Hormone replacement therapy in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hormone replacement therapy" AND menopause
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich, comprehensive information from multiple authoritative textbooks plus recent PubMed evidence. Here is the complete detailed answer:
Hormone Replacement Therapy (HRT) - Comprehensive Overview
1. Definition and Background
Hormone replacement therapy (HRT) - now more precisely termed menopausal hormone therapy (MHT) - refers to the administration of exogenous hormones (primarily estrogen, with or without a progestogen) to compensate for the decline in endogenous hormone production that occurs at menopause.
Menopause is defined as the cessation of menses for 12 consecutive months after age 40 in the absence of other causes of amenorrhea. The mean age at menopause is approximately 51.5 years, though significant hormonal changes begin earlier - FSH levels start rising as early as age 35. During menopause, estradiol falls to <30 pg/mL and progesterone to <1 ng/mL, both below the lowest levels seen during a normal menstrual cycle in younger women.
- Medical Physiology (Boron & Boulpaep), p. 1185
2. Hormones Used
Estrogens
| Preparation | Notes |
|---|---|
| Estradiol (oral, transdermal, topical, vaginal) | Most potent natural estrogen; principal estrogen in premenopausal women |
| Conjugated equine estrogens (CEE) | From urine of pregnant mares; primarily sulfate esters of estrone and equilin; widely studied (WHI trials) |
| Estrone-based (esterified estrogens, estropipate) | Oral preparations |
| Ethinyl estradiol | Synthetic; used mainly in contraceptives, less in HRT due to higher potency |
| Estriol | Weaker; found mainly in vaginal preparations |
Key point: Estradiol used in HRT is substantially lower in potency than estrogens in oral contraceptives, so adverse effects are generally less pronounced.
Progestogens
Added to protect the endometrium from estrogen-stimulated hyperplasia and carcinoma in women with an intact uterus. Women who have undergone hysterectomy may use estrogen alone.
| Agent | Type |
|---|---|
| Medroxyprogesterone acetate (MPA) | Synthetic progestin (most studied in WHI) |
| Norethindrone | Synthetic progestin |
| Micronized progesterone (Prometrium) | Bioidentical; may have a more favorable cardiovascular and breast profile |
| Levonorgestrel (IUD) | Local endometrial protection |
- Lippincott Illustrated Reviews: Pharmacology, p. 833
3. Mechanism of Action
Estradiol dissociates from its carrier proteins (SHBG, albumin) in plasma, diffuses across the cell membrane, and binds with high affinity to intranuclear estrogen receptors (ERα and ERβ). The activated hormone-receptor complex dimerizes, binds to estrogen response elements (EREs) on DNA, recruits coactivator proteins and the basal transcription complex, and drives RNA polymerase II-mediated transcription of specific target genes. The result is synthesis of proteins that mediate the multiple physiologic effects of estrogen.
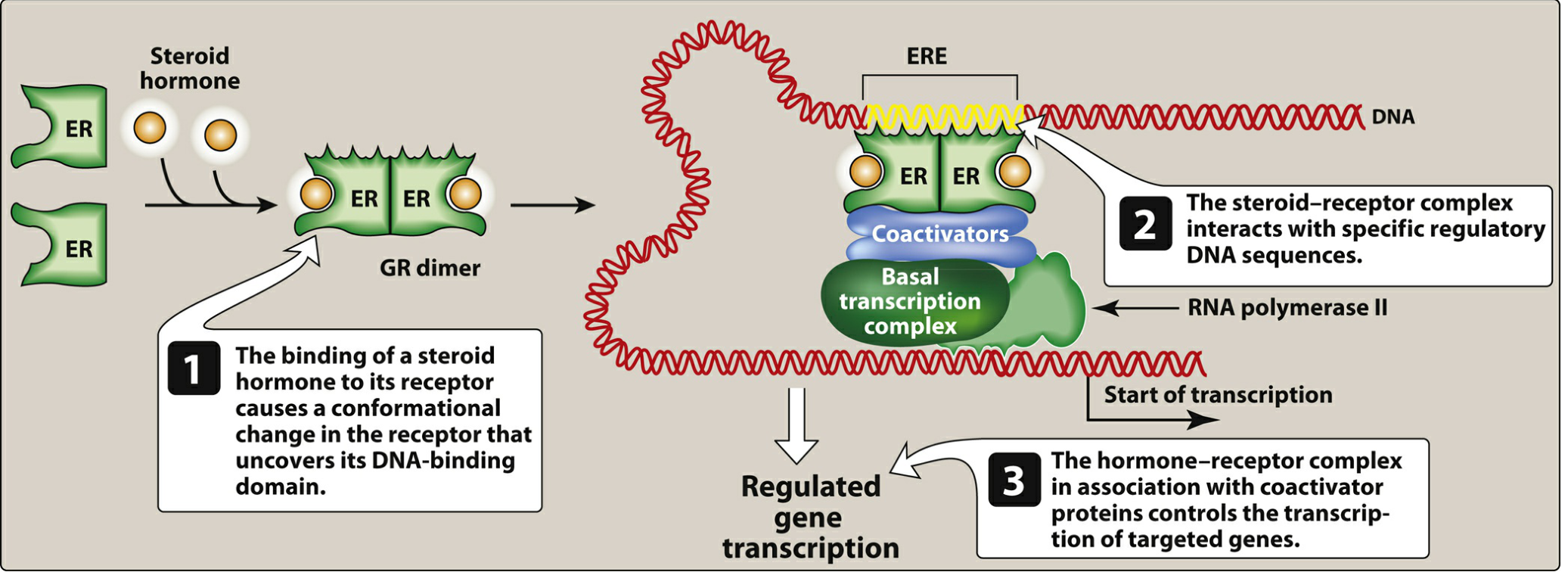
- Lippincott Illustrated Reviews: Pharmacology, p. 832
4. Routes of Administration
| Route | Examples | Notes |
|---|---|---|
| Oral | CEE, estradiol valerate, estradiol tablets | Convenient; undergoes first-pass hepatic metabolism → increases hepatic proteins (clotting factors, SHBG, CRP) |
| Transdermal patch | Estradiol patches | Bypasses first-pass metabolism; lower VTE and stroke risk than oral |
| Transdermal gel/spray | Estradiol gel | Similar advantages to patch |
| Vaginal cream | Estrogen cream | Primarily local effect; low systemic absorption with low-dose formulations |
| Vaginal ring | Low-dose: local effect; higher-dose rings may require progestogen | |
| Vaginal insert/tablet | Localized urogenital atrophy treatment | |
| Subcutaneous implant | Estradiol pellets | Less common; prolonged release |
For localized urogenital symptoms only (vaginal atrophy, dyspareunia), vaginal formulations are preferred to minimize systemic risks.
5. Indications
Primary Indication
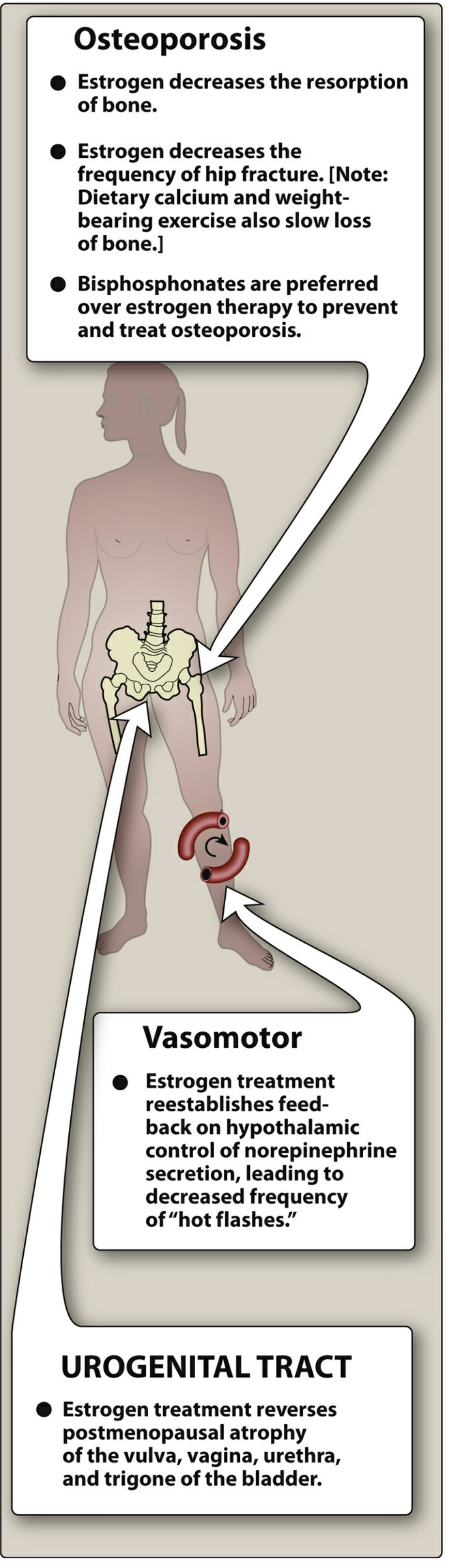
- Vasomotor symptoms (hot flashes/flushes, night sweats) - the most effective treatment available. Estrogen treatment reestablishes negative feedback on hypothalamic control of norepinephrine secretion, reducing the frequency and severity of hot flashes.
Other Indications
- Genitourinary syndrome of menopause (GSM): vaginal atrophy, dryness, dyspareunia, recurrent UTIs, urgency
- Premature ovarian insufficiency (POI) / surgical menopause before age 40-45: HRT is strongly indicated to replace hormones until the natural age of menopause; risk-benefit ratio is more favorable
- Prevention of osteoporosis: reduces bone resorption and fracture risk (hip, vertebral); however, bisphosphonates are now preferred as first-line; HRT may be considered in women with coexisting severe vasomotor symptoms
- Mood/psychological symptoms during perimenopause: improved mood, sexual function
- Female hypogonadism/Turner syndrome/gonadal dysgenesis: HRT for feminization and maintenance of secondary sexual characteristics
- Lippincott Illustrated Reviews: Pharmacology, p. 833-834
- Guyton & Hall Medical Physiology, p. 1028
6. Regimens
Combined HRT (Estrogen + Progestogen)
- Cyclic (sequential): Estrogen daily + progestogen for 12-14 days/month → scheduled withdrawal bleed
- Continuous combined: Estrogen + progestogen daily → aims for amenorrhea (common choice >12 months post-menopause; unexpected bleeding at any time warrants evaluation)
Estrogen-only HRT
- Women who have had a hysterectomy (no uterus = no endometrial cancer risk from unopposed estrogen)
Local (topical/vaginal) estrogen
- Low-dose; treats urogenital symptoms only; minimal systemic absorption with low-dose preparations; generally does not require progestogen
7. Benefits Summary
| Domain | Effect |
|---|---|
| Vasomotor symptoms | Highly effective (60-90% reduction in hot flash frequency) |
| Urogenital atrophy | Reverses atrophy of vulva, vagina, urethra, trigone |
| Bone density | Reduces bone resorption; reduces hip and vertebral fracture risk |
| Quality of life | Improved mood, sleep, sexual function |
| Colorectal cancer | WHI data: reduced risk with combined HRT |
| Possible cognitive benefit | Some data for initiation early in menopause ("timing hypothesis") |
A 2025 Lancet Healthy Longevity meta-analysis (PMID: 41448220) found that MHT is associated with a modest reduction in risk of mild cognitive impairment or dementia, particularly when initiated peri-menopausally.
8. Risks and Adverse Effects
Breast Cancer
- Combined estrogen + progestogen HRT (especially MPA) increases breast cancer risk with prolonged use (>5 years). The risk appears more modest with micronized progesterone and shorter durations of use. Estrogen-alone therapy (in hysterectomized women) has a less clear association - the WHI estrogen-alone arm actually showed a possible decrease in breast cancer incidence.
- Bailey & Love's Surgery, p. 1075
Cardiovascular Disease
- The Women's Health Initiative (WHI) trial was pivotal:
- CEE + MPA (combined arm): increased risk of MI and CVD events, especially in the first year of use; also increased risk of ischemic stroke
- CEE alone (hysterectomized women): neither increased nor decreased CVD risk; but increased stroke risk
- Younger women (50-59) with prior bilateral oophorectomy: a >30% reduction in all-cause mortality with CEE; older women did not see this benefit
- The KEEPS trial (Kronos Early Estrogen Prevention Study): starting HRT shortly after menopause does not reduce atherosclerotic progression or CVD outcomes, but does significantly improve vasomotor symptoms, mood, sexual function, and bone density - especially when started soon after menopause
- The "timing hypothesis" or "window of opportunity": HRT initiated before age 60 or within 10 years of menopause is more likely to have a neutral or favorable cardiovascular profile; initiating later (>10 years post-menopause) may worsen CVD
- Harrison's Principles of Internal Medicine 22e, p. 3208
A 2024 BMC Women's Health systematic review and meta-analysis (PMID: 38263123) confirmed the timing-dependent cardiovascular effects of HRT.
Venous Thromboembolism (VTE)
- Oral estrogen increases DVT and PE risk by increasing hepatic synthesis of procoagulant factors
- Transdermal estrogen carries a significantly lower (possibly negligible) VTE risk compared to oral - this is a key reason to prefer transdermal delivery in women at elevated VTE risk
- Coexisting thrombophilias (Factor V Leiden, antiphospholipid syndrome) further amplify VTE risk with oral HRT
- A 2025 Climacteric systematic review (PMID: 40488293) confirmed that transdermal HRT appears safer than oral in women at higher VTE risk.
Endometrial Cancer
- Unopposed estrogen significantly increases the risk of endometrial hyperplasia and carcinoma (relative risk 2-10x depending on duration and dose)
- Adding a progestogen (for at least 12-14 days/cycle) eliminates this excess risk
- Unexpected bleeding with continuous combined HRT or recurrence of bleeding after amenorrhea is established requires evaluation (endometrial biopsy/ultrasound)
Other Adverse Effects
- Breast tenderness, bloating, irregular uterine bleeding (especially in first 3-6 months)
- Nausea (oral preparations)
- Headache, mood changes
- Fluid retention
- Possible increased risk of gallbladder disease (oral route)
Absolute Contraindications
- Unexplained abnormal uterine bleeding
- Known or suspected estrogen-sensitive cancers (breast, endometrial)
- Active or recent thromboembolic disease (DVT, PE, stroke, MI)
- Active liver disease with impaired function
- Known thrombophilic disorders (relative; transdermal may be considered with specialist input)
- Pregnancy
9. The "Timing Hypothesis" (Window of Opportunity)
A core concept in modern HRT management: the risk-benefit profile varies substantially based on when HRT is initiated relative to menopause onset.
- Initiation before age 60 or within 10 years of menopause: Evidence suggests favorable or neutral cardiovascular effects; vasomotor, skeletal, and quality-of-life benefits predominate
- Initiation after age 60 or >10 years post-menopause: Cardiovascular and VTE risks increase; arterial plaques may already be established, and estrogen may destabilize rather than prevent atherosclerosis
- Guyton & Hall Medical Physiology, p. 1028
10. Special Populations
Premature Ovarian Insufficiency (POI, menopause before age 40)
- HRT is strongly recommended until at least age 51, regardless of VTE/breast cancer risk concerns applicable to older women - the risks of long-term estrogen deficiency (osteoporosis, CVD, cognitive decline) outweigh the risks of HRT in this group
Women with Hysterectomy
- Estrogen-only HRT preferred; no progestogen needed; slightly different risk profile (no endometrial cancer risk; possibly reduced breast cancer risk vs. combined HRT)
Surgical Menopause (bilateral oophorectomy)
- Acute, severe estrogen deficiency; HRT indication is strong especially before natural age of menopause
Breast Cancer Survivors
- HRT is generally contraindicated in hormone receptor-positive breast cancer survivors; non-hormonal alternatives for vasomotor symptoms are used (SSNRIs, gabapentin, clonidine)
11. Selective Estrogen Receptor Modulators (SERMs)
SERMs are structurally dissimilar compounds that act as estrogen agonists in some tissues and antagonists in others - their effects depend on the target tissue and the individual's hormonal status.
| SERM | Agonist in | Antagonist in | Main Use |
|---|---|---|---|
| Raloxifene | Bone, cardiovascular | Breast, uterus | Osteoporosis prevention; reduces breast cancer risk |
| Tamoxifen | Bone, uterus | Breast | Breast cancer treatment/prevention |
| Ospemifene | Vaginal epithelium | - | Genitourinary syndrome of menopause |
The ideal SERM for HRT would alleviate vasomotor symptoms, protect bone and the cardiovascular system, and protect against Alzheimer's disease - without estrogenic carcinogenic effects. No currently available SERM fully achieves this profile; bone benefits appear less significant with SERMs than with estrogen.
- Medical Physiology (Boron & Boulpaep), p. 1186
12. Non-Hormonal Alternatives for Vasomotor Symptoms
For women who cannot or do not wish to use HRT:
- SNRIs (venlafaxine, desvenlafaxine): first-line non-hormonal options
- SSRIs (paroxetine - FDA-approved for hot flashes as Brisdelle; escitalopram)
- Gabapentin/pregabalin: effective, especially for nocturnal symptoms
- Clonidine: modest efficacy; side effect profile limits use
- Oxybutynin: emerging evidence
- Fezolinetant (Veozah): NK3 receptor antagonist; FDA-approved 2023 specifically for vasomotor symptoms; non-hormonal; targets the hypothalamic KNDy neuron pathway directly
13. Current Recommendations
- Individualize therapy - no blanket for or against recommendation; risks and benefits differ based on age, time since menopause, type of menopause (natural vs. surgical), symptom severity, and personal risk factors
- Lowest effective dose for the shortest duration needed to control symptoms
- Prefer transdermal over oral estrogen in women with elevated VTE risk, hypertriglyceridemia, or history of migraine with aura
- Add progestogen in all women with an intact uterus
- Vaginal estrogen for isolated urogenital symptoms, with minimal systemic risk
- Annual review of continued need, dose, and route
- HRT is not routinely recommended for primary or secondary cardiovascular prevention
- Guyton & Hall Medical Physiology, p. 1028
- Lippincott Illustrated Reviews: Pharmacology, p. 833-834
- Harrison's Principles of Internal Medicine 22e, p. 3208
Recent Evidence Highlights (2024-2025)
| Study | Finding |
|---|---|
| Cognition meta-analysis, Front Endocrinol 2024 (PMID: 38501109) | Timing of HRT initiation relative to menopause affects cognitive outcomes; peri-menopausal initiation appears beneficial |
| Lancet Healthy Longevity 2025 (PMID: 41448220) | MHT associated with reduced risk of mild cognitive impairment/dementia |
| BMC Women's Health 2024 (PMID: 38263123) | Confirms cardiovascular risk depends heavily on age at initiation and type of HRT |
| Climacteric 2025 (PMID: 40488293) | Transdermal HRT is safer than oral for VTE risk in higher-risk women |
| Best Pract Res Clin Endocrinol Metab 2024 (PMID: 37634998) | Systematic review confirms progestogens (especially micronized progesterone) effectively protect endometrium with combined MHT |
Sources: Guyton & Hall Medical Physiology; Medical Physiology (Boron & Boulpaep); Lippincott Illustrated Reviews: Pharmacology; Harrison's Principles of Internal Medicine 22e; Goldman-Cecil Medicine; Bailey & Love's Short Practice of Surgery 28e; Miller's Review of Orthopaedics 9e
This is a shared conversation. Sign in to Orris to start your own chat.