Differential diagnosis endometriosis , adenomyosis , endometrial cancer , endometrial hyperplasia , endometrial stromal tumor , leiomyoma , explain on clinifeatures and histological basis in order to solve case question s
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is the comprehensive differential diagnosis framework for all six conditions, built from Robbins & Cotran Pathologic Basis of Disease, Robbins & Kumar Basic Pathology, Berek & Novak's Gynecology, and Bailey & Love's Surgery.
Differential Diagnosis: Uterine/Endometrial Pathology
Quick Orientation Map
| Feature | Endometriosis | Adenomyosis | Endometrial Hyperplasia | Endometrial Carcinoma | Endometrial Stromal Tumor | Leiomyoma |
|---|---|---|---|---|---|---|
| Age | Reproductive (3rd-4th decade) | Perimenopausal | Reproductive/perimenopausal | Postmenopausal (Type I); older (Type II) | Perimenopausal (~45-50) | Reproductive age |
| Uterine size | Normal | Diffusely enlarged | Normal | Enlarged/irregular | Irregular | Enlarged, nodular |
| Bleeding type | Dysmenorrhea | Menometrorrhagia | Irregular/heavy | Postmenopausal bleeding | Abnormal uterine bleeding | Menorrhagia |
| Pain | Severe dysmenorrhea, dyspareunia | Dysmenorrhea, dyspareunia | Minimal | Minimal early | Pelvic pain/pressure | Pressure symptoms |
| Infertility | Yes (30-40%) | Possible | Possible | Rare presenting feature | No | Yes (submucosal) |
| Malignant potential | Low (peritoneal/ovarian forms) | No | Atypical form: ~40% have co-existent Ca | Yes - IS malignant | Yes (high-grade) | Extremely rare (<1%) |
1. Endometriosis
Clinical Features
- Affects ~10% of reproductive-age females; peak in 3rd-4th decade
- Classic triad: dysmenorrhea + dyspareunia + infertility (30-40% present with infertility)
- Pelvic pain worse cyclically (because ectopic tissue bleeds with the menstrual cycle)
- Three forms: superficial peritoneal, ovarian ("chocolate cysts"), and deep infiltrating endometriosis
- Menstrual irregularities are common
- On exam: fixed retroverted uterus, uterosacral nodularity, adnexal masses (endometriomas)
- Sites (descending frequency): ovaries > uterine ligaments > rectovaginal septum > cul-de-sac > pelvic peritoneum > bowel serosa
Histological Features
- Diagnostic triad: ectopic endometrial glands + endometrial stroma + hemosiderin-laden macrophages (evidence of cyclical bleeding)
- In some cases, only stroma is present (without glands) - still diagnostic
- "Chocolate cysts" on ovary = endometriomas lined by endometrial epithelium filled with old hemorrhagic material
- Peritoneal deposits show hemosiderin deposits and fibrosis
- Superficial/ovarian forms can be precursors to endometrioid and clear cell carcinoma (ARID1A mutations overlap)
2. Adenomyosis
Clinical Features
- Defined as endometrial tissue within the myometrium (unlike endometriosis, it stays connected to the endometrium - "downgrowth")
- Occurs in up to 20% of uteri
- Symptoms: menometrorrhagia + colicky dysmenorrhea + dyspareunia - particularly worse in the premenstrual period
- Uterus is diffusely, symmetrically enlarged (boggy uterus on exam) - contrast with the asymmetric nodular enlargement of fibroids
- Can co-exist with endometriosis
- No malignant potential on its own
Histological Features
- Irregular nests/islands of endometrial stroma with or without glands embedded within myometrial smooth muscle fascicles
- These islands remain in continuity with the basal endometrium (hallmark distinction from endometriosis)
- Surrounding myometrium shows hypertrophy/hyperplasia (reactive)
- No hemosiderin deposits typically (unlike ectopic endometriosis)
Key Distinction from Endometriosis
- Adenomyosis = within myometrium, continuous with endometrium, no distant sites
- Endometriosis = outside uterus, not in continuity with endometrium, can spread to ovaries/peritoneum/distant sites
3. Endometrial Hyperplasia
Clinical Features
- Results from unopposed estrogen stimulation (endogenous or exogenous)
- Risk factors: anovulatory cycles, PCOS, estrogen-secreting ovarian tumors (granulosa cell tumor), obesity, estrogen-only HRT, tamoxifen use
- Presentation: irregular/heavy uterine bleeding in perimenopausal women; occasionally postmenopausal bleeding
- Uterine size usually normal
- WHO Classification determines prognosis and management:
- Hyperplasia without atypia: ~1-3% risk of progression to carcinoma
- Atypical hyperplasia (EIN): up to 40% already have concurrent carcinoma on hysterectomy - managed by hysterectomy or progestin therapy if fertility desired
Histological Features
- Hyperplasia without atypia: increased gland-to-stroma ratio; glands vary in size and shape; may be dilated (cystic); back-to-back glands focally but stroma retained; no nuclear atypia
- Atypical hyperplasia (EIN): complex, back-to-back glands with branching; nuclear atypia - rounded nuclei, vesicular (open) chromatin, conspicuous nucleoli; cells lose perpendicular orientation to basement membrane
- Molecular: PTEN mutations in >20% of hyperplasias (both with and without atypia)
- Considerable morphologic/genetic overlap with well-differentiated endometrioid carcinoma - accurate distinction may require hysterectomy
4. Endometrial Carcinoma
Clinical Features
Type I (Endometrioid Carcinoma) - 80-85% of cases:
- Postmenopausal women, typically younger (55-65 years)
- Associated with estrogen excess: obesity, nulliparity, late menopause, diabetes, hypertension, PCOS
- Classic presentation: postmenopausal vaginal bleeding (key red flag symptom)
- Arises on a background of endometrial hyperplasia
- Generally well-differentiated, better prognosis; 5-year survival ~85% if stage I
Type II (Serous Carcinoma) - ~10%:
- Older, postmenopausal women, often African descent (2x higher mortality)
- Not estrogen-related; arises from endometrial atrophy
- More aggressive; propensity for extrauterine spread (lymphatic, transtubal)
- 5-year survival only 18-27%, even uterus-confined tumors have 80% recurrence rate
Histological Features
Endometrioid Carcinoma:
- Well-differentiated (Grade 1): glandular pattern mimicking proliferative endometrium, invades myometrium
- Grade 3: predominantly solid growth, loss of gland formation
- Desmoplastic stromal response at invasion front
- Key mutations: PTEN (30-80%), PIK3CA (~40%), KRAS (~25%), ARID1A (~33%), MLH1 silencing (~20%)
- Lynch syndrome association (mismatch repair deficiency)
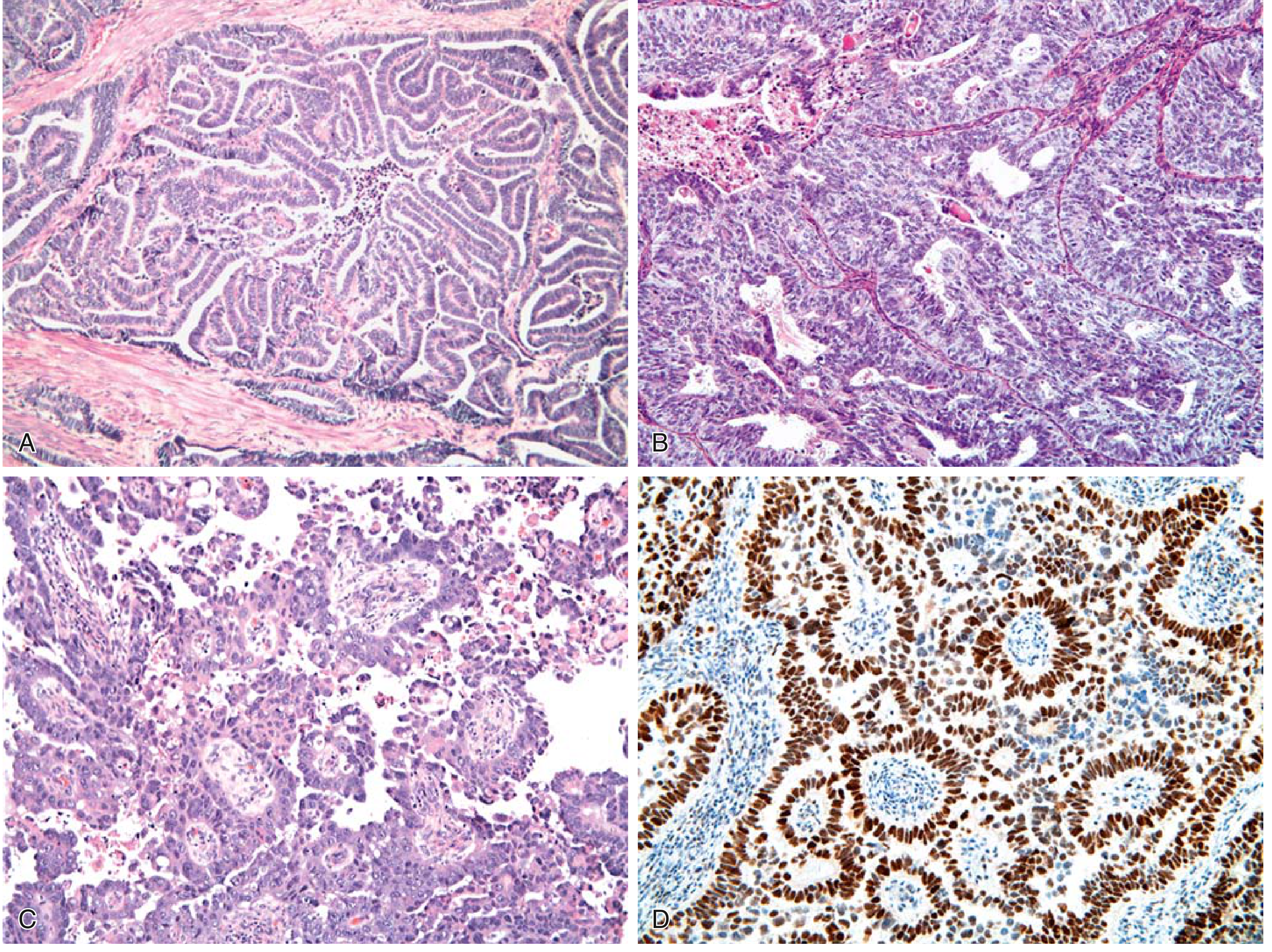
Serous Carcinoma:
- Papillary growth pattern with fronds lined by highly atypical cells
- High nuclear-to-cytoplasmic ratio, hyperchromasia, atypical mitoses
- TP53 mutation is the hallmark (present in precursor "serous EIC" and invasive carcinoma)
- Strong, diffuse p53 immunostaining (IHC marker)
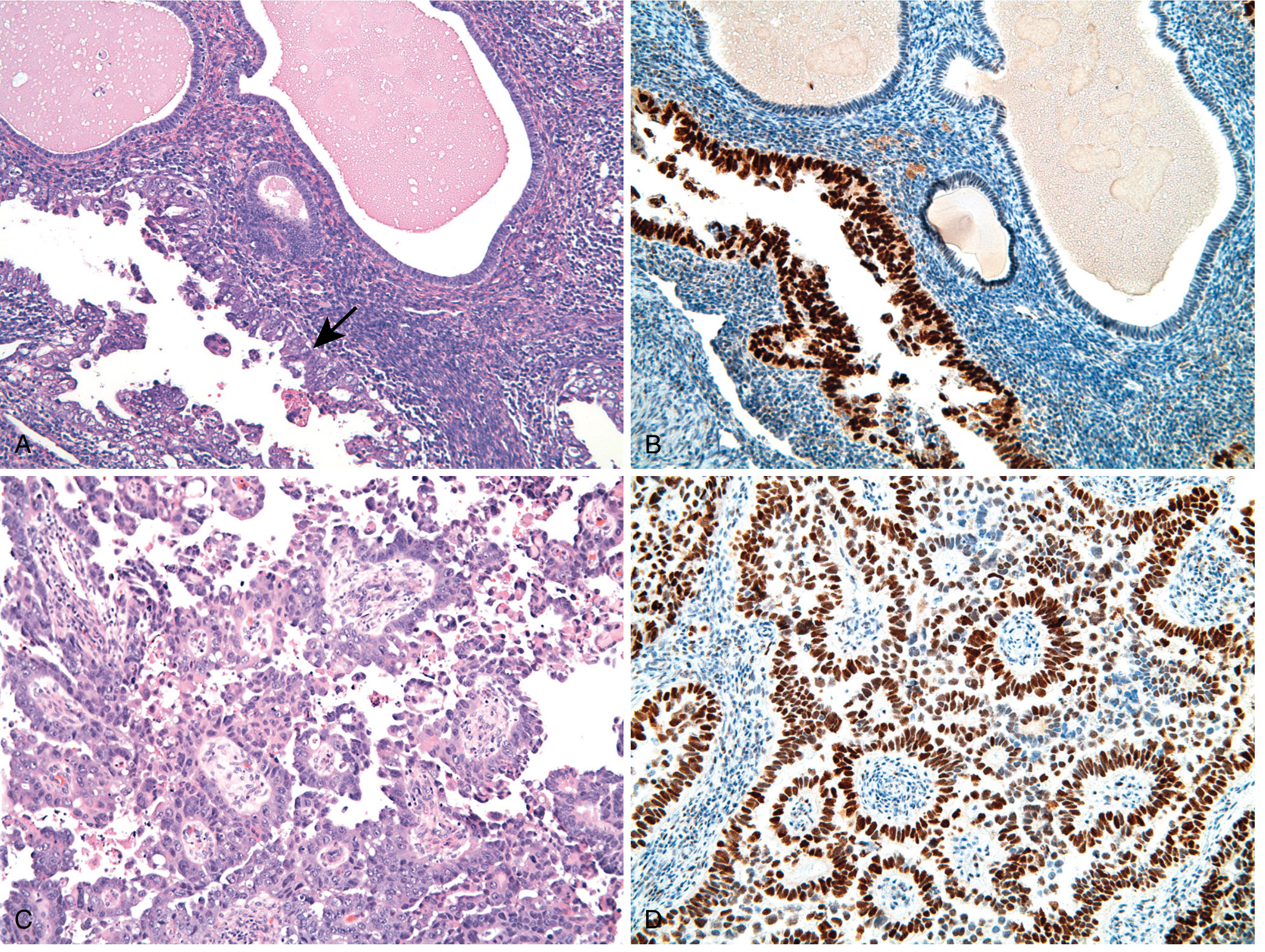
- Precursor: Serous endometrial intraepithelial carcinoma (EIC) - noninvasive, lining gland surfaces
Histology images from Robbins & Kumar Basic Pathology:
Serous carcinoma with EIC precursor (Robbins Cotran):
5. Endometrial Stromal Tumor (ESS)
Clinical Features
- Primarily perimenopausal women (age 45-50); ~1/3 postmenopausal
- Most frequent symptom: abnormal uterine bleeding
- Abdominal pain and pressure from enlarging uterus (less common)
- Pelvic exam: uterine enlargement (regular or irregular); rubbery parametrial induration
- Pre-operative diagnosis is usually mistaken for leiomyoma - diagnosis often made on endometrial biopsy or at surgery
- No apparent relationship to parity or associated conditions; rare in African American women
Classification (WHO):
| Low-Grade ESS | High-Grade ESS / Undifferentiated Sarcoma | |
|---|---|---|
| Mitoses | <10 MF/10 HPF | >10 MF/10 HPF |
| Atypia | Slight | Marked |
| ER/PR | Positive | Negative |
| Behavior | Indolent, 40% extrauterine at diagnosis | Aggressive |
| Molecular | JAZF1-SUZ12 fusion (up to 50%) | Complex alterations |
Histological Features
- Cells resemble normal proliferative-phase endometrial stroma - small, uniform, ovoid cells with scant cytoplasm
- Characteristic "tongue-like" myometrial invasion with permeation of lymphovascular channels (worm-like plugs in vessels)
- Low-grade: minimal atypia, low mitotic rate, ER/PR positive
- High-grade: marked atypia, high mitotic rate, necrosis
- IHC: CD10 positive (stromal marker); ER/PR positive in low-grade; WT1 and SMARCA4 loss in some high-grade
6. Leiomyoma (Uterine Fibroid)
Clinical Features
- Most common tumor in women; more common in African-Caribbean women
- Estrogen and progesterone dependent - shrink after menopause
- Multiple in most cases (contrast with leiomyosarcoma which is almost always solitary)
- Location determines symptoms:
- Submucosal: heavy menorrhagia, infertility, recurrent pregnancy loss; may prolapse through cervical os
- Intramural: heavy periods, endometrial distortion, infertility
- Subserosal: pressure symptoms (urinary frequency/retention, constipation, backache); pedunculated forms mimic ovarian tumor
- Enlarged irregular, nodular uterus on bimanual exam (vs. diffusely boggy in adenomyosis)
- Malignant transformation (<1%) to leiomyosarcoma - extremely rare
- Complications: red degeneration (in pregnancy), torsion of pedunculated fibroid
Histological Features
- Sharply circumscribed, well-defined borders (unlike leiomyosarcoma which is infiltrative)
- Bundles of smooth muscle cells arranged in whorled/intersecting fascicles
- Cells morphologically identical to normal myometrium - bland spindle cells, abundant eosinophilic cytoplasm, cigar-shaped nuclei, no atypia
- No significant mitotic activity (contrast with leiomyosarcoma: >10 MF/10 HPF)
- May show secondary changes: hyaline degeneration (most common), cystic, red/carneous (pregnancy), calcific, fatty degeneration
- Gross: gray-white, firm, whorled cut surface
- Molecular: MED12 mutations in ~70%; chromosomal rearrangements of 6 and 12
Critical Histological Distinctions for Case Questions
| Histological Finding | Diagnosis |
|---|---|
| Endometrial glands + stroma OUTSIDE uterus + hemosiderin | Endometriosis |
| Endometrial islands WITHIN myometrium, continuous with endometrium | Adenomyosis |
| Increased gland:stroma ratio, NO atypia | Hyperplasia without atypia |
| Back-to-back glands, vesicular nuclei, conspicuous nucleoli | Atypical hyperplasia (EIN) |
| Glandular invasion of myometrium, PTEN/PIK3CA mutations | Endometrioid carcinoma |
| Papillary pattern, marked atypia, diffuse p53 IHC | Serous carcinoma |
| Small uniform oval cells resembling stromal cells, "worm-like" vascular invasion, CD10+ | Endometrial Stromal Sarcoma |
| Whorled smooth muscle bundles, sharp margins, NO atypia, NO mitoses | Leiomyoma |
Clinical Clue Summary for MCQs
- Postmenopausal bleeding → always think endometrial carcinoma first; work up with endometrial biopsy
- Severe dysmenorrhea + infertility + normal uterus → endometriosis (look for adnexal mass/chocolate cyst)
- Diffusely enlarged boggy uterus + dysmenorrhea + heavy menses → adenomyosis
- Irregular nodular uterus + heavy menses, asymptomatic → leiomyoma
- Irregular heavy bleeding + risk factors (obesity, PCOS, anovulation) → endometrial hyperplasia
- Uterine enlargement mistaken for fibroids on exam, abnormal bleeding in 45-50 yo → think endometrial stromal sarcoma (CD10+, JAZF1-SUZ12 fusion)
- Tamoxifen use → risk for endometrial hyperplasia AND endometrial polyps
- Lynch syndrome (MMR defect) → increased risk of endometrioid carcinoma (MLH1 silencing)
- Obese + hypertensive + diabetic + postmenopausal bleeding → classic Type I (endometrioid) carcinoma triad
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 929-935; Robbins & Kumar Basic Pathology, p. 692, 718; Berek & Novak's Gynecology, p. 2194; Bailey and Love's Short Practice of Surgery 28th Ed., p. 1609
This is a shared conversation. Sign in to Orris to start your own chat.