Contractility of cardiac muscle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to deliver a thorough answer. Let me compile everything.
Contractility of Cardiac Muscle
Definition
Contractility (also called inotropy) is the intrinsic ability of cardiac muscle to generate force and shorten, independent of preload (fiber length) and afterload (resistance to ejection). It is a measure of the "vigor" of contraction that allows comparison between a well-performing and a poorly performing heart at the same filling volume and arterial pressure.
- Medical Physiology, p. 773: "Contractility is a somewhat vague but clinically useful term that distinguishes a better-performing heart from a poorly performing one."
Molecular Basis of Contraction
The fundamental contractile event depends on activator calcium (Ca²+) binding to the actin-troponin-tropomyosin complex, which uncovers myosin-binding sites on actin and permits cross-bridge cycling.
The diagram below (from Katzung's Basic & Clinical Pharmacology) shows the full calcium handling pathway in a cardiac sarcomere:
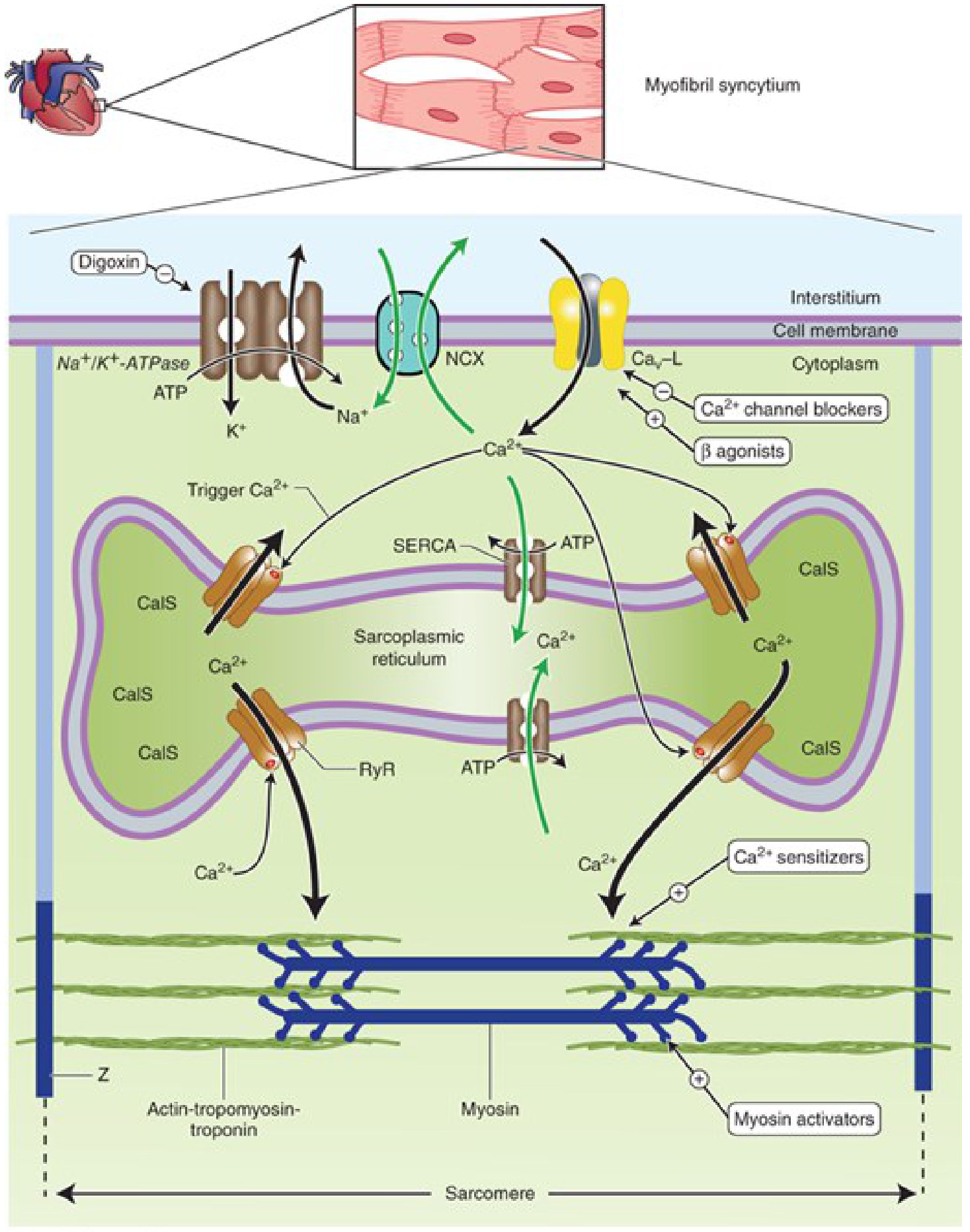
Key components:
- L-type Ca²+ channels (Ca_v-L): Voltage-gated; open during action potential plateau, admitting trigger Ca²+
- Ryanodine receptors (RyR2): Ca²+-sensitive SR channels; trigger Ca²+ from the L-type channel causes them to release a large Ca²+ bolus (Ca²+-induced Ca²+ release, CICR)
- SERCA (Sarcoplasmic Endoplasmic Reticulum Ca²+-ATPase): Pumps Ca²+ back into the SR during relaxation; normally inhibited by phospholamban
- NCX (Na-Ca exchanger): Antiporter using the Na+ gradient to extrude Ca²+ from the cell (3 Na+ in : 1 Ca²+ out)
- Na+/K+-ATPase: Maintains the Na+ gradient that drives NCX; the target of cardiac glycosides (digoxin)
- Calsequestrin (CalS): High-capacity Ca²+ storage protein within the SR
Determinants of Contractility (Katzung, 16th Edition, p. 332)
Contractility is regulated at six main points:
1. Calcium Sensitivity of Contractile Proteins
The relationship between myofibril shortening and cytoplasmic [Ca²+] is the "calcium sensitivity curve." Drugs like levosimendan increase this sensitivity (and may inhibit phosphodiesterase), improving contraction without raising [Ca²+]. Omecamtiv mecarbil shifts myosin from a low-actin-binding state to a strongly force-generating state, potentially improving efficiency.
2. Ca²+ Released from SR
Trigger Ca²+ (entering via L-type channels) opens RyR2 channels in the SR membrane, releasing a large Ca²+ bolus. The amount released is proportional to both the SR Ca²+ load and the trigger signal.
3. Ca²+ Stored in the SR
SERCA fills the SR during diastole. Phosphorylation of phospholamban by PKA (via cAMP, stimulated by beta-adrenergic activation) de-inhibits SERCA, increasing SR Ca²+ loading and thus the available pool for release. The SR Ca²+ store is also governed by the balance of Ca²+ influx (L-type channels) vs. Ca²+ efflux (NCX).
4. Amount of Trigger Ca²+
This depends on extracellular [Ca²+], channel availability, and duration of opening. Sympathomimetics increase Ca²+ influx through these channels; calcium channel blockers reduce it.
5. Na-Ca Exchanger (NCX) Activity
NCX exchanges 3 Na+ (in) for 1 Ca²+ (out). Its direction is governed by intracellular [Na+]. If intracellular Na+ rises (e.g., Na+/K+-ATPase is inhibited by digoxin), NCX is slowed, Ca²+ builds up inside the cell, and contractility increases.
6. Intracellular Na+ / Na+/K+-ATPase
Na+/K+-ATPase is the primary regulator of intracellular [Na+]. This is the key mechanism of cardiac glycosides: digoxin inhibits Na+/K+-ATPase -> [Na+]_i rises -> NCX slowed -> [Ca²+]_i rises -> positive inotropy.
Positive vs. Negative Inotropic Agents
| Agent | Mechanism |
|---|---|
| Catecholamines (epi, norepinephrine) | beta-1 receptor -> Gs -> cAMP -> PKA -> opens L-type Ca²+ channels; phosphorylates phospholamban (also speeds relaxation) |
| Cardiac glycosides (digoxin) | Inhibit Na+/K+-ATPase -> [Na+]_i up -> NCX slowed -> [Ca²+]_i up |
| High extracellular [Ca²+] | Reduces NCX-driven Ca²+ efflux; more Ca²+ entry via L-type channels |
| Low extracellular [Na+] | Reduces Na+ gradient -> NCX slowed -> [Ca²+]_i up |
| Increased heart rate | Staircase (Bowditch) phenomenon: more Ca²+ enters per unit time, SR loads up |
| Ca²+ channel blockers (verapamil, diltiazem) | Reduce L-type Ca²+ influx -> less trigger -> negative inotropic effect |
Measuring Contractility
Because contractility must be independent of load, simple measures like stroke volume or cardiac output are insufficient (they depend on preload). Better indices include:
| Index | Basis |
|---|---|
| Ejection fraction (EF) | Widely used clinically; still somewhat load-dependent |
| dP/dt_max | Maximum rate of LV pressure rise during isovolumic contraction; sensitive to inotropic interventions |
| ESPVR (End-Systolic Pressure-Volume Relation) | Slope (E_es) is load-independent; gold standard for contractility measurement |
| Preload recruitable stroke work (Msw) | Slope of stroke work vs. end-diastolic volume relation |
The diagram below shows how beta-adrenergic stimulation increases the slope of the ESPVR (E_es), reflecting positive inotropy, while also causing a positive lusitropic (relaxation) effect:
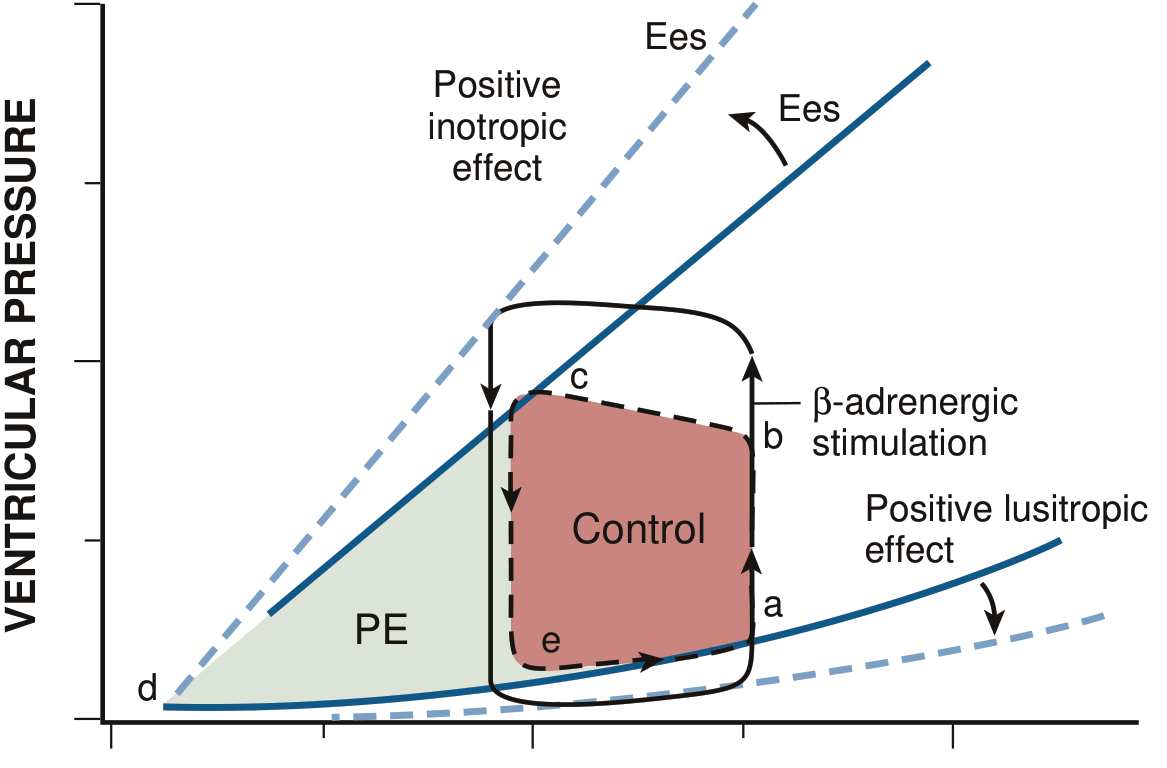
A steeper ESPVR slope = higher contractility. Dobutamine or catecholamines shift the line upward and to the left; myocardial depression (e.g., heart failure) flattens it.
Contractility vs. Preload (Frank-Starling Mechanism)
These two are often confused but represent distinct phenomena:
- Preload effect (Frank-Starling): Increased EDV stretches sarcomeres -> improved actin-myosin overlap and increased Ca²+ sensitivity -> stronger contraction. This is a length-dependent change in performance - the heart does not "have more contractility," it uses existing contractility more effectively.
- Contractility change: A change in force generation at any given fiber length - i.e., the entire Frank-Starling curve shifts upward (positive inotropy) or downward (negative inotropy).
Clinically: a positive inotropic intervention shifts the entire Starling curve upward; the same EDV now produces a greater stroke volume.
Clinical Relevance
- Heart failure with reduced EF (HFrEF): Contractility is depressed; E_es is low and the ESPVR is shallow. Inotropic agents (dobutamine, milrinone) temporarily increase contractility.
- Calcium channel blockers: Reduce contractility by limiting trigger Ca²+ - important to remember in patients with borderline cardiac function.
- Digoxin toxicity: Results from excessive intracellular Ca²+ accumulation - can cause dangerous ventricular arrhythmias.
- Beta-blockers: Initially reduce contractility but in chronic heart failure, they up-regulate beta receptors and ultimately improve contractile function over time.
Sources: Medical Physiology (Boron & Boulpaep), p. 773-774; Katzung's Basic & Clinical Pharmacology, 16th Edition, p. 332-334; Braunwald's Heart Disease; Barash's Clinical Anesthesia, 9th Edition, p. 900-901
This is a shared conversation. Sign in to Orris to start your own chat.