Pancreatitis
Reading File
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Finding Sources
Searching PubMed
acute pancreatitis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full, detailed response.
Pancreatitis
Pancreatitis is inflammation of the pancreas that results from inappropriate activation of digestive enzymes within the gland, leading to autodigestion. It spans a spectrum from mild, self-limited disease to life-threatening necrotizing pancreatitis with multi-organ failure.
1. Classification
Acute Pancreatitis (AP)
The Revised Atlanta Classification (2008) defines two morphological types:
- Interstitial oedematous pancreatitis - proteolytic enzymes injure the acinar cell, causing oedema and swelling but not necrosis. This constitutes 70-80% of cases and is generally self-limiting.
- Necrotising pancreatitis - the inflammatory response is strong enough to induce cell apoptosis and fat necrosis, which spreads to the pancreatic parenchyma. Necrosis is the major determinant of morbidity and mortality.
Severity is classified as:
- Mild - no organ failure, no local/systemic complications
- Moderately severe - transient organ failure (<48 hours) and/or local complications
- Severe - persistent organ failure (>48 hours), mortality ~29.5%
Chronic Pancreatitis (CP)
Permanent pathological damage resulting in progressive exocrine and endocrine insufficiency, chronic pain, and structural changes (calcifications, ductal strictures).
2. Etiology
Acute Pancreatitis
The causes are diverse. The most common in adults are:
| Cause | Frequency |
|---|---|
| Gallstones / biliary sludge / microlithiasis | >50% |
| Alcohol | ~30% |
| Hypertriglyceridemia (TG >1000 mg/dL) | <5% |
| Medications | <5% |
| Trauma, ERCP, neoplasm, infection, metabolic | <15% combined |
| Idiopathic | ~5% |
Key points:
- Gallstone pancreatitis is caused by transient or sustained impaction of sludge or a stone within the common channel of the ampulla of Vater
- Hypertriglyceridemia should be considered the etiology when serum TG >1000 mg/dL with no cholelithiasis or significant alcohol use
- Pancreatic neoplasm must be considered on the differential in anyone >40 years
- Post-ERCP pancreatitis occurs in 5-10%, rising to >20% with risk factors (young age, suspected sphincter of Oddi dysfunction, failed/difficult cannulation, pancreatic guidewire placement, history of prior post-ERCP pancreatitis)
- Drugs known to cause AP include valproate, L-asparaginase, prednisone, 6-mercaptopurine, azathioprine
- Viral infections (enteroviruses, EBV, mumps, CMV, HIV-related)
- Genetic causes: SPINK1, CFTR, PRSS1 mutations - particularly relevant in recurrent and pediatric cases
Chronic Pancreatitis
Alcohol is the leading cause in adults. Repeated acute attacks from any etiology can progress to CP. Genetic mutations, autoimmune pancreatitis, and tropical pancreatitis are other recognized causes.
3. Clinical Presentation
Acute Pancreatitis
- Epigastric pain - severe, constant, boring through to the back; partially relieved by leaning forward
- Nausea and vomiting
- Fever and tachycardia in more severe cases
- Abdominal tenderness - epigastric, may be diffuse in severe disease
- Classic signs in hemorrhagic/necrotizing pancreatitis:
- Grey-Turner sign - flank ecchymosis
- Cullen's sign - periumbilical ecchymosis
- Severe disease: hypotension, tachycardia, respiratory distress, altered mental status (signs of multi-organ failure)
Chronic Pancreatitis
- Recurrent attacks of epigastric pain, often relentless
- Steatorrhoea and malabsorption (exocrine insufficiency)
- Diabetes mellitus (endocrine insufficiency)
- Weight loss and nutritional deficiencies
- Complications: pseudocysts, biliary stricture, fistulae, mesenteric venous thrombosis, arterial pseudoaneurysm, pancreatic ascites
4. Diagnosis
Diagnostic Criteria
Diagnosis requires at least 2 of 3:
- Abdominal pain strongly suggestive of acute pancreatitis
- Serum amylase and/or lipase ≥3 times the upper limit of normal
- Characteristic findings on abdominal imaging
- Clinically, ~40% of acute cases are recognized only at autopsy, underlining the importance of early diagnosis within 48 hours - Textbook of Family Medicine 9e, p. 1136
Laboratory Tests
- Serum lipase - preferred; sensitivity >90%, remains elevated up to 14 days
- Serum amylase - cleared within 48-72 hours; sensitivity falls to <30% by day 2-4
- Neither marker predicts disease severity
- CRP - useful marker for pancreatic necrosis (though limited specificity)
- LFTs, bilirubin, ALP - elevated with biliary obstruction/CBD stone
- BUN, creatinine - rising levels suggest hemoconcentration and third-spacing; fall in BUN with aggressive hydration is a treatment target
- Hematocrit - may be elevated due to fluid shifts (third-spacing)
- Serum triglycerides when metabolic cause is suspected
Imaging
Ultrasound (first-line):
- Recommended in all patients with AP to evaluate for gallstones/biliary cause
- May show diffuse gland swelling, reduced reflectivity, peripancreatic fluid
- Cannot reliably detect pancreatic necrosis
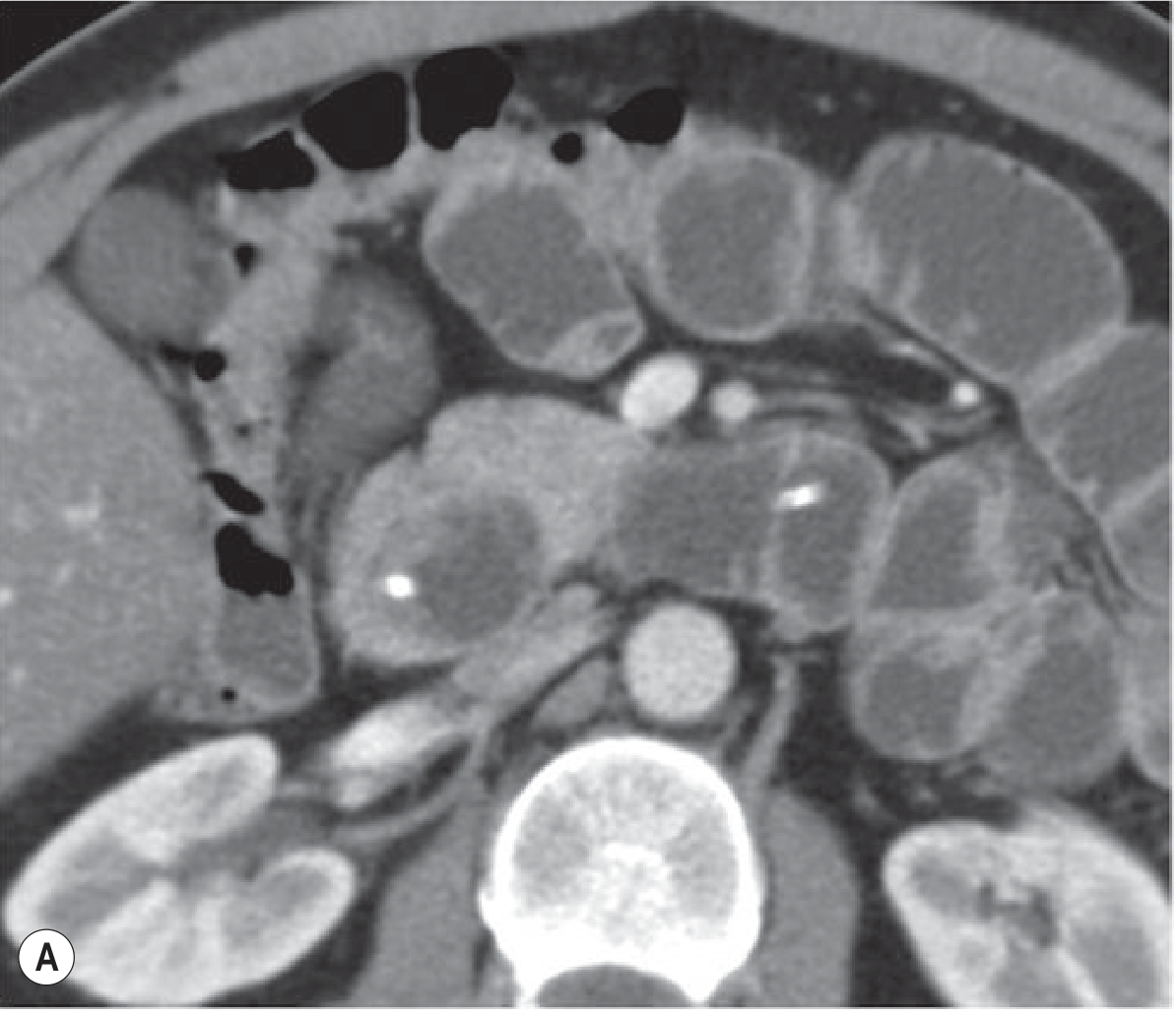
CT (CECT - gold standard for severity):
- Indicated when diagnosis is unclear, or when patient fails to improve in first 48-72 hours
- Best modality to assess presence and extent of pancreatic necrosis, peripancreatic collections
- CT Severity Index (CTSI) / Modified CTSI:
| Prognostic Indicator | Points |
|---|---|
| Normal pancreas | 0 |
| Intrinsic pancreatic abnormalities ± peripancreatic fat changes | 2 |
| Pancreatic/peripancreatic fluid collection or fat necrosis | 4 |
| No pancreatic necrosis | 0 |
| Necrosis ≤30% of parenchyma | 2 |
| Necrosis >30% of parenchyma | 4 |
| Extrapancreatic complications (pleural effusion, ascites, vascular complications, GI involvement) | 2 |
| Mild: 0-2 | Moderate: 4-6 | Severe: 8-10 |
Note: CT scoring does not supersede clinical scoring systems (BISAP, Ranson's, APACHE-II) for identifying severe pancreatitis.
MRCP / MRI - useful for evaluating bile duct stones without the risks of ERCP; preferred when choledocholithiasis is highly suspected but cholangitis/jaundice are absent.
EUS - sensitive for bile duct stones; alternative to MRCP.
Severity Scoring Systems
| System | Variables |
|---|---|
| Ranson's criteria | 11 clinical/lab variables at admission and 48 hours |
| APACHE-II | Physiologic score; calculable at any time |
| BISAP | BUN >25, impaired mental status, SIRS, age >60, pleural effusion |
| Revised Atlanta | Clinical classification into mild/moderately severe/severe |
Overall accuracy for predicting mortality at admission: ~40%, even at 48 hours: ≤80% - Textbook of Family Medicine 9e, p. 1137
5. Management
Acute Pancreatitis - General Principles
Fluid Resuscitation (most critical intervention)
- Aggressive IV hydration with isotonic crystalloid at 250-500 mL/hr in all patients unless cardiovascular or renal comorbidities exist
- Higher rates required in hypotension/tachycardia
- Most beneficial in the first 12-24 hours - may minimize or prevent pancreatic necrosis
- Target: decrease in BUN; correction of hemoconcentration
- Lactated Ringer's preferred over normal saline (anti-inflammatory properties)
Pain Management
- Adequate analgesia is essential (IV opioids commonly used)
Nutrition
A major paradigm shift: from NPO to early enteral nutrition (EN)
- If severe (ICU-level SIRS, mechanical ventilation): nasogastric (NG) or nasojejunal (NJ) tube placed + EN initiated within 24-36 hours
- If mild/moderate (ward-level): oral diet offered as tolerated; EN only if oral diet fails to advance after 4 days
- Gastric vs. jejunal feeding: 3 RCTs showed no significant difference in tolerance or clinical outcomes in severe AP
- EN vs. parenteral nutrition (PN): EN significantly reduces:
- Risk of infected peripancreatic necrosis (OR 0.28, 95% CI 0.15-0.51)
- Single organ failure (OR 0.25, 95% CI 0.10-0.62)
- Multi-organ failure (OR 0.41, 95% CI 0.27-0.63)
- Risk of death (~2.5-fold reduction)
- Source: AGA technical review of 12 RCTs - Sleisenger & Fordtran's GI and Liver Disease, p. (nutrition chapter)
Antibiotics
- Not indicated routinely
- Indicated only for documented infection (e.g., infected pancreatic necrosis, cholangitis)
- Prophylactic antibiotics do not reduce mortality or infection rates in AP
Gallstone Pancreatitis
- ERCP within 24 hours if concurrent acute cholangitis
- ERCP not needed in most patients without evidence of ongoing biliary obstruction
- Without cholangitis/jaundice: use MRCP or EUS to screen for choledocholithiasis first
- Early laparoscopic cholecystectomy (within 3 days) in mild biliary pancreatitis improves outcomes and reduces need for subsequent ERCP
- Standard of care: early cholecystectomy after resolution
Local Complications
| Complication | Definition | Timing | Management |
|---|---|---|---|
| Acute peripancreatic fluid collection | Fluid near pancreas, no wall | Early (< 4 weeks) | Usually resolves spontaneously |
| Pseudocyst | Fluid collection with capsule, no significant solid debris | >4 weeks after AP | Endoscopic drainage if symptomatic/infected, close to GI wall |
| Acute necrotic collection | Mixed solid/liquid necrotic material, no wall | Early | Often conservative; drain if infected |
| Walled-off necrosis (WON) | Encapsulated necrosis | >4 weeks after AP | Endoscopic transmural drainage if symptomatic/infected |
- Endoscopic drainage preferred for collections in close apposition to the gastric or duodenal wall (endoscopic cyst-gastrostomy or cyst-duodenostomy)
6. Chronic Pancreatitis Management
- Abstinence from alcohol (patients who continue drinking have more recurrent attacks)
- Pain management - often requires multimodal approach; selected patients may benefit from therapeutic ERCP or pancreatic surgery
- Pancreatic enzyme supplementation with each meal for exocrine insufficiency (malabsorption, steatorrhoea)
- Diabetes management - pancreatic (type 3c) diabetes requiring insulin
- Nutritional support - jejunal feeding used to improve weight and reduce pain; antioxidant supplementation (selenium, ascorbic acid, β-carotene, α-tocopherol, methionine) has shown benefit in some RCTs for pain relief
- ERCP for ductal strictures and stones; endoscopic pancreatic sphincterotomy
- Surgery: lateral pancreaticojejunostomy (Partington-Rochelle) or Whipple procedure for selected cases
Complications of CP requiring monitoring and intervention:
- Pseudocyst, abscess
- Bile duct stricture
- Fistula (pancreatic-enteric, pancreaticoplural)
- Pancreatic ascites
- Mesenteric venous thrombosis
- Arterial pseudoaneurysm
- Increased risk of pancreatic adenocarcinoma
7. Prognosis
- Mild AP: >80% recover uneventfully; most cases resolve within 1 week
- Severe AP: mortality ~29.5% (mainly from respiratory or hemodynamic failure, or infected necrosis)
- ~40% of severe acute cases only recognized at autopsy, underscoring need for early clinical vigilance
- CP is progressive; eventual exocrine failure (malabsorption) and endocrine failure (diabetes) are common end points
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Textbook of Family Medicine 9e; Grainger & Allison's Diagnostic Radiology; Clinical Gastrointestinal Endoscopy 3e
This is a shared conversation. Sign in to Orris to start your own chat.