Embryology and development of larynx in a creative manner from standard ENT textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have all the key content needed. Let me compose a rich, creative, well-illustrated response.
🎭 The Story of the Larynx: An Embryological Drama in Four Acts
Sources: The Developing Human (Moore & Persaud), Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology
Prologue: Setting the Stage (Week 4 - The Pharyngeal Apparatus)
Picture the 4-week embryo's foregut as a bustling construction site. Six paired pharyngeal (branchial) arches - ridges of mesoderm clad in ectoderm outside and endoderm inside - stack up on either side of the developing head and neck. Each arch carries its own cartilage blueprint, muscle crew, nerve foreman, and vascular supply. The larynx will be built primarily by workers from Arch 4 and Arch 6 - the last two active arches, the unsung heroes of voice.
On the floor of the primitive pharynx, a small groove appears pointing downward: the laryngotracheal groove. This is the first whisper that a voice box is coming.
Act I: The Groove Becomes a Bud (Week 4-5)
The laryngotracheal groove deepens into the laryngotracheal diverticulum - a fingerlike outpouching from the ventral wall of the foregut (future pharynx). As it elongates caudally, it pinches off from the esophagus behind it, separated by two ridges - the tracheoesophageal folds - that fuse in the midline to form the tracheoesophageal septum.
Think of it as two zipper pulls meeting in the middle: if the zipper fails to close completely, you get a tracheoesophageal fistula (TEF) - the most common congenital anomaly of this region.
The cranial end of this diverticulum becomes the primordium of the larynx. Its lining is endoderm - the same tissue that will coat every surface inside.
Act II: The Architects Arrive - Arch 4 and Arch 6 Cartilages
Here is where the drama gets specific. Neural crest cells migrate into Arches 4 and 6 and condense as mesenchyme around the cranial end of the laryngotracheal tube. They differentiate into the laryngeal cartilages with a precise division of labour:
| Pharyngeal Arch | Cartilage Derivatives | Muscle Crew | Nerve Foreman |
|---|---|---|---|
| Arch 4 | Thyroid cartilage, cuneiform cartilages, epiglottis | Cricothyroid, pharyngeal constrictors | Superior laryngeal nerve (CN X) |
| Arch 6 | Cricoid, arytenoid, corniculate cartilages | All intrinsic laryngeal muscles (except cricothyroid) | Recurrent laryngeal nerve (CN X) |
Why does the recurrent laryngeal nerve loop under the aortic arch? Because the 6th arch artery becomes the ductus arteriosus (left) and proximal pulmonary artery (right). As the heart descends into the thorax, the nerve - loyal to its arch - gets dragged down with it, forced to loop around the 6th arch artery remnant. A perfect example of embryology dictating adult anatomy.
(Cummings Otolaryngology, Chapter 202)
Act III: The T-shaped Inlet and the "Great Occlusion" (Weeks 5-10)
This is the most dramatic act - a temporary crisis that resolves in a miracle of recanalization.
Scene 1: The Arytenoid Swellings Rise (Week 5)
Paired arytenoid swellings erupt from the mesenchyme at the cranial end of the laryngotracheal tube. They grow upward toward the tongue with impressive speed, transforming the slit-like primordial glottis first into a T-shaped laryngeal inlet and then - by sheer overcrowding of proliferating epithelium - into no opening at all.
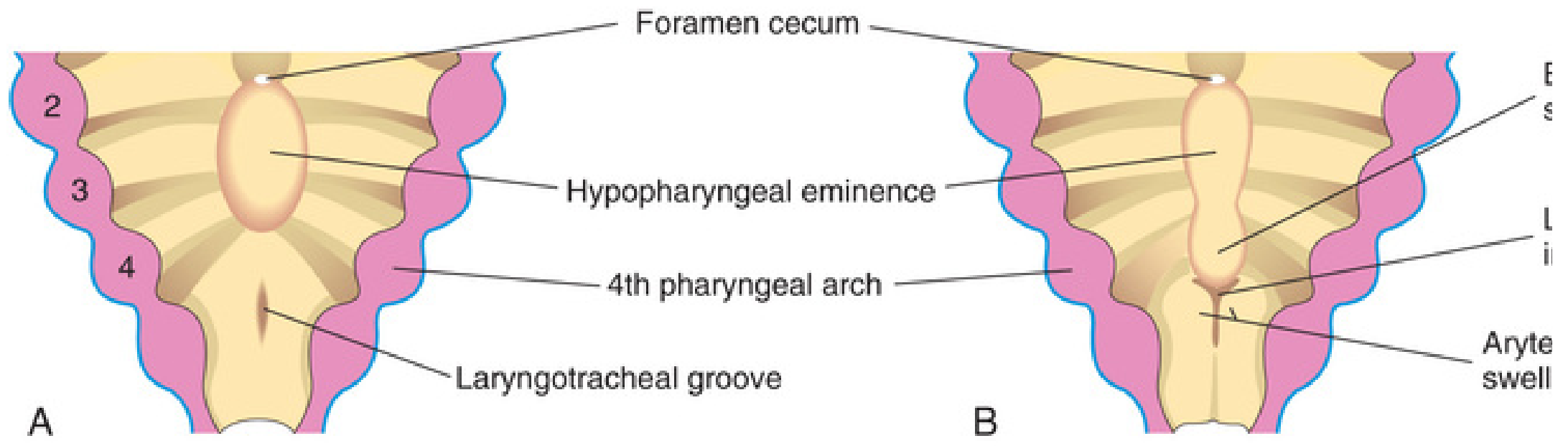
Fig. 10.4 A & B - The developing laryngeal floor at 4 weeks (A) and 5 weeks (B). Note the laryngotracheal groove (A) and the emerging arytenoid swellings (B). The Developing Human, Moore & Persaud
Scene 2: The Great Occlusion (Week 6-9)
The laryngeal epithelium proliferates so rapidly that it completely obliterates the lumen. The larynx is, for a time, a solid plug of tissue - a sealed room. This is normal. The fetus doesn't need to breathe through it yet.
Scene 3: Recanalization - The Room Opens Again (Week 10)
By the 10th week, the epithelium breaks down in an orderly fashion, reopening the lumen. As it does, lateral recesses form - the laryngeal ventricles. The mucous membrane folds bordering these recesses become:
- The vestibular folds (false vocal cords) - upper
- The vocal folds (true vocal cords) - lower
If recanalization fails completely: → Laryngeal atresia (CHAOS syndrome - Congenital High Airway Obstruction Syndrome): airways distal to the block fill with fluid, lungs enlarge massively, diaphragm flattens or inverts, fetal ascites develops. Often fatal from fetal heart failure.
If recanalization is incomplete: → Laryngeal web - a membranous bridge covers part of the glottis, causing a hoarse cry at birth and airway obstruction. Treated by endoscopic dilation.
(The Developing Human, pp. 569-572)
Act IV: The Epiglottis - The Tongue's Southern Gift (Weeks 5-10)
The epiglottis has a unique origin. It does not come from the arytenoid swellings. Instead, it develops from the caudal part of the hypopharyngeal eminence - a mound of mesenchyme produced by proliferation within the ventral ends of the 3rd and 4th pharyngeal arches.
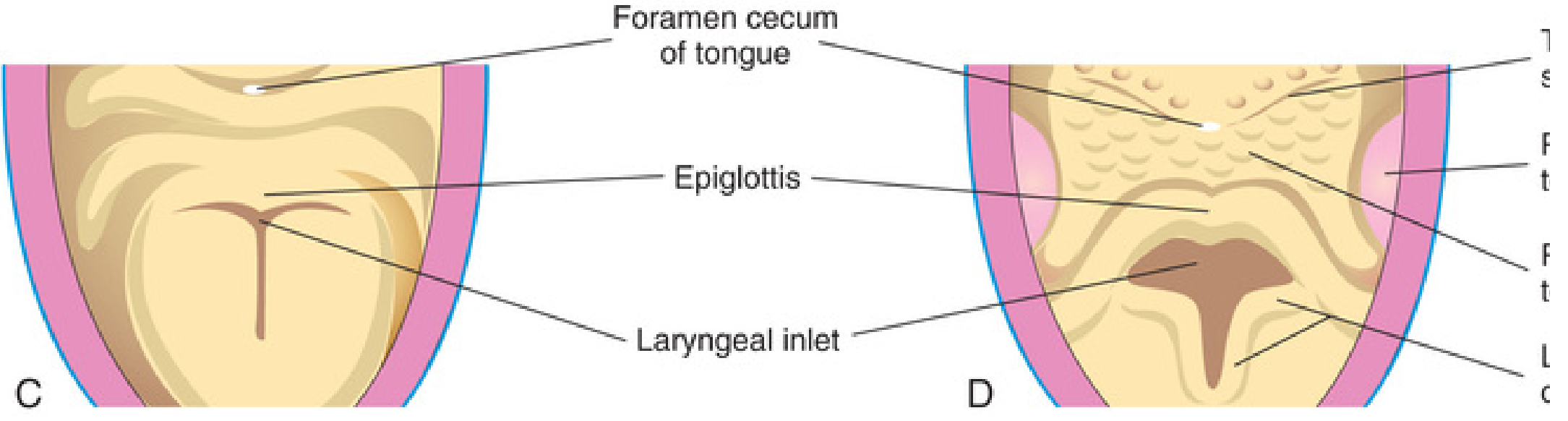
Fig. 10.4 C & D - By week 6 the epiglottis is visible; by week 10 recanalization is complete and the ventricles have formed. The Developing Human, Moore & Persaud
The rostral part of the same hypopharyngeal eminence contributes to the posterior third (pharyngeal part) of the tongue. So the epiglottis and the back of your tongue are siblings - born from the same mesenchymal mound.
Epilogue: The Newborn Larynx - A High Rider
At birth, the larynx is proportionally smaller and sits much higher in the neck than in the adult - opposite the level of C3-C4 (vs C5-C6 in adults). This high position has a beautiful physiological purpose:
- The epiglottis can actually contact the soft palate
- This creates nearly separate respiratory and digestive passages
- The neonate can suckle and breathe simultaneously
- Neonates are obligate nasal breathers as a result
Structural descent occurs progressively over the first 2 years of life. At puberty, testicular androgens drive a dramatic enlargement - the male AP diameter almost doubles (to ~36 mm), increasing vocal fold length from ~6-8 mm to ~15-18 mm, causing voice "breaking."
(Scott-Brown's Otorhinolaryngology Vol. 2, Table 33.1)
The Full Cast: Summary Table
| Event | Timing | Structure Formed | Embryological Origin |
|---|---|---|---|
| Laryngotracheal groove appears | Week 4 | Laryngotracheal diverticulum | Endoderm of foregut floor |
| TE septum formation | Week 4-5 | Separates trachea from esophagus | Tracheoesophageal folds fusing |
| Arytenoid swellings appear | Week 5 | Arytenoid cartilages, glottic inlet | Neural crest mesenchyme (Arch 6) |
| T-shaped inlet forms | Week 5-6 | Laryngeal inlet shape | Arytenoid swelling proliferation |
| Epiglottis forms | Week 5-6 | Epiglottis | Hypopharyngeal eminence (Arch 3+4) |
| Laryngeal lumen occluded | Week 6-9 | (temporary solid plug) | Endodermal epithelial proliferation |
| Recanalization | Week 10 | Vocal folds, vestibular folds, ventricles | Selective epithelial breakdown |
| Laryngeal cartilages ossify | Variable (adult) | Thyroid ossifies first | Neural crest-derived mesenchyme |
Congenital Anomalies: When the Story Goes Wrong
| Anomaly | Embryological Error | Clinical Feature |
|---|---|---|
| Laryngeal atresia / CHAOS | Failed recanalization (complete) | Hydrops, lung hyperplasia, fetal ascites, fatal |
| Laryngeal web | Incomplete recanalization | Hoarse cry, airway obstruction; endoscopic dilation |
| Laryngeal cleft | Incomplete fusion of arytenoid swellings | Aspiration, recurrent pneumonia |
| Subglottic stenosis (congenital) | Abnormal cricoid development (Arch 6) | Stridor, recurrent croup |
| TEF | Incomplete TE septum formation | Classic presentation: polyhydramnios, choking feeds |
Sources:
- The Developing Human: Clinically Oriented Embryology, Moore & Persaud, pp. 569-572
- Cummings Otolaryngology Head and Neck Surgery, Chapter 202 (Pharyngeal Arch Derivatives)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, Chapter 33 (Growth and Development of the Larynx)
This is a shared conversation. Sign in to Orris to start your own chat.