Lap appendicectomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content for a thorough response. Let me compile the full answer.
Laparoscopic Appendicectomy
Source: Bailey and Love's Short Practice of Surgery, 28th Edition
Overview
Laparoscopy has two roles in suspected appendicitis: diagnostic and therapeutic. Its diagnostic value is particularly important in women of childbearing age, where gynaecological pathology can mimic appendicitis closely.
Port Placement and Patient Positioning
The standard setup involves 3 ports:
| Port | Site | Function |
|---|---|---|
| 1st | Infraumbilical (open technique) | Camera port |
| 2nd | Suprapubic | Working port |
| 3rd | Left lower quadrant | Working port |
- Pneumoperitoneum is established using the open (Hasson) infraumbilical approach
- Port placement may vary with operator preference and previous abdominal scars
- Moderate Trendelenburg tilt with the right side of the table elevated improves exposure and assists delivery of small bowel loops from the pelvis
Surgical Steps
1. Identify the appendix
The appendix is located in the conventional manner by identifying the caecal taeniae and tracing them to their confluence. A laparoscopic tissue-holding forceps is used to control it.
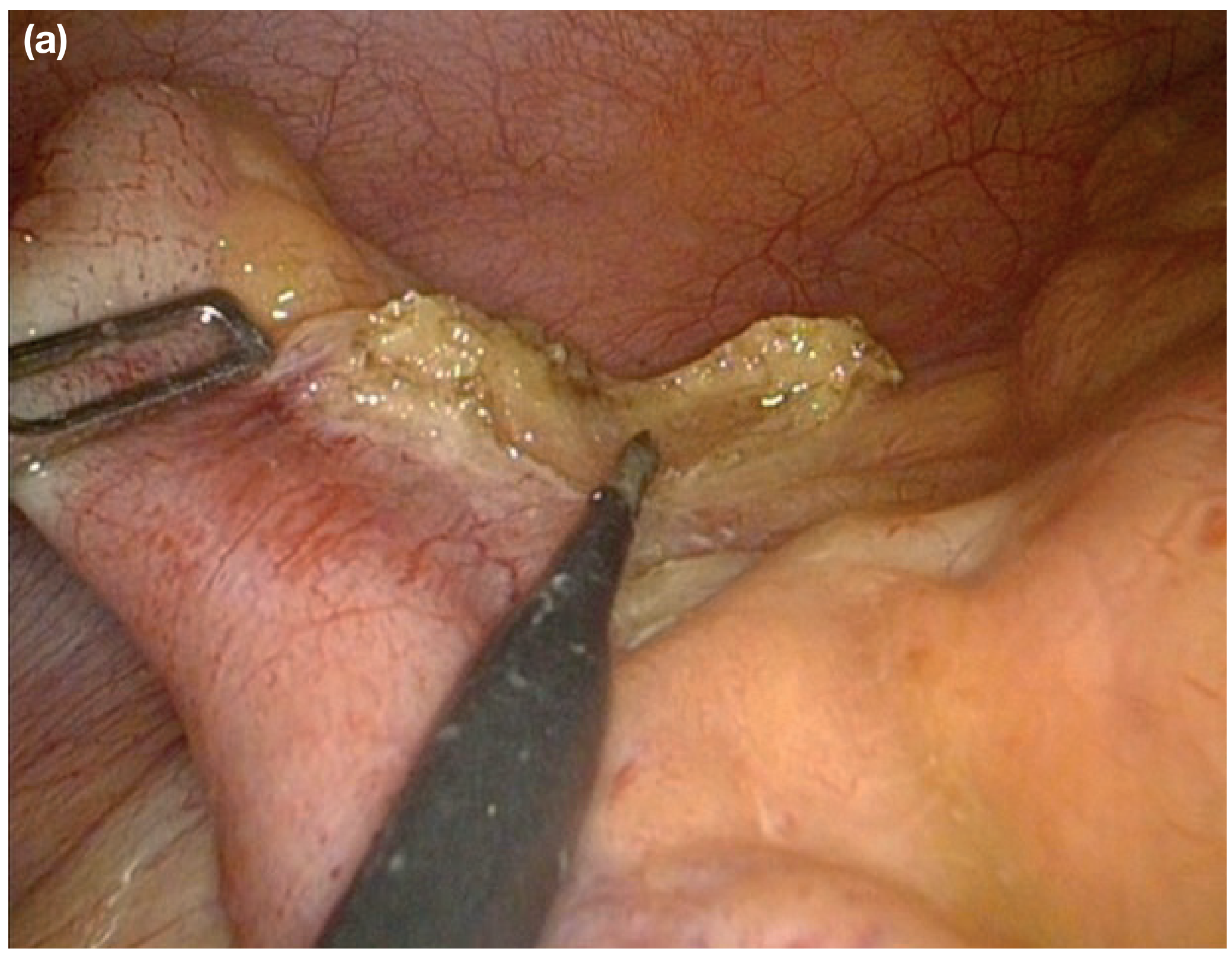
2. Expose the mesoappendix
By elevating the appendix, the mesoappendix is displayed. Peritoneal attachments may need division to adequately mobilise the caecum.
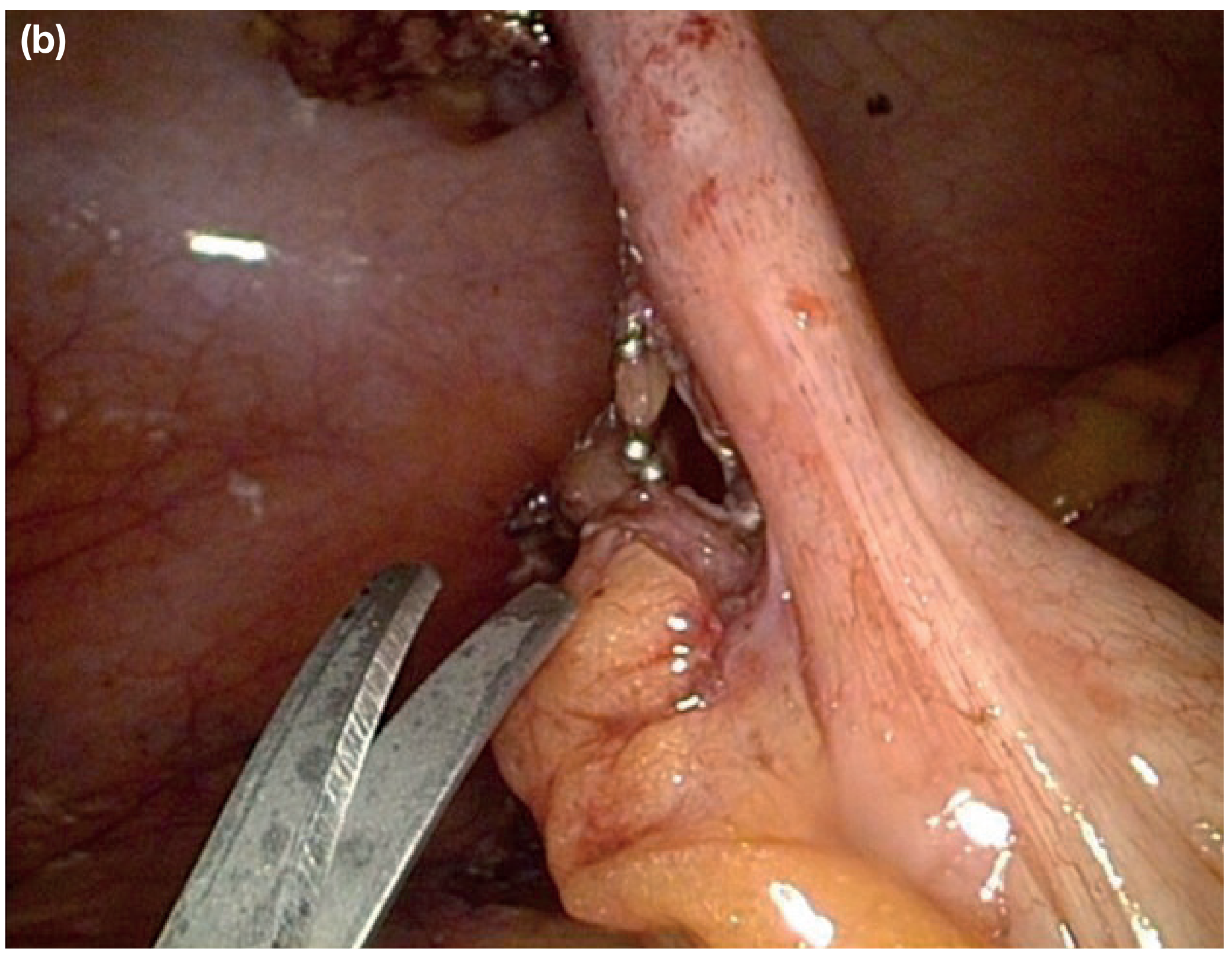
3. Dissect and ligate the appendicular vessels
A dissecting forceps, hook diathermy, or scissors diathermy dissects through the mesoappendix and exposes the appendicular vessels, which are then:
- Coagulated, or
- Ligated with a clip applicator
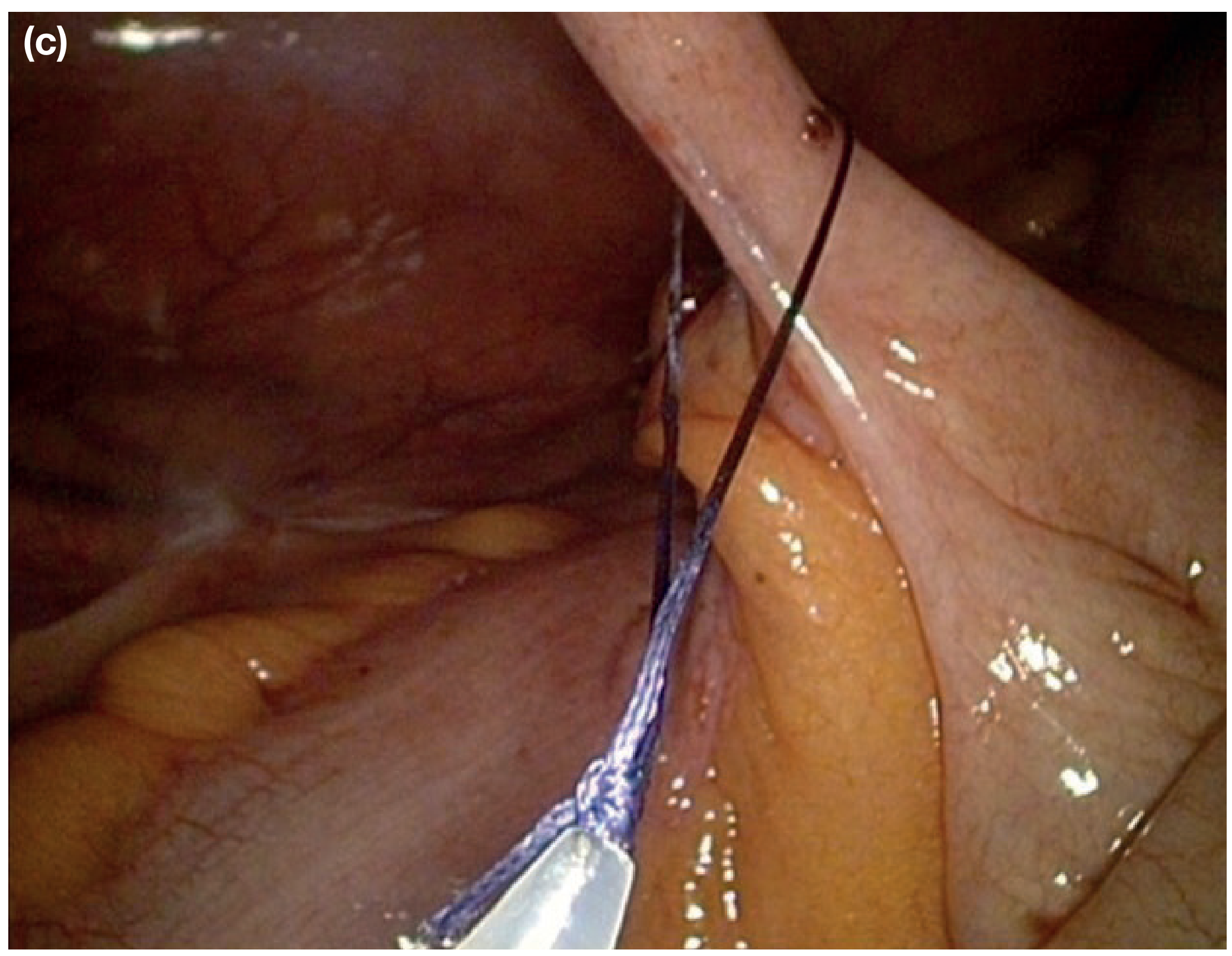
4. Ligate and divide the appendix base
The appendix, free of its mesentery, is ligated at its base with either:
- An absorbable loop ligature (Roeder loop / Endoloop), or
- A linear stapling device
The stump is NOT routinely invaginated (unlike open technique).
5. Specimen retrieval
The divided appendix is placed in a specimen bag and removed through one of the operating ports to avoid port-site contamination.

6. Closure
- Fascia closed with absorbable sutures at umbilical port and any port site >5 mm
- Skin incisions closed with subcuticular sutures
Intraoperative Problems
| Problem | Management |
|---|---|
| Normal appendix found | Remove it anyway (to avoid future diagnostic confusion) if a skin crease/gridiron incision has been made; may preserve if diagnostic laparoscopy only, though ~25% of macroscopically normal appendices have microscopic inflammation |
| Cannot find appendix | Trace caecal taeniae to their confluence before diagnosing absent appendix |
| Appendix mass / pericaecal phlegmon | Safer to abandon procedure; drain any abscess, give IV antibiotics, monitor carefully |
| Gangrenous base | Do not attempt ligation; place stitches through healthy caecal wall and amputate flush, or use linear stapler across healthy caecum |
| Crohn's disease at ileocaecal region | If caecal wall at base is healthy, appendicectomy is safe; if appendix itself involved, consider IV corticosteroids and antibiotics |
Special Situations
Appendicitis in Pregnancy
- Most common extrauterine acute abdominal condition in pregnancy (0.5-1 per 1000 pregnancies)
- Slightly more common in second trimester; presentation is more likely to be complicated
- Fetal loss: 3-5% with acute appendicitis; rises to >20% with perforation
- Negative appendicectomy carries: fetal loss 4%, preterm labour 10%
- Laparoscopic approach is now considered safe in any trimester - use open Hasson technique for initial access
- If fetus is at viable gestational age (≥23 weeks), appropriate obstetric/neonatal support should be available
Postoperative Complications
Early Complications
Wound infection (most common - 5-10% of patients)
- Presents day 4-5 with pain and erythema, often after hospital discharge
- Organisms: mixed Gram-negative bacilli + anaerobes (Bacteroides, anaerobic streptococci)
- Treatment: wound drainage ± antibiotics
Intra-abdominal abscess (~8%)
- Spiking fever, malaise, anorexia at 5-7 days post-op
- Sites: interloop, paracolic, pelvic, subphrenic
- Diagnosis: USS or CT; treatment: percutaneous drainage
- Surgical exploration if imaging negative but sepsis ongoing (especially with ileus)
Ileus
- Expected after gangrenous appendix removal
- If persisting >4-5 days with fever - suggests ongoing sepsis, investigate further
- Richter hernia at port site can mimic ileus - CT is diagnostic
Respiratory - rare without concurrent pulmonary disease; prevent with analgesia and physiotherapy
VTE - rare; assess preoperatively and use appropriate prophylaxis
Serious / Rare Complications
| Complication | Key Points |
|---|---|
| Portal pyaemia (pylephlebitis) | Septicaemia in portal venous system → multiple intrahepatic abscesses; high fever, rigors, jaundice; treat with systemic antibiotics + percutaneous drainage |
| Faecal fistula | Leakage from appendix stump; follows deep encircling stitch, caecal wall oedema/inflammation, or Crohn's disease |
| Adhesive intestinal obstruction | Most common LATE complication; usually a single band adhesion; laparoscopic lysis is effective |
Checklist for Unwell Patient Post-Appendicectomy
- Wound / abdomen - abscess?
- Rectum - pelvic abscess?
- Lungs - pneumonitis/collapse?
- Legs - DVT?
- Eyes/liver - pyelophlebitis (jaundice, rigors)?
- Urine - pyelonephritis?
- Subphrenic abscess?
Advantages of Laparoscopic over Open Appendicectomy
- Superior diagnostic value (especially in women of childbearing age)
- Lower wound infection rates
- Shorter hospital stay and faster return to activity
- Better cosmesis
- Allows inspection of entire peritoneal cavity
Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 76 (pp. 1367-1370)
This is a shared conversation. Sign in to Orris to start your own chat.