Explain me about tracts of cns
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have comprehensive information from Gray's Anatomy for Students and Guyton & Hall. Here is the full explanation:
Tracts of the CNS
CNS tracts are organized bundles of myelinated axons (white matter) that carry signals between the spinal cord, brainstem, and brain. They divide into two broad categories: ascending (sensory) tracts going up toward the brain, and descending (motor) tracts going down toward the muscles.
The diagram below shows all major tracts in a cross-section of the spinal cord:
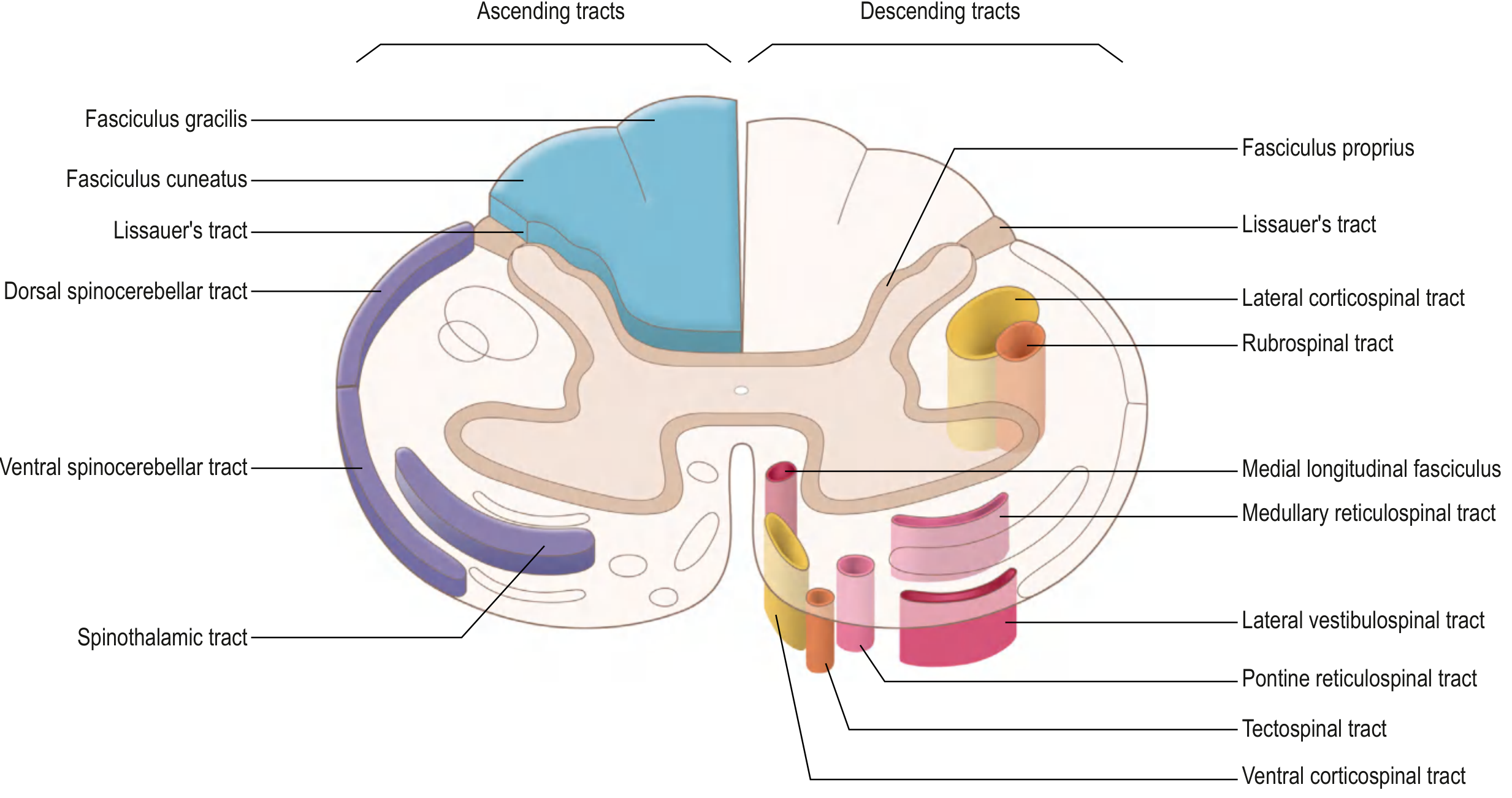
ASCENDING (SENSORY) TRACTS
Sensory information from peripheral receptors is carried upward through a chain of three neurons before reaching the cortex.
1. Anterolateral Pathways
These carry pain, temperature, and crude touch. They consist of three tracts:
A. Spinothalamic Tract (most important)
- 1st-order neuron: Cell body in the dorsal root ganglion. Enters the spinal cord via the posterior root, and either synapses immediately in the posterior horn (laminae I & V) or ascends 1-2 segments in Lissauer's tract before synapsing.
- 2nd-order neuron: Crosses obliquely over 2-3 spinal segments via the anterior commissure to the opposite (contralateral) anterolateral tract, then ascends to the ventral posterior lateral (VPL) nucleus of the thalamus.
- 3rd-order neuron: Projects through the posterior limb of the internal capsule to reach the primary somatosensory cortex.
Key point: Decussation happens at the level of entry (in the spinal cord), so a lesion above the decussation produces contralateral sensory loss.
B. Spinoreticular Tract
- Same first-order neuron as spinothalamic, but the 2nd-order axons project to the reticular formation of the brainstem.
- Conveys the emotional and arousal aspects of pain (the suffering component).
C. Spinomesencephalic Tract
- 2nd-order axons project to the periaqueductal gray (PAG) of the midbrain.
- Involved in pain modulation (activates descending inhibitory pain pathways).
2. Posterior Column - Medial Lemniscal Pathway
Carries fine/discriminative touch, vibration, and conscious proprioception.
- 1st-order neuron: Cell body in the dorsal root ganglion. Axons enter the posterior root and ascend ipsilaterally in the posterior (dorsal) columns:
- Fasciculus gracilis (medial) - from lower limbs and trunk (below T6)
- Fasciculus cuneatus (lateral) - from upper limbs and neck (above T6)
- They ascend all the way to the caudal medulla where they synapse in:
- Nucleus gracilis (for gracilis fibers)
- Nucleus cuneatus (for cuneatus fibers)
- 2nd-order neuron: Axons cross as internal arcuate fibers to form the medial lemniscus on the contralateral side, then ascend to the VPL nucleus of the thalamus.
- 3rd-order neuron: Projects through the posterior limb of the internal capsule to the primary somatosensory cortex.
Key difference from spinothalamic: Decussation happens in the medulla (not in the spinal cord). So a spinal cord lesion affecting the posterior columns causes ipsilateral loss of fine touch and proprioception.
DESCENDING (MOTOR) TRACTS
Descending tracts control voluntary movement, posture, and balance. They involve upper motor neurons (UMN) (cortex or brainstem) and lower motor neurons (LMN) (anterior horn of spinal cord).
They divide into the Lateral and Medial motor systems.
LATERAL MOTOR SYSTEM
Controls distal limb muscles - voluntary, skilled movements.
1. Lateral Corticospinal Tract (most important motor tract)
- Origin: ~30% primary motor cortex, ~30% premotor/supplementary motor cortex, ~40% somatosensory cortex (posterior to central sulcus).
- Course: Axons converge in the corona radiata → posterior limb of the internal capsule → crus cerebri of the midbrain → anterior pons (scattered bundles) → form the pyramids of the medulla.
- Decussation: At the caudal medulla (pyramidal decussation / cervicomedullary junction), ~85-90% of fibers cross to the contralateral side, forming the lateral corticospinal tract in the lateral funiculus.
- Termination: Synapse on LMN cell bodies in the lateral anterior horn at all spinal cord levels (especially cervical and lumbosacral enlargements for limb control).
- Special fibers: Giant Betz cells in the primary motor cortex send the fastest-conducting fibers (~70 m/sec). There are ~34,000 large Betz cell fibers per tract, but over 1 million fibers total.
- Function: Movement of contralateral limbs.
2. Rubrospinal Tract
- Origin: Red nucleus (magnocellular division), midbrain.
- Decussation: Crosses immediately in the ventral tegmental decussation of the midbrain.
- Termination: Cervical spinal cord only; synapses on interneurons in the anterior horn.
- Function: Facilitates flexor muscle activity and inhibits extensor activity of the upper limb. In humans, its functional role is uncertain (possibly overshadowed by the corticospinal tract).
MEDIAL MOTOR SYSTEM
Controls axial and proximal muscles - posture, balance, gait, and head/neck orientation. These tracts project bilaterally, making individual clinical testing difficult.
1. Anterior Corticospinal Tract
- Formed by fibers (~10-15%) that did NOT decussate in the medulla.
- Descend ipsilaterally in the anterior funiculus to cervical and upper thoracic levels.
- Project bilaterally to LMNs in the medial anterior horn.
- Function: Control of bilateral axial and girdle muscles.
2. Tectospinal Tract
- Origin: Superior colliculus (dorsal midbrain), which receives visual input.
- Decussation: Dorsal tegmental decussation, immediately after origin.
- Descends near the medial longitudinal fasciculus (MLF) into cervical spinal cord.
- Function: Reflex postural movements of the head and neck in response to visual stimuli.
3. Vestibulospinal Tracts (VST) - Two tracts
| Tract | Origin | Course | Function |
|---|---|---|---|
| Medial VST | Medial & inferior vestibular nuclei | Bilaterally to cervical/upper thoracic | Head and neck positioning |
| Lateral VST | Lateral (Deiters') vestibular nucleus | Ipsilaterally down entire cord | Facilitates extensor/antigravity muscles, inhibits flexors - maintains balance and upright posture |
The vestibular nuclei receive input from the inner ear and cerebellum. The classic example: when you start to trip, the lateral VST fires to extend the limbs and prevent the fall.
4. Reticulospinal Tracts (Pontine & Medullary)
- Origin: Reticular formation in pons and medulla.
- Both tracts descend ipsilaterally in the anterior white matter to all levels.
- Function: Regulate voluntary movements, reflex activity, and autonomic outflow.
Summary Table: Key Tracts at a Glance
| Tract | Type | Modality / Function | Decussation Level | Key Location in Cord |
|---|---|---|---|---|
| Spinothalamic | Ascending | Pain, temperature, crude touch | Spinal cord (entry level) | Anterolateral |
| Posterior column (gracilis + cuneatus) | Ascending | Fine touch, vibration, proprioception | Medulla | Posterior funiculus |
| Spinoreticular | Ascending | Emotional/arousal aspect of pain | - | Anterolateral |
| Lateral corticospinal | Descending | Voluntary limb movement | Caudal medulla (pyramidal decussation) | Lateral funiculus |
| Anterior corticospinal | Descending | Bilateral axial/postural control | Spinal cord level | Anterior funiculus |
| Rubrospinal | Descending | Flexor tone, upper limb | Midbrain (ventral tegmental) | Lateral funiculus |
| Vestibulospinal | Descending | Balance, extensor tone | None (ipsilateral) | Anterior funiculus |
| Reticulospinal | Descending | Posture, gait, autonomic | None (ipsilateral) | Anterior funiculus |
| Tectospinal | Descending | Head/eye reflex movement | Midbrain (dorsal tegmental) | Anterior funiculus (cervical) |
Clinical Relevance
- Hemisection of the spinal cord (Brown-Sequard Syndrome): Ipsilateral loss of fine touch/proprioception (posterior columns) + contralateral loss of pain/temperature (spinothalamic), both below the lesion. Motor loss is ipsilateral (lateral corticospinal).
- UMN vs LMN lesions: Damage to the lateral corticospinal tract above the anterior horn causes UMN signs (spasticity, hyperreflexia, Babinski sign). Damage at or below the anterior horn (LMN) causes flaccid paralysis, atrophy, hyporeflexia.
- Syringomyelia: Cavity in the central cord damages crossing spinothalamic fibers (anterior commissure) → bilateral loss of pain and temperature at the affected dermatome level ("cape" distribution), with preserved posterior columns.
Sources: - Gray's Anatomy for Students, pp. 1326-1335 | - Guyton and Hall Textbook of Medical Physiology, p. 689
This is a shared conversation. Sign in to Orris to start your own chat.