Bartholin cyst
Reading File
Finding Sources
Searching PubMed
Bartholin cyst gland management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
Bartholin cyst abscess anatomy location vulva
Here is a comprehensive overview of Bartholin cyst (and abscess), drawn from multiple authoritative sources:
Bartholin Cyst (and Abscess)
Anatomy
The Bartholin glands (greater vestibular glands) are paired, pea-sized glands located in the labia minora. Their ducts drain into the posterior vestibule at the 4 o'clock and 8 o'clock positions. They begin functioning at puberty, providing moisture to the vestibule, and involute with age.
Pathophysiology
Cyst formation: When the duct becomes obstructed (by trauma, edema, or prior inflammation), secretions accumulate, forming a retention cyst. The cyst is typically lined by transitional or squamous epithelium. A cyst does not need to be present before an abscess can develop.
Abscess formation: If retained secretions become infected, an abscess forms. Abscesses can be quite large and cause extreme pain.
Common organisms:
- E. coli — most common isolate
- Polymicrobial (majority)
- Less common: N. gonorrhoeae, C. trachomatis
Clinical Features
| Feature | Cyst | Abscess |
|---|---|---|
| Pain | Mild or absent | Severe |
| Fluctuance | Present | Present + marked |
| Systemic symptoms | Rare | Rarely fever/chills |
| Erythema/induration | Minimal | Often present |
- Cysts range up to 3–5 cm in diameter
- Located at the posterior introitus near 4 or 8 o'clock
Histopathology
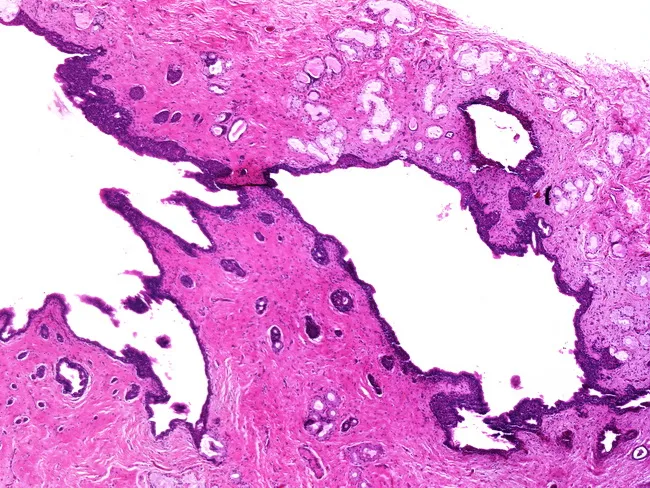
Histopathology: Bartholin gland cyst — dilated duct with mucous retention, lined by transitional/ductal-type epithelium within fibrous stroma. No dysplasia.
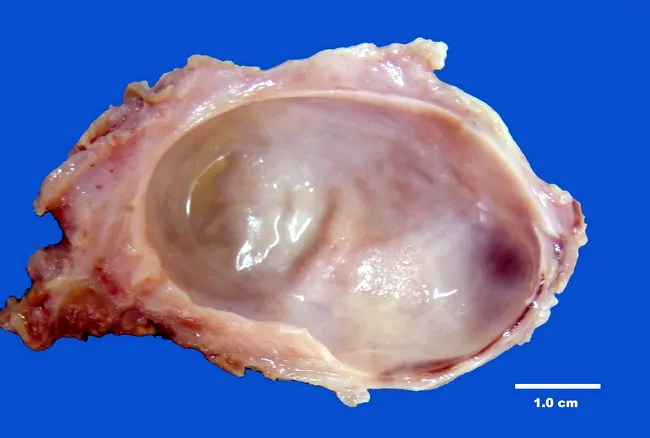
Gross specimen: unilocular cyst (5.5 × 4.0 × 3.0 cm), smooth tan-pink exterior, glistening inner lining, serous fluid.
Diagnosis
- Primarily clinical — unilateral posterior vulvar/vestibular mass near 4 or 8 o'clock
- Ultrasound can confirm a discrete fluid collection when the abscess is not clearly defined, and helps distinguish cyst from abscess or solid neoplasm

Ultrasound: hypoechoic well-circumscribed vulvar mass (~2.9 × 2.5 cm) with posterior acoustic enhancement — consistent with Bartholin cyst/abscess.
Important in women >40 years: Bartholin gland carcinoma is rare but must be excluded. Any atypical or solid/neoplastic-appearing epithelium in the cyst wall should prompt biopsy and pathologic evaluation.
Management
Conservative (small, asymptomatic cyst): Observation, warm sitz baths.
Definitive drainage options:
1. Word Catheter Placement (first-line, office-based)
- Patient in dorsal lithotomy position
- Local anesthesia: 2–4 mL of 1% lidocaine injected into the mucosal surface
- Stab incision with #11 scalpel on the mucosal surface of the vestibule, just lateral to the hymenal ring, at the point of greatest fluctuation — incision only a few mm (too large = catheter displacement)
- Drain contents; send fluid for culture
- Insert Word catheter (similar to #10 Foley, 1-inch stem, inflatable balloon) into the incision; inflate balloon with 2–4 mL of water/saline
- Tuck catheter end into the vagina for comfort
- Leave in place 4–6 weeks to allow epithelialization of a new drainage tract
Common errors with Word catheter:
- Stab wound too large → catheter falls out early
- Releasing syringe pressure after filling balloon → balloon deflates, catheter falls out prematurely
- Placing balloon outside true cyst cavity → significant pain
2. Marsupialization (definitive surgical option)
- Dorsal lithotomy; local anesthetic (2% lidocaine with epinephrine) or pudendal block
- Fusiform longitudinal incision 1–2 cm wide over the cyst wall, internal to the hymenal ring
- Excise the mucosa overlying the cyst; grasp cyst wall with hemostats before segment removal
- Irrigate cavity with normal saline
- Suture cyst wall edge to adjacent vaginal mucosal edge using 4-0 Vicryl interrupted sutures — intent is to suture the cavity open permanently
- Post-op: daily sitz baths × 3–4 days; follow-up at 1 week to verify patency
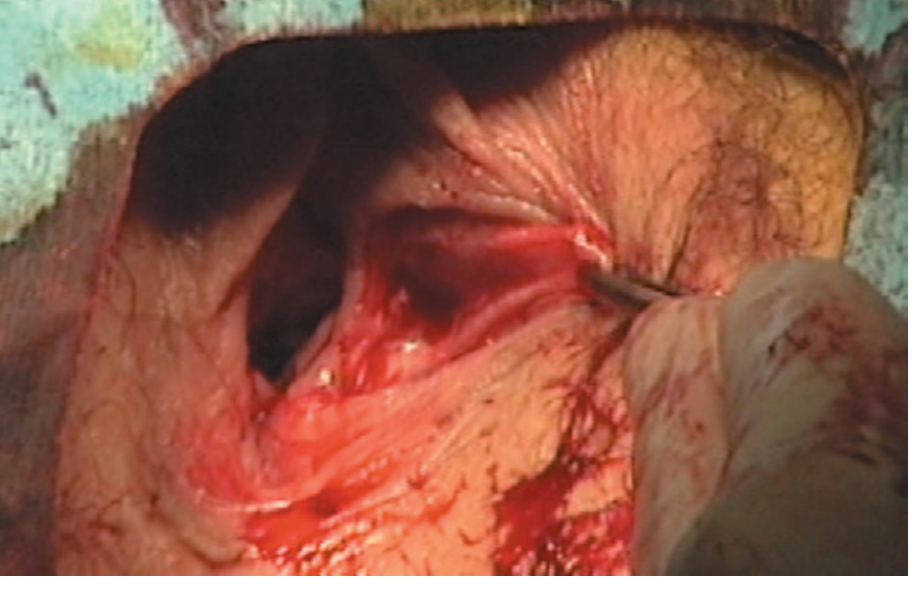
Intraoperative: Bartholin cyst opened with roof removed.
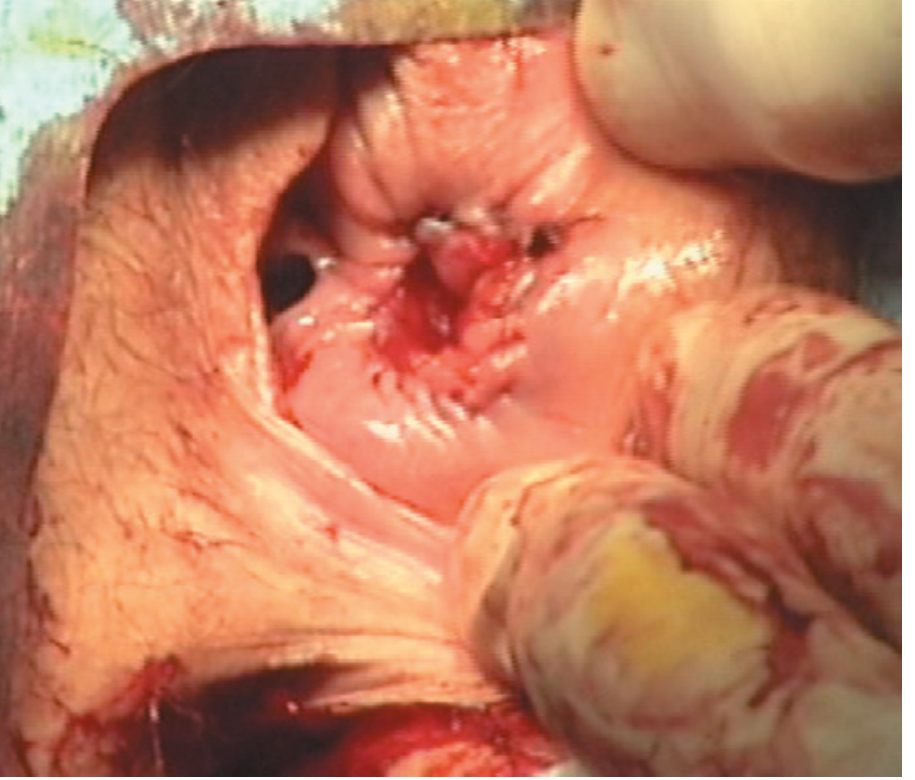
Marsupialization complete — cyst wall sutured open to vaginal mucosa.
3. Gland Excision
Reserved for recurrent cases or strong suspicion of malignancy (particularly in postmenopausal women).
Antibiotics
- Not routinely needed for simple drainage
- Indicated if surrounding cellulitis, pregnancy, diabetes, or immunocompromise
- If N. gonorrhoeae / C. trachomatis suspected, treat accordingly
Key Comparison: Cyst vs. Abscess
| Bartholin Cyst | Bartholin Abscess | |
|---|---|---|
| Contents | Mucoid/serous secretion | Pus |
| Timing | Chronic, gradual | Acute, days |
| Pain | Mild | Severe |
| Treatment | Word catheter / marsupialization | I&D + Word catheter / marsupialization |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 916 · Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. · Textbook of Family Medicine, 9th ed., p. 767 · Tintinalli's Emergency Medicine: A Comprehensive Study, p. 695
Bartholin cyst removal
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.