Anatomy of pancreas
Reading File
Finding Sources
Searching Images
pancreas anatomy diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive information. Let me compile the full anatomy of the pancreas.
Anatomy of the Pancreas
Overview
The pancreas is a soft, tan-colored retroperitoneal organ serving both exocrine and endocrine functions. It lies deep in the upper retroperitoneum, posterior to the stomach and transverse colon, and anterior to the great vessels of the abdomen.
Gross Anatomy: Parts of the Pancreas
The pancreas is classically divided into four parts:
1. Head
- The broadest part, nestled in the concavity of the duodenal C-loop (2nd and 3rd portions of the duodenum)
- Contains the common bile duct (CBD) in a groove or tunnel posteriorly
- The uncinate process is a hook-like inferior projection of the head that passes posterior to the superior mesenteric vessels
- The CBD and main pancreatic duct join at the ampulla of Vater, opening at the major duodenal papilla
2. Neck
- The constricted portion (~2 cm), overlying the superior mesenteric vessels
- The superior mesenteric artery (SMA) and superior mesenteric vein (SMV) pass posterior to the neck
- The SMV joins the splenic vein behind the neck to form the portal vein — a critical surgical landmark
3. Body
- Extends to the left, lying behind the stomach
- Crosses the aorta, left adrenal gland, left kidney, and left renal vessels
4. Tail
- The narrow left end, which is intraperitoneal (within the splenorenal ligament)
- Passes anterior to the left kidney and adrenal gland
- Terminates near the hilum of the spleen
Embryology
The pancreas develops from two buds of the foregut endoderm, first visible at ~4 weeks of gestation:
- Ventral bud: Pdx1+/Sox17+ cells; rotates clockwise with the bile duct and duodenum. Gives rise to the head and uncinate process
- Dorsal bud: Grows more rapidly, gives rise to the body and tail
By the 7th week, the ventral bud rotates posterior to the duodenum and fuses with the dorsal bud. Failure of fusion → pancreas divisum; abnormal encirclement of the duodenum → annular pancreas.
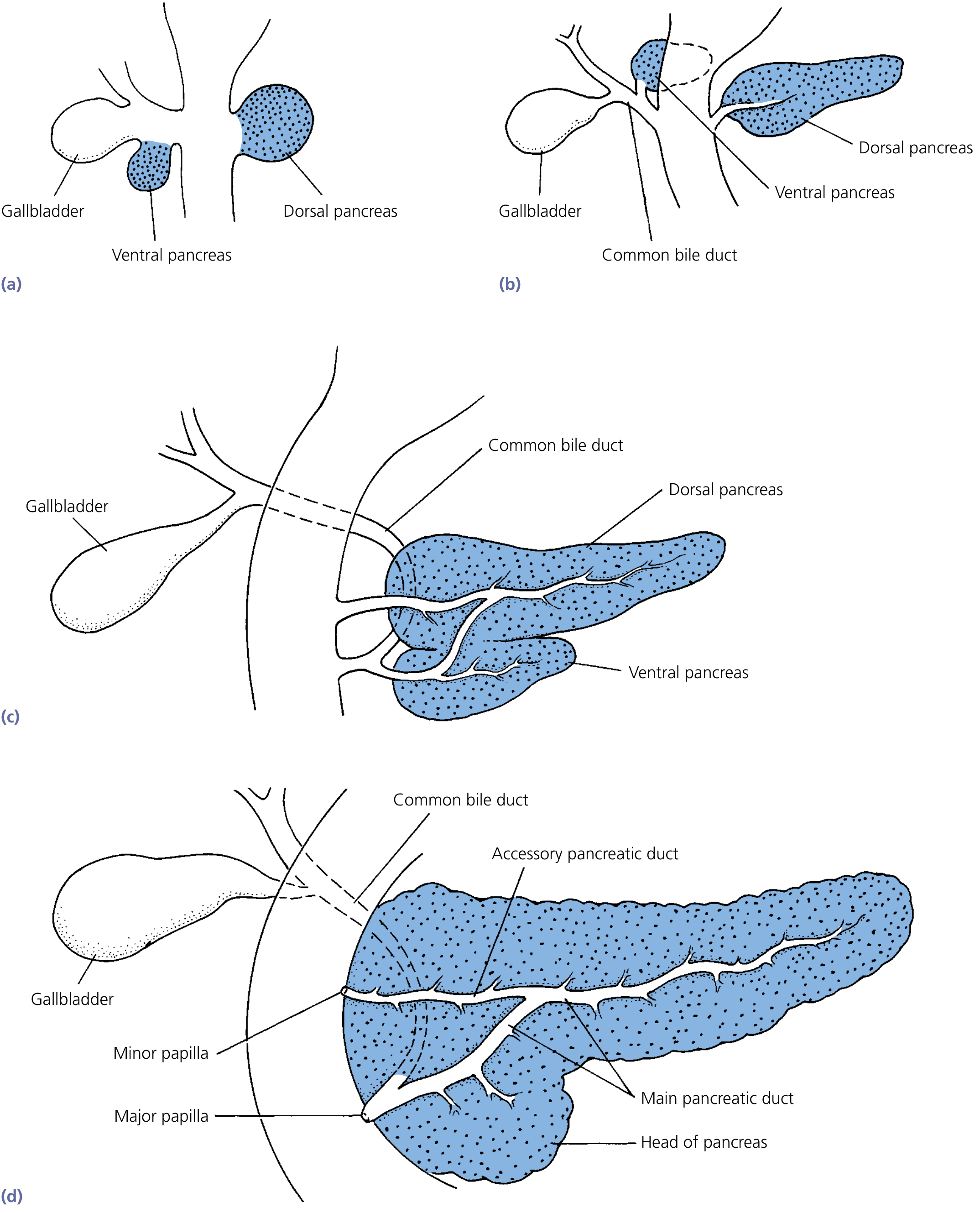
Embryological development of the pancreas — Yamada's Textbook of Gastroenterology
Ductal System
| Duct | Origin | Drainage |
|---|---|---|
| Main pancreatic duct (Wirsung) | Tail → head | Joins CBD → major papilla (ampulla of Vater) |
| Accessory duct (Santorini) | Drains upper head/neck | Opens at minor papilla (~2 cm proximal to major) |
In most people, the main duct drains the majority of the gland. In pancreas divisum (the most common congenital anomaly, ~10% of population), the dorsal duct (Santorini) does not fuse with the ventral duct — most of the gland drains through the small minor papilla.
Blood Supply
Arterial Supply
The pancreas has a dual arterial supply:
Head (shared with duodenum):
- Anterior and posterior pancreaticoduodenal arcades — formed by anastomoses between:
- Anterior/posterior superior pancreaticoduodenal arteries (from gastroduodenal artery → common hepatic artery → celiac axis)
- Anterior/posterior inferior pancreaticoduodenal arteries (from superior mesenteric artery)
- This shared supply means that pancreaticoduodenal arcade ligation can compromise duodenal viability
Body and Tail:
- Splenic artery (largest branch of the celiac axis, 5–11 mm diameter) — courses along the upper border of the pancreas with characteristic tortuosity, giving multiple branches to the neck, body, and tail
Venous Drainage
- Follows the arterial pattern; all blood drains ultimately into the portal vein
- The portal vein forms behind the neck of the pancreas (SMV + splenic vein junction)
- This intimate relationship makes portal vein involvement a key concern in pancreatic surgery
Relations and Posterior Surface
| Structure | Relation |
|---|---|
| Stomach | Anterior to body/tail |
| Duodenum (C-loop) | Surrounds the head |
| Common bile duct | Passes through/behind the head |
| Superior mesenteric vessels | Posterior to the neck |
| Portal vein | Formed behind the neck |
| Aorta, IVC | Posterior to the head |
| Left kidney and adrenal | Posterior to body/tail |
| Spleen | Adjacent to the tail |
| Celiac axis, common hepatic artery | Superior relations |
Lymphatic Drainage
Lymphatics follow major vascular routes along several systems:
- Splenic nodes (body/tail)
- Hepatic nodes (head)
- Superior mesenteric nodes (uncinate/inferior head)
- Aortocaval and posterior abdominal wall lymphatics
This multi-directional drainage explains the early lymphatic spread of pancreatic carcinoma.
Innervation
- Pancreatic nerve plexus originates from the celiac plexus
- Controls both endocrine and exocrine function
- Rich afferent pain fibers travel through the celiac plexus — the basis for celiac plexus neurolysis in pancreatic cancer pain management
Histology / Microanatomy
The pancreas contains two functionally distinct compartments:
Exocrine Pancreas (~90–95% of mass)
- Acinar cells: Produce and secrete digestive enzymes (amylase, lipase, proteases) stored as zymogen granules
- Centroacinar and ductal cells: Secrete sodium bicarbonate solution that neutralizes gastric acid in the duodenum
- Organized into lobules separated by connective tissue septa
Endocrine Pancreas (1–2% of mass, ~15% of blood flow)
- Islets of Langerhans: 1–2 million islets distributed throughout the gland; each ~0.3 mm in diameter, organized around capillaries
| Cell Type | % of Islet | Hormone | Function |
|---|---|---|---|
| Beta (β) cells | ~60% | Insulin + Amylin (IAPP) | Glucose uptake, anabolic; in center of islet |
| Alpha (α) cells | ~25% | Glucagon | Gluconeogenesis, glycogenolysis |
| Delta (δ) cells | ~10% | Somatostatin | Inhibits insulin and glucagon secretion |
| PP cells | Small number | Pancreatic polypeptide | Inhibits exocrine secretion |
Paracrine interactions are important: insulin inhibits glucagon secretion; somatostatin inhibits both insulin and glucagon; amylin inhibits insulin secretion.
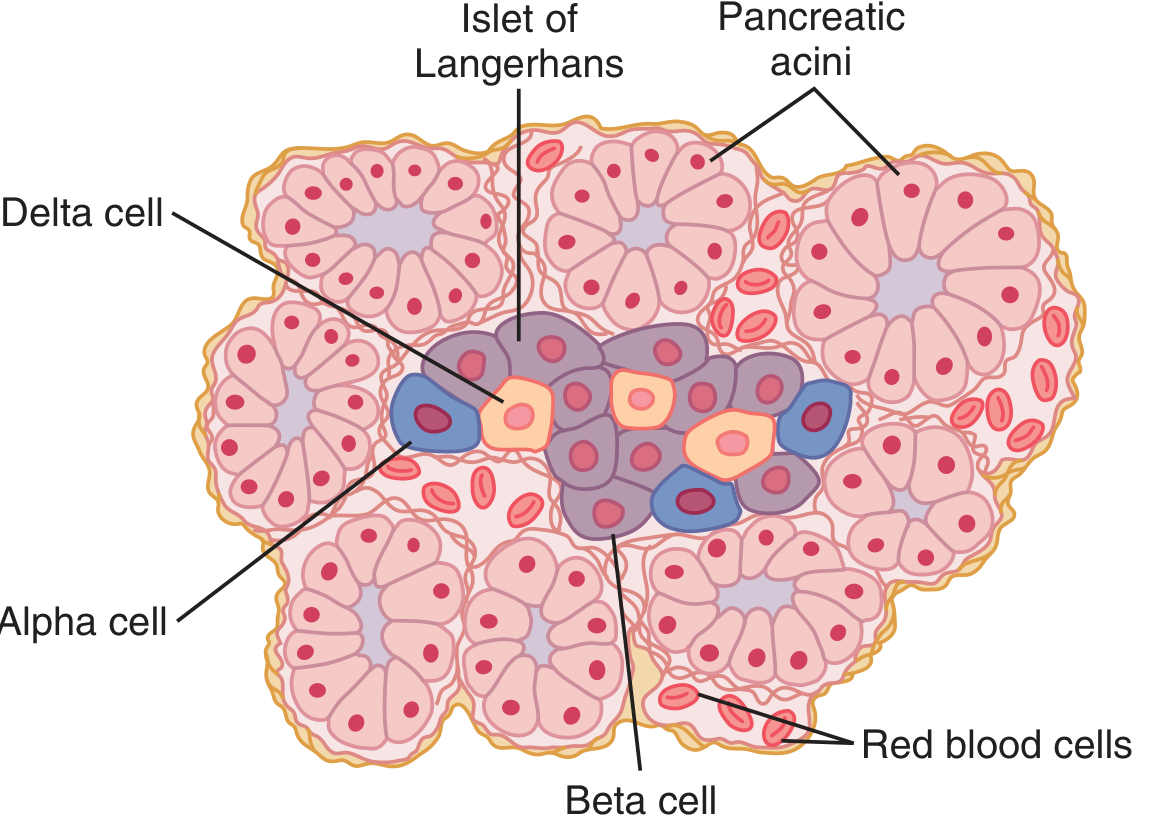
Islet of Langerhans — Guyton & Hall Textbook of Medical Physiology
Key Surgical Landmarks
- Portal vein formation behind the neck of the pancreas — the critical plane in pancreaticoduodenectomy (Whipple procedure)
- SMA posterior to the neck — its involvement defines unresectability in pancreatic cancer
- CBD within the head — obstructed by head tumors, causing painless jaundice
- Shared pancreaticoduodenal blood supply — extensive arterial ligation risks duodenal ischemia
Sources:
- Yamada's Textbook of Gastroenterology, 7e — Ch. 7: Pancreas: Anatomy and Structural Anomalies
- Mulholland & Greenfield's Surgery, 7e — Ch. 52: Pancreas Anatomy and Physiology
- Guyton & Hall Textbook of Medical Physiology — Ch. 79: Physiological Anatomy of the Pancreas
This is a shared conversation. Sign in to Orris to start your own chat.