Female at perimenopausal age with bleeding more than 7 days and anemic
Reading File
Finding Sources
Finding Sources
Searching PubMed
"abnormal uterine bleeding" AND perimenopause AND management
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is the full clinical response:
Perimenopausal Female: Bleeding >7 Days with Anemia
Definition & Classification
This presentation is Abnormal Uterine Bleeding (AUB) - specifically Heavy Menstrual Bleeding (HMB) with prolonged duration. Per FIGO terminology, flow lasting >8 days on a regular basis is classified as prolonged menstrual bleeding; >7 days is already beyond the upper normal limit of a menstrual cycle. The FIGO PALM-COEIN classification (2011) replaced the obsolete term "dysfunctional uterine bleeding."
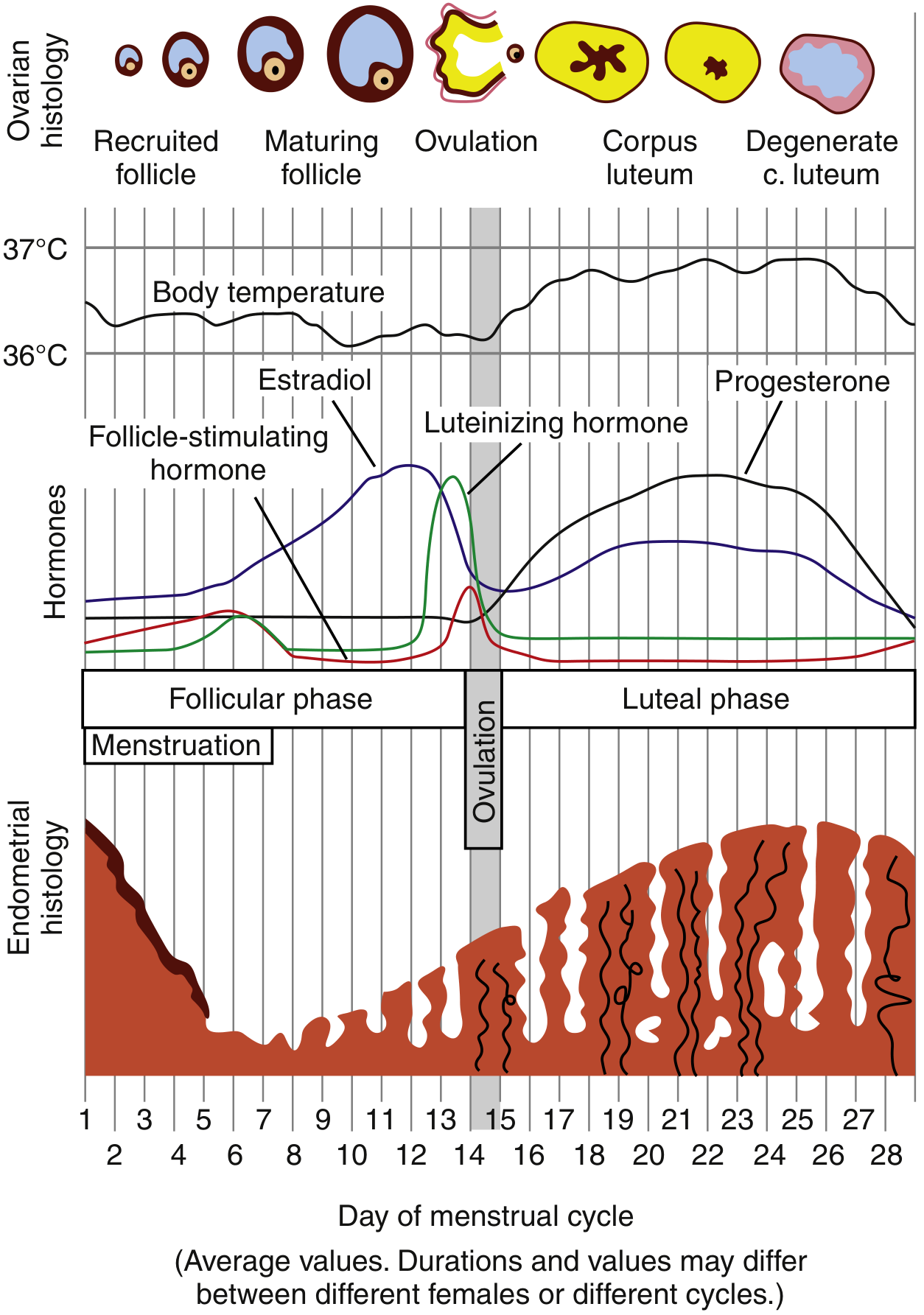
In perimenopause, declining ovarian function disrupts the HPO axis shown above - the result is anovulatory cycles with unopposed estrogen.
PALM-COEIN: Causes to Consider
PALM (Structural)
| Cause | Notes in Perimenopause |
|---|---|
| Polyp (AUB-P) | Endometrial/endocervical polyps; common in women >35; cause intermenstrual bleeding |
| Adenomyosis (AUB-A) | Endometrial glands within myometrium; heavy, painful periods |
| Leiomyoma (AUB-L) | Submucosal fibroids most likely to cause heavy bleeding; palpable on bimanual exam |
| Malignancy/Hyperplasia (AUB-M) | Must rule out in this age group - endometrial hyperplasia and carcinoma risk rises sharply >40 |
COEIN (Non-structural)
| Cause | Notes |
|---|---|
| Ovulatory Dysfunction (AUB-O) | Most common cause in perimenopause - anovulatory cycles from HPO axis dysregulation; unopposed estrogen leads to irregular, heavy, prolonged bleeding |
| Endometrial (AUB-E) | Abnormal endometrial hemostasis; primary disorder of the endometrium |
| Coagulopathy (AUB-C) | Von Willebrand disease (up to 13% of HMB); acquired coagulopathies (liver disease, anticoagulants) |
| Iatrogenic (AUB-I) | Exogenous hormone use, IUD, anticoagulants |
| Not classified (AUB-N) | Rare entities |
In patients >40 years but not yet postmenopausal, anovulatory bleeding due to perimenopause is most likely, but endometrial carcinoma or hyperplasia and leiomyoma must be actively excluded - Rosen's Emergency Medicine
Why Anovulation Drives Perimenopausal AUB
Perimenopause is characterized by declining and erratic ovarian follicular function. When ovulation fails:
- No corpus luteum forms → no progesterone secretion
- Estrogen continues to stimulate endometrial proliferation unopposed
- The thickened endometrium sheds irregularly, erratically, and heavily
- Prolonged amenorrhea followed by heavy bleeding is the classic pattern
- Chronically increases risk of endometrial hyperplasia and adenocarcinoma
Evaluation
Initial Assessment (for any patient)
- Hemodynamic stability first - examine for signs of hypovolemia/anemia (pallor, tachycardia, BP)
- Rule out pregnancy (urine/serum β-hCG) - always, even in perimenopause
Laboratory Workup
| Test | Rationale |
|---|---|
| CBC | Confirm anemia, platelet count |
| Serum β-hCG | Exclude pregnancy |
| PT/aPTT | Coagulopathy screen |
| TSH | Hypothyroidism causes AUB in 0.3-2.5% of cases |
| Iron studies (ferritin, serum iron, TIBC) | Characterize iron deficiency anemia |
| FSH/LH/Estradiol | Confirm perimenopausal status |
| Consider: vWF antigen/activity | If history of lifelong heavy periods |
Imaging
- Transvaginal ultrasound (TVUS): first-line imaging
- Identifies fibroids, polyps, endometrial thickening, ovarian pathology
- Endometrial thickness >4-5 mm in postmenopausal women warrants further evaluation; in perimenopausal women, thickness is more variable but >12 mm is abnormal
- Sonohysterography (saline infusion sonography): better delineation of intracavitary lesions
Endometrial Sampling - Mandatory in This Age Group
- Endometrial biopsy (EMB) is indicated in all perimenopausal women with AUB to exclude endometrial hyperplasia and carcinoma
- Indicated especially with: age >40, obesity, diabetes, hypertension, nulliparity, family history of endometrial/colorectal cancer
- Hysteroscopy with D&C if EMB is inconclusive or inadequate
Management
Acute/Emergency Management (Hemodynamically Unstable or Severe Anemia)
| Drug | Dose | Notes |
|---|---|---|
| Conjugated equine estrogen (IV Premarin) | 25 mg IV every 4-6 hours until bleeding stops (max 24 h) | Emergency use; stops bleeding within hours; contraindicated in VTE, thrombophilia, liver disease, malignancy |
| Tranexamic acid (TXA) | 1.0-1.3 g IV (can continue PO 3x/day) | FDA-approved for menorrhagia; prevents clot degradation; especially effective in fibroids; reduces blood loss significantly |
| Intrauterine tamponade | 26-Fr Foley with 30 mL saline | Temporizing measure |
| Surgical: D&C, uterine artery embolization, endometrial ablation, hysterectomy | As indicated | If medical management fails |
Medical Management (Subacute/Chronic)
Hormonal Options:
| Drug | Dose | Notes |
|---|---|---|
| Combined OCP (monophasic) | 1 pill TID x7 days OR 1 pill BID x5 days then QD for rest of pack | Regulates cycles; reduces flow; avoid in smokers >35 yo, VTE history, uncontrolled HTN, active liver disease |
| Progestin-only (MPA) | Medroxyprogesterone acetate 10 mg PO OD x10 days | For women with estrogen contraindications; preferred in perimenopause |
| Levonorgestrel IUD (Mirena) | Long-term | Highly effective; reduces flow by 90%; first-line for long-term management |
| Cyclic progestins | Days 14-28 of cycle | Controls anovulatory bleeding; not contraceptive |
| GnRH agonists | (leuprolide, etc.) | Short-term only; for fibroid-related HMB pre-surgery |
Non-Hormonal Options:
| Drug | Dose | Notes |
|---|---|---|
| NSAIDs (ibuprofen/mefenamic acid) | PO with meals | Reduces flow 30-50%; useful for ovulatory HMB; less effective than TXA or LNG-IUD |
| Tranexamic acid (PO) | 1.3 g TID during menses | Antifibrinolytic; FDA-approved; does not affect cycle regularity |
| Danazol | 200 mg/day | Reduces flow significantly; androgenic side effects limit use |
Treatment of Associated Iron Deficiency Anemia
- Oral ferrous sulfate 325 mg TID (on empty stomach if tolerated) - first-line
- IV iron sucrose or ferric carboxymaltose if oral iron not tolerated, non-compliant, or severe anemia requiring faster repletion
- Blood transfusion if Hb <7 g/dL or hemodynamically unstable
Surgical Management
Reserved for failure of or contraindications to medical therapy:
- Endometrial ablation: effective for AUB without structural lesions; not suitable if malignancy suspected
- Hysteroscopic myomectomy/polypectomy: for submucosal fibroids or polyps
- Hysterectomy: definitive treatment
Red Flags Requiring Urgent Evaluation
- Hemodynamic instability
- Hb <8 g/dL with ongoing bleeding
- Endometrial thickness >12 mm on TVUS
- Irregular or thickened endometrium
- Postcoital bleeding (suggests cervical/endometrial pathology)
- Associated pelvic pain/mass
- Risk factors for endometrial cancer (obesity, DM, PCOS, nulliparity)
"Perimenopausal and menopausal women with abnormal bleeding should have expedited follow-up for evaluation of possible malignancy." - Rosen's Emergency Medicine
Key Summary
Perimenopausal AUB + Anemia
↓
1. Stabilize (fluids, transfusion if needed)
2. Rule out pregnancy
3. CBC, TSH, coags, iron studies
4. TVUS → assess endometrial thickness, structural pathology
5. Endometrial biopsy → exclude hyperplasia/cancer
6. Treat bleeding: TXA ± hormonal therapy (MPA or OCP taper)
7. Treat anemia: oral/IV iron ± transfusion
8. Long-term: LNG-IUD or cyclic progestins
9. If structural cause found → targeted surgical/procedural management
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 86 (Abnormal Uterine Bleeding)
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, Chapter 96 (Vaginal Bleeding)
She doesn't have any structural cause so what should be the management
Finding Sources
Finding Sources
Searching PubMed
"anovulatory bleeding" AND perimenopause AND treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Excellent - now I have comprehensive, specific management data. Here is the focused answer:
Management of AUB-O (Anovulatory) in a Perimenopausal Woman with Anemia
No structural cause confirmed + perimenopausal age = AUB-O - anovulatory bleeding from unopposed estrogen due to declining HPO axis function. The endometrium proliferates without progesterone to stabilize it, then sheds irregularly and heavily.
Step 1: Assess Severity
| Severity | Definition | Initial Action |
|---|---|---|
| Hemodynamically unstable | Shock, active heavy bleeding | Resuscitate first (IV fluids, pRBC transfusion) |
| Stable with severe anemia | Hb <8, ongoing bleeding | Medical hemostasis + transfusion if Hb <7 |
| Stable, moderate-severe anemia | Hb 8-10, prolonged bleeding | Medical management + oral iron |
Step 2: Stop the Acute Bleed
A. Hormonal - First Line
Option 1: Combined OCP (if no estrogen contraindications)
- Monophasic pill containing <35 µg ethinyl estradiol
- 1 pill every 6 hours x 5-7 days (acute heavy bleed) - Goldman-Cecil Medicine
- OR: 1 pill TID x 7 days; or 1 pill BID x 5 days then OD for rest of pack
- Bleeding should cease within 24-72 hours
- ⚠️ Warn the patient: heavy withdrawal bleed expected 2-4 days after stopping
- After acute control: transition to cyclic OCP (1 pill/day) for at least 3 cycles
Contraindications to estrogen (very relevant in perimenopausal women): smokers >35 years, hypertension, VTE/stroke history, active liver disease, thromboembolic disorders, breast cancer, uncontrolled diabetes with vascular disease
Option 2: Progestin-only (if estrogen is contraindicated - preferred for perimenopausal/older patients)
- Medroxyprogesterone acetate (MPA):
- Acute: 20 mg PO TID x 7 days, OR 10 mg OD x 10 days
- Bleeding stops in >3 days typically
- Simultaneously with IV estrogen in severe cases
- After acute episode: cyclic MPA (days 14-28 of cycle) for long-term management
B. Non-Hormonal Adjunct
Tranexamic acid (antifibrinolytic)
- Acute IV: 1.0-1.3 g IV, effective within ~3 hours; can continue PO TID
- Ongoing: 1.3 g PO TID during days of heavy bleeding only
- FDA-approved for menorrhagia
- Reduces menstrual blood loss significantly; does not affect cycle regularity
- ⚠️ Contraindicated in VTE/thrombophilia history
NSAIDs
- Naproxen 500 mg BID, OR Ibuprofen 400 mg every 6 hours, OR Mefenamic acid 500 mg TID
- Reduce blood loss 30-50% by inhibiting prostaglandins
- Use during days of heavy flow; less potent than TXA or LNG-IUD
- Caution: GI disease, renal disease, bleeding disorders
Step 3: Long-Term Maintenance (Prevent Recurrence)
Once acute bleed is controlled, a long-term strategy is needed because perimenopausal anovulatory cycles will continue until menopause:
| Option | Dosing | Best For |
|---|---|---|
| Levonorgestrel IUD (Mirena) | Inserted once; lasts 5 years | First-line long-term - reduces flow by ~90%, provides endometrial protection, local progestin with minimal systemic effects |
| Cyclic oral contraceptives | 1 pill/day cyclically | Cycle regulation + contraception (perimenopausal women can still ovulate unpredictably) |
| Cyclic progestins | MPA 10 mg OD, days 14-28 | When estrogen contraindicated; induces regular withdrawal bleeds; protects endometrium from hyperplasia |
| Continuous progestin | Norethindrone 5 mg OD or MPA 10 mg OD continuously | Induces amenorrhea; good for reducing blood loss |
| NSAIDs + TXA | Each cycle during menses | Non-hormonal option; additive effect when combined |
Step 4: Treat Iron Deficiency Anemia
Since bleeding has been prolonged, iron depletion is almost certain:
| Route | Drug | Dose | Notes |
|---|---|---|---|
| Oral (first-line) | Ferrous sulfate / fumarate / gluconate | 325 mg TID | Avoid timed-release preparations (bypass duodenum, ineffective); take on empty stomach for best absorption; Hb rises ~0.9 g/dL/week |
| IV (second-line) | Ferric carboxymaltose or Iron sucrose | Per weight-based formula | For severe anemia needing faster repletion, intolerance to oral iron, or ongoing blood loss exceeding oral supplementation capacity; Hb rises ~1.5-1.9 g/dL/week |
| Transfusion | pRBC | If Hb <7 g/dL or hemodynamic instability | Acute setting only |
Summary Algorithm
Perimenopausal AUB-O (no structural cause) + Anemia
↓
Hemodynamically stable?
YES ──────────────────→ NO → Resuscitate + IV estrogen + IV TXA
↓
Estrogen contraindicated?
NO → Combined OCP taper (TID x7 days)
YES → MPA 20 mg TID x7 days (or 10 mg OD x10 days)
↓
Bleeding controlled → Withdrawal bleed expected (warn patient)
↓
Long-term:
- LNG-IUD (first preference) OR cyclic progestins/OCP
- TXA ± NSAIDs each cycle if non-hormonal preferred
↓
Treat anemia:
- Oral ferrous sulfate TID (ongoing)
- IV iron if severe or oral not tolerated
↓
Follow-up: Repeat CBC at 4-6 weeks; gynecology review
"Anovulatory bleeding in the reproductive-age female increases the risk of endometrial hyperplasia and adenocarcinoma" - even after structural causes are excluded, cyclic progestin or LNG-IUD is mandatory to protect the endometrium from ongoing unopposed estrogen. - Tintinalli's Emergency Medicine
Sources:
- Goldman-Cecil Medicine, Chapter 220 (Abnormal Uterine Bleeding - Treatment)
- Tintinalli's Emergency Medicine, Chapter 96 (Table 96-4: Treatment of Heavy Vaginal Bleeding)
- Rosen's Emergency Medicine, Chapter 30 & 86 (Pharmacologic Treatment Regimens for AUB)
- Berek & Novak's Gynecology, Nonsurgical Management of AUB
This is a shared conversation. Sign in to Orris to start your own chat.