TCC of bladder 25 marks Rguhs radiology ans
Reading File
Finding Sources
Finding Sources
Searching the Web
RGUHS radiology 25 marks TCC transitional cell carcinoma bladder answer
Finding Sources
Reading Web Page
https://radiopaedia.org/articles/urothelial-carcinoma-urinar…
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent! I now have comprehensive information. Let me compile the complete 25-mark RGUHS radiology answer on TCC of the Bladder.
Transitional Cell Carcinoma (TCC) of the Urinary Bladder - Radiology
(25 Marks - RGUHS Radiology Answer)
1. Introduction
Transitional cell carcinoma (TCC), now preferably termed urothelial carcinoma (UC), is the most common primary neoplasm of the urinary bladder, accounting for approximately 90% of all bladder cancers. It is the most common tumor of the entire urinary system. It is more common in males (M:F = 3:1), with peak incidence in the 6th-7th decades.
2. Etiology / Risk Factors
- Cigarette smoking - single most important risk factor
- Occupational exposure: aromatic amines (rubber, plastic manufacturing), arylamines, polycyclic aromatic hydrocarbons
- Schistosoma haematobium infection (associated with squamous cell carcinoma)
- Cyclophosphamide therapy (dose-response pattern)
- Chronic bladder irritation, calculi
- Analgesic abuse (phenacetin)
3. Pathology
Gross appearance:
- Papillary (exophytic) - most common form; frond-like projections into lumen; low grade
- Sessile/flat - higher grade; more likely to invade muscle
- Carcinoma in situ (CIS) - flat, high-grade intraepithelial lesion; red velvety patches on cystoscopy
Location: Most common at the trigone and posterolateral walls near the ureteric orifices
Histology:
- Urothelial cells with nuclear pleomorphism, mitoses
- Papillary cores with fibrovascular stroma
- WHO grading: Low-grade vs. High-grade (2004 classification)
4. Clinical Features
- Painless gross hematuria - most common presenting symptom (~85% of cases)
- Irritative voiding symptoms (urgency, frequency, dysuria) - especially in CIS
- Recurrent UTI
- Obstructive symptoms if near ureteric orifice
5. Imaging Modalities
A. Intravenous Urography (IVU) / Excretory Urography
Historically the first-line imaging:
- Filling defect in the bladder - most common finding; papillary mass projects into the lumen
- Lobulated/irregular intraluminal filling defect that does not move with patient positioning (unlike calculus)
- Absent nephrogram or delayed/diminished excretion if ureteric orifice involved with hydronephrosis
- Upper tract TCC may show: filling defects in renal pelvis/ureter, "goblet sign" (dilatation below the lesion in ureter), irregular mucosal margins
- Limitation: Poor soft tissue contrast; cannot assess depth of invasion
Cystogram phase: Irregular nodular soft tissue density filling defect projecting into contrast-filled bladder
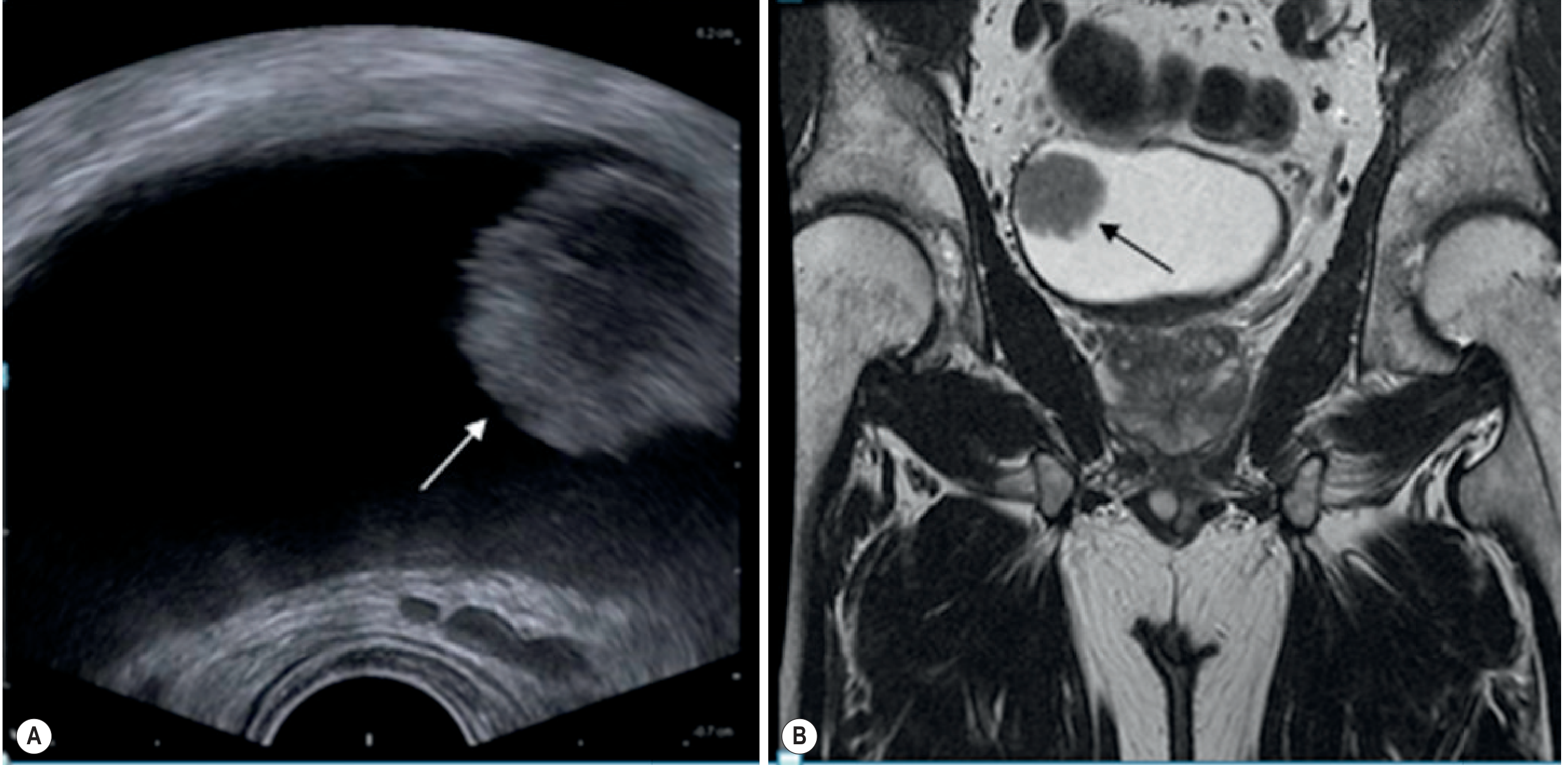
B. Ultrasound (USG)
- First-line modality for patients presenting with hematuria
- TCC appears as an echogenic, non-mobile, polypoid mass projecting into the bladder lumen
- Attached to the bladder wall, no posterior acoustic shadowing (differentiates from calculus)
- Doppler: Shows intrinsic vascularity within the mass (helps differentiate from blood clot which is avascular)
- Transabdominal US - good for larger lesions; limited for small (<5 mm) lesions and flat lesions (CIS)
- Transrectal/Transvaginal US - better for posterior wall lesions and trigone
- Endoluminal US - can assess depth of invasion (T staging)
- Limitations: Cannot reliably stage; operator dependent; poor for flat lesions; limited for thick-walled bladder
Key finding on USG: Echogenic, non-shadowing, non-mobile intraluminal mass with internal vascularity on Doppler
C. Computed Tomography (CT) / CT Urography (CTU)
CT Urography is the current gold standard for hematuria evaluation and staging.
CT findings:
- Non-contrast phase: Isodense or slightly hyperdense mass against the low-density urine
- Post-contrast phases:
- Corticomedullary phase - demonstrates vascularity of mass; shows early enhancement
- Nephrographic phase - peritumoral enhancement; wall thickening
- Excretory/Urographic phase - filling defect in opacified bladder; most important phase
Appearances:
- Papillary TCC: Enhancing polypoid, pedunculated, or sessile mass; frond-like projections
- Sessile TCC: Focal or diffuse bladder wall thickening with irregular inner surface
- CIS: Usually normal CT or diffuse mucosal enhancement - often invisible on CT
CT Staging (Jewett-Marshall / TNM):
| Stage | CT Features |
|---|---|
| Ta/T1 | Intraluminal mass; normal outer bladder wall |
| T2 (muscle invasion) | Thickened wall; blurring of internal perivesical fat |
| T3a (microscopic perivesical) | Cannot be reliably detected by CT |
| T3b (macroscopic perivesical) | Irregular bladder wall; soft tissue stranding in perivesical fat |
| T4a | Direct invasion of prostate, uterus, vagina - loss of fat plane |
| T4b | Invasion of pelvic wall/abdominal wall - fixed mass |
| N+ | Lymph node enlargement >10 mm (obturator, iliac chains) |
| M1 | Distant metastases: liver, lung, bone |
CT advantages:
- Best for assessing extravesical extension (T3b, T4)
- Lymph node assessment
- Distant metastases (staging CT of chest, abdomen, pelvis)
- Upper tract evaluation for synchronous TCC (renal pelvis, ureter)
- Hydronephrosis detection
CT limitations:
- Cannot distinguish T2 from T3a (microscopic perivesical invasion)
- Post-TURBT changes cause overstaging
- Limited for CIS
- Overall CT staging accuracy ~55-70%
D. Magnetic Resonance Imaging (MRI)
MRI is the best modality for local staging of bladder cancer.
MRI protocol:
- T1W: Tumor is isointense to muscle; detects lymph nodes and bone marrow metastases
- T2W (most important): Tumor appears intermediate signal against high signal urine and low signal muscle
- Intact low-signal outer muscle wall = no muscle invasion (T1)
- Disruption of low-signal muscle band = muscle invasion (T2)
- Perivesical fat stranding on T2 = T3b
- DWI (Diffusion-Weighted Imaging): TCC restricts diffusion; high signal on DWI, low ADC values; helps detect CIS and small flat lesions
- DCE-MRI (Dynamic Contrast Enhanced): Early enhancement of tumor relative to bladder wall; good for assessing depth of invasion
MRI T staging:
- T2 vs T3a distinction: Best on MRI (better soft tissue contrast than CT)
- Perivesical fat invasion on fat-suppressed T1W post-contrast
- Organ invasion (prostate, seminal vesicles, vagina, uterus) clearly shown
- Lymph nodes: Size criteria same as CT; functional MRI (DWI) may improve nodal detection
MRI advantages over CT:
- Better soft tissue contrast
- Superior local staging (especially T2 vs T3)
- No radiation
- Better for assessment of pelvic organ involvement
E. Retrograde Pyelography (RGP)
- Used when IVU/CTU inconclusive or contraindicated (renal failure, contrast allergy)
- Shows filling defects in collecting system for upper tract TCC
- "Stippled nephrogram" appearance with papillary lesions
- Can be combined with ureteroscopy for biopsy
F. Positron Emission Tomography (PET-CT)
- FDG-PET has limited role in primary diagnosis (FDG excreted in urine causing bladder activity)
- Role: Detection of lymph node metastases and distant metastases in staging
- 18F-NaF PET - for bone metastasis evaluation
6. TNM Staging System (2017)
Tis - Carcinoma in situ (flat)
Ta - Non-invasive papillary carcinoma
T1 - Invades subepithelial connective tissue (lamina propria)
T2a - Invades superficial muscle (inner half)
T2b - Invades deep muscle (outer half)
T3a - Microscopic perivesical invasion
T3b - Macroscopic perivesical invasion
T4a - Invades prostate, uterus, or vagina
T4b - Invades pelvic wall or abdominal wall
N0 - No regional lymph nodes
N1 - Single node ≤2 cm (true pelvis)
N2 - Single node 2-5 cm or multiple nodes ≤5 cm
N3 - Lymph node >5 cm
M0/M1 - No distant/distant metastasis
Non-muscle invasive (NMIBC): Ta, T1, CIS (~70-80% at presentation)
Muscle invasive (MIBC): T2-T4 (~20-30%)
7. Imaging Algorithm for Suspected Bladder TCC
Hematuria (painless, adult)
↓
USG Abdomen + Pelvis
(initial, non-invasive)
↓
Filling defect/mass seen → CT Urography (3-phase)
(also evaluates upper tract)
↓
Cystoscopy + Biopsy (gold standard for diagnosis)
↓
If muscle-invasive on TURBT → MRI Pelvis for local staging
↓
CT Chest + Abdomen + Pelvis for distant staging
8. Differential Diagnosis on Imaging
| Condition | Differentiating Feature |
|---|---|
| Blood clot | Avascular on Doppler; mobile; resolves on repeat scan |
| Prostate carcinoma invading bladder | Arises from base; large prostate mass |
| Endometriosis | Female; cyclic hematuria; wall thickening, no intraluminal mass |
| Cystitis cystica | Multiple small submucosal cysts; history of infection |
| Leiomyoma | Submucosal; homogeneous; smooth margin |
| Bladder calculus | Posterior acoustic shadow; moves with position; dense on CT |
| Neurofibromatosis | Multiple lesions; known NF1 |
9. Radiology-Guided Procedures
- CT-guided biopsy - rarely needed; cystoscopy preferred
- Image-guided nephrostomy - for obstructive uropathy from ureteric involvement
- Radiological staging guides treatment: TURBT for NMIBC; radical cystectomy or chemoradiation for MIBC
10. Summary / Key Points for RGUHS
- TCC is the most common bladder tumor (90%); presents with painless hematuria
- CT Urography is the imaging investigation of choice for hematuria evaluation and staging
- MRI is best for local staging, particularly distinguishing T2 from T3 disease
- USG is the first-line modality; shows echogenic, non-mobile, vascular intraluminal mass
- IVU shows filling defects; historically important but now replaced by CTU
- Cystoscopy + biopsy remains the gold standard for diagnosis
- Staging guides treatment: NMIBC (Ta, T1, CIS) → endoscopic; MIBC (T2+) → radical surgery/chemoradiation
- Upper tract TCC must be sought (synchronous in 2-4%)
- CT: best for lymph nodes and metastases; MRI: best for local soft tissue staging
- DWI-MRI and DCE-MRI improve staging accuracy
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751); Campbell-Walsh-Wein Urology (9780323546423); Robbins & Cotran Pathologic Basis of Disease (9780443264528); Radiopaedia - Urothelial Carcinoma Bladder
Neurogenic bladder my style
Reading File
Finding Sources
Finding Sources
Searching the Web
neurogenic bladder radiology RGUHS imaging findings VCUG MRI ultrasound classification
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://radiologykey.com/bladder-and-ureteral-imaging
Reading File
Reading File
I now have everything needed. Let me compile the full answer in "my style" - same format as the TCC answer above.
Neurogenic Bladder - Radiology
(RGUHS Radiology - 25 Marks)
1. Introduction
Neurogenic bladder (NGB) refers to dysfunction of the urinary bladder due to disease or injury of the nervous system. It is not a single disease but a spectrum of disorders - the exact manifestation depends on the level and completeness of the neurological lesion. The primary radiological concern is identifying the functional type, assessing bladder morphology, detecting complications (hydronephrosis, VUR, stones), and monitoring upper tract deterioration - which can occur silently without symptoms.
2. Neuroanatomy (Brief)
Normal micturition requires an intact spinobulbospinal reflex arc:
Cerebral cortex (voluntary control)
↓
Pontine Micturition Centre (PMC / Barrington's nucleus) - coordinates detrusor and sphincter
↓
Sacral cord (S2-S4) - parasympathetic outflow → detrusor contraction
↓
Pudendal nerve / sympathetic (T10-L2) → sphincter function
- Parasympathetic (S2-S4): Detrusor contraction - via M2/M3 receptors (acetylcholine)
- Sympathetic (T10-L2): Bladder neck/internal sphincter closure - via α1 receptors; detrusor relaxation via β3 receptors
- Somatic (pudendal, S2-S4): External urethral sphincter (voluntary)
3. Classification
A. Lapides Classification (Most Exam-Relevant)
| Type | Lesion Level | Detrusor | Sensation | Capacity | Key Feature |
|---|---|---|---|---|---|
| Uninhibited neurogenic | Above PMC (cortex, CVA, Parkinson's) | Overactive | Intact | Reduced | Urgency incontinence; no DSD |
| Reflex neurogenic | Between PMC and S2-S4 (spinal cord) | Overactive | Absent | Small | DSD; autonomic dysreflexia |
| Autonomous neurogenic | Sacral cord / conus (S2-S4) | Areflexic | Absent | Large | No reflex; overflow incontinence |
| Motor paralytic | Motor efferents only (cauda equina motor) | Acontractile | Intact | Large | Urinary retention; sensation present |
| Sensory neurogenic | Afferent limb only (DM, tabes dorsalis) | Normal | Absent | Large | Overflow; no sensation of filling |
B. Urodynamic Classification (Krane-Siroky - Used in Practice)
- Detrusor Overactivity (DO) - with coordinated sphincters / striated sphincter dyssynergia (DSD) / smooth sphincter dyssynergia
- Detrusor Areflexia - with coordinated sphincters / nonrelaxing striated sphincter / denervated striated sphincter
C. Functional Classification (ICS)
- Failure to store (overactive bladder, low compliance)
- Failure to empty (areflexic/acontractile detrusor, bladder outlet obstruction)
4. Etiology by Level
| Level | Common Causes |
|---|---|
| Suprapontine | CVA, Parkinson's disease, multiple system atrophy, brain tumors, dementia |
| Spinal cord (above S2) | Spinal cord injury (SCI), multiple sclerosis, transverse myelitis, cervical spondylosis |
| Sacral/Infrasacral | Myelomeningocele (spina bifida), sacral agenesis, cauda equina syndrome, lumbar disc prolapse, pelvic surgery |
| Peripheral | Diabetes mellitus (most common cause), Guillain-Barré syndrome, pelvic surgery, herpes zoster |
5. Clinical Features
- Overactive/Spastic NB: Urgency, frequency, urgency incontinence, small voided volumes, may have autonomic dysreflexia (SCI above T6)
- Underactive/Flaccid NB: Incomplete emptying, overflow incontinence, straining to void, recurrent UTI
- Detrusor-Sphincter Dyssynergia (DSD): Simultaneous contraction of detrusor and external sphincter - high-pressure voiding - major cause of upper tract damage
6. Radiological Investigations
A. Plain X-ray (KUB)
- Limited role for the bladder itself
- May show spinal anomalies - spina bifida occulta, sacral agenesis, vertebral defects
- Bladder calculi (from stasis and recurrent UTI) - radio-opaque stones
- Renal calculi (secondary to hydronephrosis)
- Spinal cord injuries - vertebral fracture/dislocation
B. Ultrasound (USG)
First-line, non-invasive, radiation-free - initial and surveillance modality of choice.
Bladder findings:
- Spastic (high-pressure) NB:
- Thickened bladder wall (>3 mm when full, >5 mm when empty)
- Trabeculation - irregular lumpy inner surface
- Diverticula - multiple pseudo-diverticula (mucosa herniating between hypertrophic muscle bundles)
- Small bladder capacity
- Flaccid (low-pressure) NB:
- Large, smooth-walled bladder
- Markedly elevated post-void residual (PVR)
- Thin wall
- Both types:
- Bladder calculi (dependent echogenic foci with posterior shadowing)
- VUR-related changes
Upper tract findings:
- Hydronephrosis / hydroureteronephrosis - due to high intravesical pressure, DSD, or VUR
- Renal parenchymal thinning (chronic obstruction)
- Renal scarring (recurrent pyelonephritis)
- Ureteric dilatation ("yo-yo" peristalsis pattern)
Role of USG:
- Measure PVR (normal <100 mL)
- Bladder wall thickness assessment
- Detect diverticula and stones
- Monitor upper tract on a regular/serial basis
- Guide suprapubic catheter insertion
C. Voiding Cystourethrogram (VCUG) / Micturating Cystourethrogram (MCU)
Most important and specific radiological test for neurogenic bladder.
Technique: Bladder filled retrograde with iodinated contrast via catheter → images taken during filling and voiding phases
Key Findings:
1. "Christmas Tree" Bladder (Pine Tree / Fir Tree Sign)
- Pathognomonic of spastic/UMN neurogenic bladder (classically spina bifida with LMN)
- AP image shows a tall, narrow, pointed bladder superiorly with irregular serrated margins
- Trabeculation gives the outline a "jagged/pine tree" appearance
- Multiple diverticula resembling pine tree branches
- Trabeculation spares the bladder base (trigone)
- Seen in: myelomeningocele, spinal cord injury (chronic phase)
2. Vesicoureteric Reflux (VUR)
- Contrast seen tracking into ureter(s) on VCUG
- Common in high-pressure neurogenic bladder
- Graded I-V (International Classification)
- Bilateral VUR with hydronephrosis = poor prognosis for upper tracts
3. Bladder Neck / Urethral Abnormalities
- Open bladder neck at rest = internal sphincter incompetence (LMN)
- Tight/non-relaxing bladder neck = sympathetic DSD
- Spinning top urethra = in females; non-relaxing external sphincter
- DSD appearance: Proximal urethra dilated; external sphincter contracts during voiding - appearance of "figure 8" or dilated posterior urethra with abrupt cut-off
4. Large Smooth Bladder (Flaccid / LMN)
- Huge, smooth-walled, featureless bladder
- Open or lax bladder neck
- Poor/absent detrusor contraction during voiding phase
- Elevated PVR
5. Bladder Diverticula
- Saccular outpouchings; thin-necked (pseudo-diverticula in NB)
- May persist post-voiding
6. Upper Tract Appearance on VCUG
- VUR grade and extent documented
- Intrarenal reflux (grade V) - worst prognostic sign
D. Video-Urodynamics (VUD) - Gold Standard
- Combines VCUG fluoroscopy + multichannel urodynamics simultaneously
- Real-time visualization of bladder behavior during filling and voiding with pressure measurement
- Criteria standard for neurogenic bladder evaluation
- Assesses:
- Bladder compliance (normal: >40 mL/cmH₂O)
- Detrusor Leak Point Pressure (DLPP): >40 cmH₂O = high risk of upper tract damage
- DSD (simultaneous EMG activity of external sphincter with detrusor contraction)
- VUR during filling vs. voiding phase
- Recommended for all high-risk patients (spina bifida, SCI) before surgical planning
E. Intravenous Urography (IVU)
- Largely replaced by CT Urography
- Shows: dilated renal pelves/ureters, cortical thinning, impaired contrast excretion
- May show bladder trabeculation on cystogram phase
- Bladder: filling defects from trabeculation or stones
F. CT Scan / CT Urography (CTU)
Best for overall anatomical survey and complications.
Bladder findings on CT:
- Wall thickening - uniform >3 mm
- Trabeculation - irregular inner surface
- Diverticula - air/contrast-filled outpouchings
- Calculi - hyperdense foci (most sensitive modality)
- Small (spastic) or large (flaccid) bladder on CT
Upper tract findings:
- Hydronephrosis, hydroureter, ureteric tortuosity
- Cortical thinning, renal scarring
- Perinephric fat stranding (infection)
Spinal imaging:
- CT spine: vertebral anomalies, sacral agenesis, fractures
- CT myelogram: in patients who cannot have MRI (metallic implants)
G. MRI
Best modality for identifying the underlying neurological cause and for local soft-tissue assessment.
Spinal cord MRI:
- Sequence of choice: T1W + T2W sagittal and axial; DWI; Gadolinium-enhanced
- Tethered cord: Conus medullaris at or below L2; thickened filum terminale (>2 mm); fat signal in filum (lipoma)
- Myelomeningocele/meningocele: Posterior meningeal sac, neural elements within
- Syringomyelia/Hydromyelia: T2 hyperintense central canal fluid signal
- Spinal cord injury: T2 hyperintensity (edema/contusion), cord compression, cord atrophy (chronic)
- Multiple sclerosis: Periventricular and cord plaques (T2/FLAIR hyperintense)
- Sacral agenesis: Absent sacral segments; "scimitar sacrum" appearance
- Diastematomyelia: Split cord on axial MRI
Bladder MRI (T2W):
- Thickened, trabeculated wall - intermediate signal mass
- Diverticula as T2 bright outpouchings
- DWI helps detect bladder wall changes
- MR urography: hydronephrosis without radiation/contrast
H. Radionuclide Studies
- DMSA scan: Renal cortical scarring (most sensitive); differential renal function
- DTPA/MAG3 scan: Obstruction vs. dilatation distinction; GFR estimation; drainage curve post-furosemide
- Important in neurogenic bladder follow-up to detect functional renal deterioration before serum creatinine rises
7. Summary of Imaging Findings
| Modality | Key Findings in Neurogenic Bladder |
|---|---|
| USG | Thickened wall, trabeculation, diverticula, elevated PVR, hydronephrosis |
| VCUG | Christmas tree bladder, VUR, DSD appearance, smooth large bladder, open bladder neck |
| Video-UDS | DLPP >40 cmH₂O, DSD, poor compliance, VUR during filling - GOLD STANDARD |
| CT | Wall thickening, calculi, diverticula, hydroureteronephrosis, spinal anomalies |
| MRI | Underlying cause - tethered cord, MS plaques, SCI, myelomeningocele |
| DMSA | Renal scarring, differential function |
| DTPA/MAG3 | Obstruction, drainage, GFR |
8. Complications Detected on Imaging
- Hydronephrosis / Chronic Kidney Disease - USG, CTU, DTPA
- Vesicoureteric Reflux (VUR) - VCUG (graded I-V)
- Recurrent Urinary Tract Infections - USG (thickened wall, debris), DMSA (scarring)
- Bladder Calculi - CT (most sensitive), plain KUB, USG
- Autonomic Dysreflexia (SCI above T6) - clinical; bladder distension is commonest trigger
- Bladder cancer - increased risk with chronic inflammation; detected on CT/cystoscopy
9. Imaging Algorithm
Neurogenic Bladder (known or suspected)
↓
USG (Bladder + Kidneys + PVR)
KUB (spinal anomalies, calculi)
↓
VCUG / MCU
(morphology + VUR assessment)
↓
Video-Urodynamics (VUD)
[High-risk: SCI, spina bifida]
[Gold standard for functional assessment]
↓
MRI Spine (if cause unknown or tethered cord suspected)
↓
CT Abdomen/Pelvis
(complications: stones, hydronephrosis)
↓
DMSA / MAG3
(renal function, scarring - serial surveillance)
10. Management Principles (Radiology-relevant)
| Dysfunction | First-line Treatment |
|---|---|
| Neurogenic DO (storage) | Anticholinergics (oxybutynin, solifenacin); Botulinum toxin A intravesical injection (image-guided) |
| Urinary retention (flaccid) | Clean Intermittent Catheterization (CIC); suprapubic catheter (USG-guided insertion) |
| High DLPP with poor compliance | Augmentation cystoplasty (surgical); urinary diversion |
| VUR | CIC + anticholinergics; Deflux injection (endoscopic, image-guided); reimplantation |
| Bladder stones | Endoscopic/percutaneous lithotripsy; detected on CT/USG |
| Obstructive uropathy | Percutaneous nephrostomy (image-guided) |
11. Key Points for Exam
- Neurogenic bladder = bladder dysfunction from any neurological cause; manifestation depends on level of lesion
- Christmas tree / pine tree bladder on VCUG = spastic (UMN/suprasacral) neurogenic bladder
- Video-urodynamics is the gold standard; DLPP >40 cmH₂O = risk of upper tract damage
- USG is first-line and surveillance modality; MRI identifies the underlying neurological cause
- DSD (Detrusor-Sphincter Dyssynergia) is the most dangerous urodynamic pattern - seen in suprasacral SCI
- DMSA detects renal scarring before serum creatinine rises
- VUR on VCUG is common - high intravesical pressure drives reflux
- Sacral agenesis, tethered cord, myelomeningocele = commonest causes in children; SCI, DM, MS in adults
- PVR >100 mL = significant retention; must be measured serially
- Primary goal of management AND imaging: protect the upper urinary tracts
Sources: Smith & Tanagho's General Urology 19e (9781259834332); Campbell-Walsh-Wein Urology (9780323546423); Grainger & Allison's Diagnostic Radiology (9780323760751); Radiology Key - Bladder & Ureteral Imaging
10 mark
The user wants the same Neurogenic Bladder answer condensed to 10-mark format (same style, but shorter/tighter). No new research needed - I have all the content from the previous answer.
Neurogenic Bladder
(10 Marks - RGUHS Radiology)
1. Definition
Neurogenic bladder is dysfunction of the urinary bladder resulting from disease or injury of the central or peripheral nervous system. The type of dysfunction depends on the level of the neurological lesion.
2. Classification (Lapides - Most Important)
| Type | Lesion | Bladder |
|---|---|---|
| Uninhibited | Cortex / CVA / Parkinson's | Overactive, urgency incontinence |
| Reflex | Spinal cord (above S2) | Overactive + DSD, no sensation |
| Autonomous | Sacral cord (S2-S4) | Areflexic, large, overflow |
| Motor paralytic | Motor efferents / cauda equina | Acontractile, retention, sensation intact |
| Sensory | Afferent only (DM, tabes) | Large, no filling sensation |
Rule: Lesions above sacral cord (S2-S4) → spastic/overactive bladder; lesions at or below sacral cord → flaccid/areflexic bladder
3. Radiological Investigations
A. Plain X-ray (KUB)
- Spinal anomalies: spina bifida occulta, sacral agenesis, vertebral defects
- Bladder and renal calculi (radio-opaque)
B. Ultrasound - First-Line / Surveillance Modality
Spastic NB:
- Thickened bladder wall (>3 mm when full)
- Trabeculation, pseudo-diverticula
- Small bladder capacity
Flaccid NB:
- Large, smooth, thin-walled bladder
- Massively elevated Post-Void Residual (PVR)
Both: Hydronephrosis, hydroureter, renal scarring, calculi
C. VCUG / MCU - Most Specific Radiological Test
Key findings:
1. "Christmas Tree" Bladder
- Pathognomonic of spastic (suprasacral) neurogenic bladder
- Tall, narrow, pointed bladder superiorly
- Trabeculated, serrated irregular margins
- Multiple diverticula resembling pine branches
- Trigone/bladder base spared
- Seen in: myelomeningocele, chronic SCI
2. Vesicoureteric Reflux (VUR)
- Contrast tracking into ureters/renal pelves
- Graded I-V; indicates high intravesical pressure
3. Large Smooth Bladder (Flaccid)
- Featureless, huge bladder; open/lax bladder neck
- Poor/absent detrusor contraction on voiding
4. Detrusor-Sphincter Dyssynergia (DSD)
- Dilated posterior urethra with abrupt cut-off at external sphincter
- Most dangerous pattern - causes high-pressure voiding and upper tract damage
D. Video-Urodynamics (VUD) - Gold Standard
- Combines VCUG fluoroscopy + multichannel pressure measurement
- Key parameters:
- DLPP >40 cmH₂O = high risk of upper tract damage
- Bladder compliance (normal >40 mL/cmH₂O)
- DSD detection on EMG + fluoroscopy
- Mandatory in SCI and spina bifida patients
E. MRI Spine
- Best for identifying the underlying neurological cause
- Tethered cord: Conus below L2, thickened filum terminale
- Myelomeningocele: Posterior neural sac
- SCI: T2 cord signal change, compression, atrophy
- MS plaques, sacral agenesis, diastematomyelia
F. CT / DMSA / MAG3
- CT: Calculi (most sensitive), diverticula, hydronephrosis, wall thickening
- DMSA: Renal cortical scarring, differential function
- MAG3/DTPA: Obstruction vs. dilatation, drainage curve
4. Imaging Summary Table
| Modality | Key Finding |
|---|---|
| USG | Thickened wall, PVR, hydronephrosis |
| VCUG | Christmas tree, VUR, DSD, large smooth bladder |
| Video-UDS | DLPP, compliance - gold standard |
| MRI spine | Underlying cause (tethered cord, SCI, MS) |
| DMSA | Renal scarring |
| CT | Calculi, complications |
5. Key Points
- Christmas tree bladder on VCUG = spastic/UMN neurogenic bladder
- Video-urodynamics is the gold standard - DLPP >40 cmH₂O = upper tract danger
- USG = first-line and serial surveillance modality
- MRI spine identifies the underlying neurological cause
- Primary radiological goal: detect and prevent upper tract damage
Sources: Smith & Tanagho's General Urology 19e; Campbell-Walsh-Wein Urology; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.