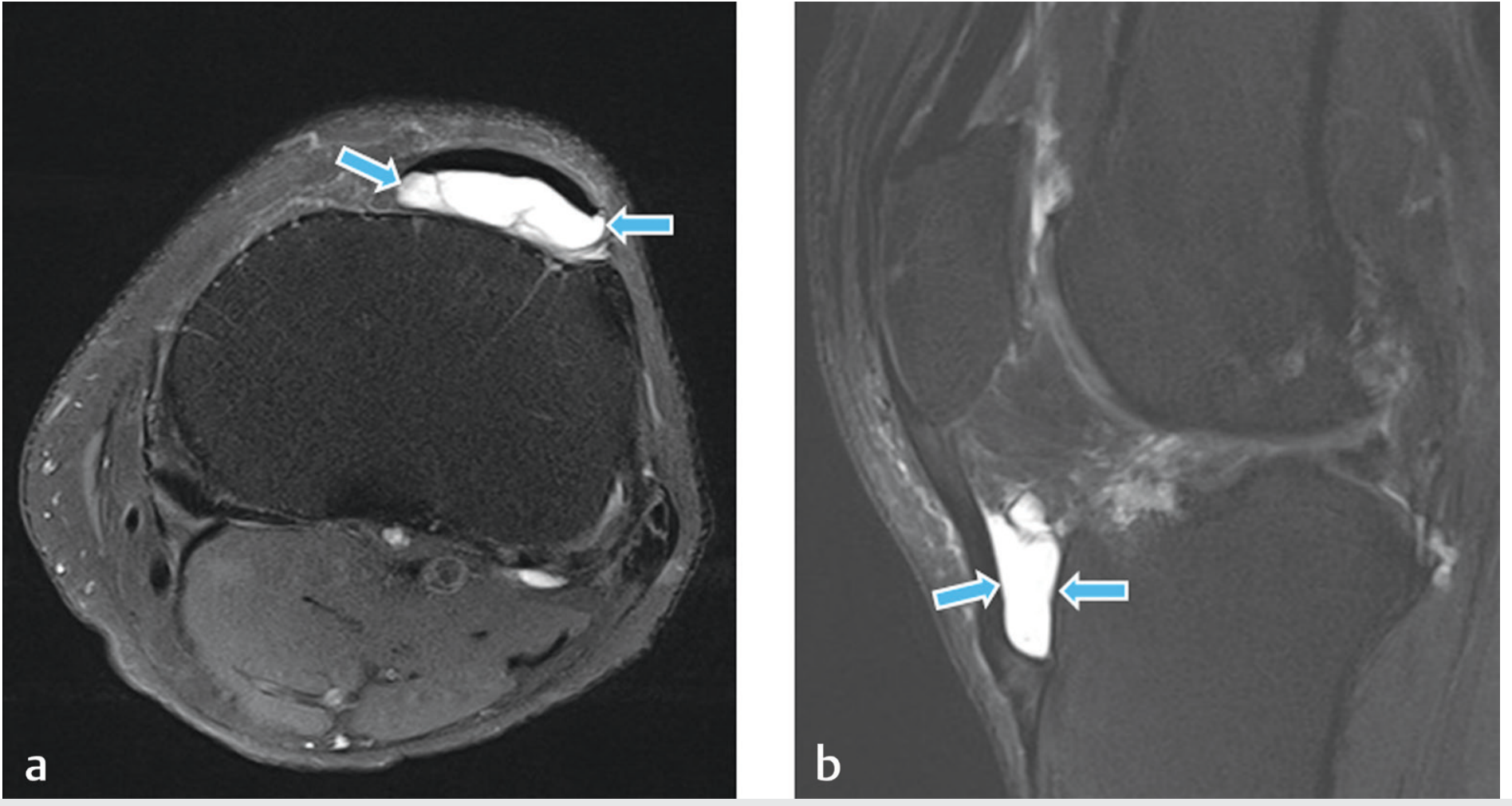
Fig. 21.39 - Deep infrapatellar bursitis (blue arrows):
- (a) Axial PD-FS: thin, low-signal capsule containing bright high-signal fluid with septations - located posterior to the patellar tendon at the tibial insertion
- (b) Sagittal T2FS: well-defined fluid collection between the posterior distal patellar tendon and anterior tibia, with an internally-septated pattern
On USG equivalent appearance:
- Hypoechoic/anechoic fluid collection posterior to the distal patellar tendon
- Thin echogenic capsule
- Internal septations in chronic cases
- Located in the space between patellar tendon and tibial tuberosity (Hoffa's fat pad may appear compressed or displaced)
- No communication with the knee joint
(Imaging Anatomy: Bones, Joints, Vessels and Nerves)
USG Technique for Infrapatellar Bursae
| Parameter | Recommendation |
|---|---|
| Probe | High-frequency linear, 7.5-15 MHz |
| Patient position | Supine, knee slightly flexed (15-20°) or extended |
| Scan plane | Longitudinal (sagittal) as primary; add transverse for width assessment |
| Key landmark | Patellar tendon - traces from inferior pole of patella to tibial tuberosity |
| Superficial infrapatellar bursa | Scan superficial to the mid-patellar tendon |
| Deep infrapatellar bursa | Scan deep/posterior to the distal patellar tendon, just proximal to tibial tuberosity |
| Colour Doppler | Add to assess hyperaemia in active/septic bursitis |
USG Findings Summary
| Feature | Superficial Infrapatellar Bursitis | Deep Infrapatellar Bursitis |
|---|---|---|
| Location on USG | Anterior to mid-patellar tendon | Posterior to distal patellar tendon / above tibia |
| Echogenicity | Anechoic (simple) or complex | Anechoic (simple) or complex with septations |
| Wall | Thin; thickened if chronic/septic | Thin low-echogenicity capsule |
| Doppler | Increased in active inflammation | Increased in active inflammation |
| Hoffa fat pad | Not displaced | May be compressed/displaced |
| Associated findings | May mimic prepatellar bursitis | Associated with Osgood-Schlatter (tibial tuberosity irregularity), patellar tendon insertional thickening |
| Joint communication | None | None |
Clinical Notes for USG
- The infrapatellar bursa lies deeper and more distal than the prepatellar bursa - the patellar tendon itself acts as the anterior boundary
- In Osgood-Schlatter disease, USG will also show: pretibial soft-tissue swelling, fragmentation of the tibial ossification center, and insertional thickening of the patellar tendon alongside bursal distension
- The deep infrapatellar bursa is separated from the knee joint synovium by Hoffa's fat pad - a sterile effusion of the knee joint may coexist but should not be confused with infrapatellar infection
- A distended deep infrapatellar bursa "obliterates the normal depression on each side of the patellar tendon" - this is the clinical sign that USG confirms
Sources:
- Imaging Anatomy: Bones, Joints, Vessels and Nerves (Thieme), Figs. 21.34, 21.35, 21.38, 21.39
- Campbell's Operative Orthopaedics 15th Ed (2026), p. 595
- Grainger & Allison's Diagnostic Radiology
- Rosen's Emergency Medicine, Osgood-Schlatter Syndrome
- Goldman-Cecil Medicine, Bursitis and Tendinitis
I NEED USG IMAGES OF INFRAPATELLAR BURSITIS
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
This is a shared conversation. Sign in to Orris to start your own chat.