Muscarinic receptors full details for md exam answer to fetch 10/10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I have all the data I need. Let me now compose the comprehensive, exam-grade answer.
Muscarinic Receptors - Complete MD Exam Answer
1. Introduction
Muscarinic receptors are G protein-coupled receptors (GPCRs) named after the alkaloid muscarine (from Amanita muscaria mushroom), which selectively activates them. They mediate the actions of acetylcholine (ACh) at parasympathetic neuroeffector junctions and in the CNS. They are pharmacologically distinct from nicotinic receptors (which are ligand-gated ion channels).
- Natural ligand: Acetylcholine (rapidly hydrolyzed by AChE and BuChE)
- Structure: 7-transmembrane (TM) domain GPCRs
- Subtypes: Five cloned subtypes: M1 - M5
2. Structural Features
All five muscarinic receptor subtypes share:
- Seven transmembrane (TM) helices (classic GPCR architecture)
- A highly conserved orthosteric (classical) binding site buried deeply within the TM domain
- Key interactions: charge-charge between the quaternary N of ACh and a TM3 aspartate residue; hydrogen bond with a TM6 asparagine (unique to muscarinic receptors among biogenic amine GPCRs)
- Allosteric binding sites on extracellular loops (ECL2, ECL3) - these vary among subtypes, enabling subtype-selective modulators (PAMs/NAMs)
(Goodman & Gilman's, p. 227)
3. Subtypes, Location, G-Protein Coupling & Second Messengers
This is the single most important table for the exam:
| Subtype | G-Protein | 2nd Messenger | Key Locations | Selective Antagonist |
|---|---|---|---|---|
| M1 | Gq/11 | ↑PLC → ↑IP3 → ↑[Ca²⁺]i; ↑DAG → ↑PKC | Cerebral cortex, hippocampus, striatum, autonomic ganglia, gastric parietal cells | Pirenzepine |
| M2 | Gi/o | ↓Adenylyl cyclase → ↓cAMP → ↓PKA; opens GIRK K⁺ channels | Heart (SA node, AV node), presynaptic nerve terminals (autoreceptor) | Gallamine, AF-DX 116 |
| M3 | Gq/11 | ↑PLC → ↑IP3 → ↑[Ca²⁺]i → ↑eNOS → ↑NO | Exocrine glands (salivary, lacrimal, bronchial, sweat), smooth muscle (bladder, bronchi, GI), vascular endothelium, eye (iris sphincter, ciliary) | Darifenacin, solifenacin, 4-DAMP |
| M4 | Gi/o | ↓Adenylyl cyclase → ↓cAMP | Striatum, CNS (modulates dopamine), presynaptic (brain) | Tropicamide (weak) |
| M5 | Gq/11 | ↑PLC → ↑IP3 | Substantia nigra, dopaminergic neurons, cerebral vessels | None clinically |
Mnemonic: "Odd = Gq (1,3,5); Even = Gi (2,4)"
4. Signal Transduction - The Two Pathways
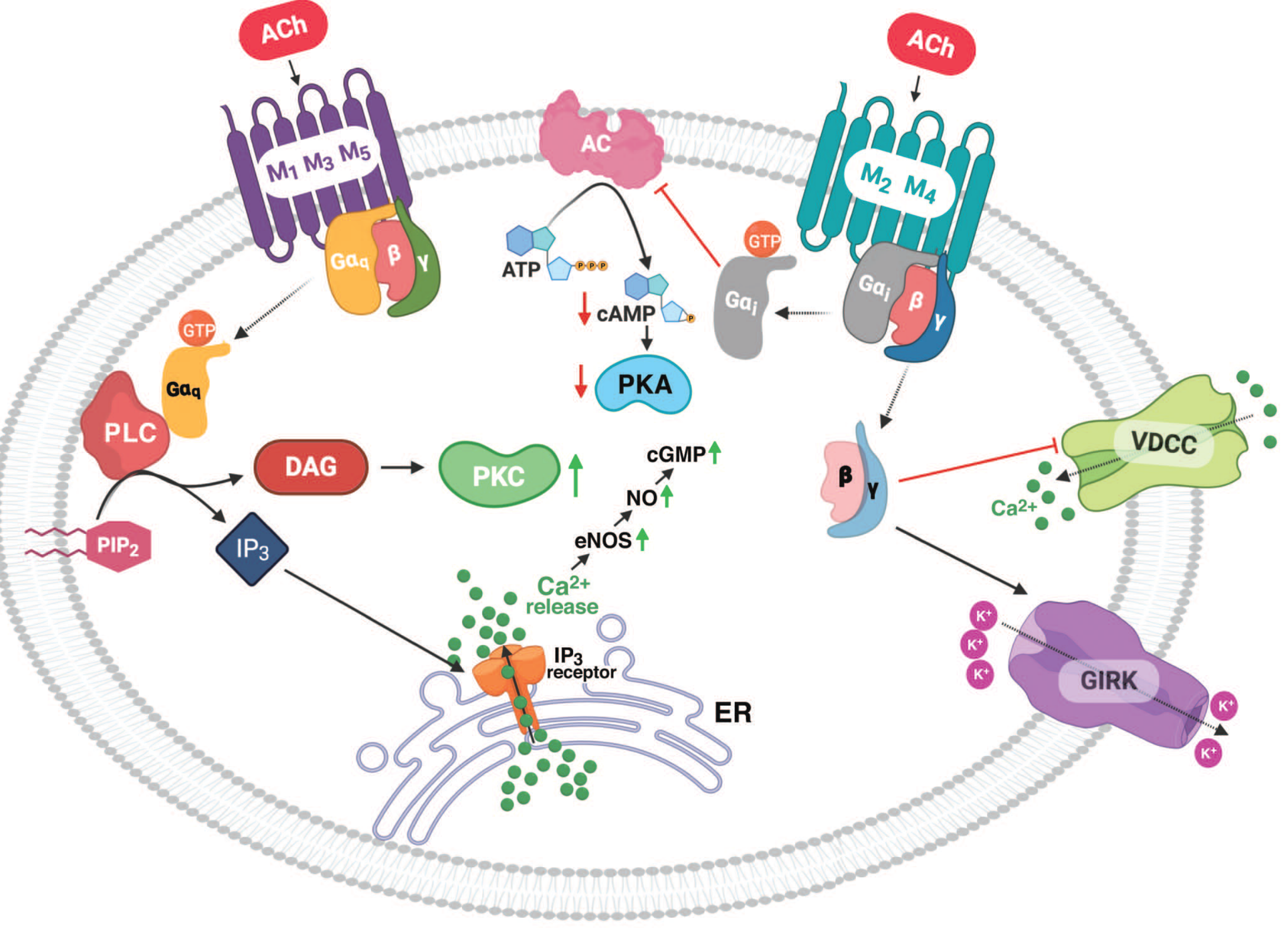
Gq pathway (M1, M3, M5):
Receptor → Gq/11 → Phospholipase C (PLC) → PIP2 hydrolysis → IP3 + DAG
- IP3 → ER Ca²⁺ release → smooth muscle contraction, glandular secretion
- DAG → Protein Kinase C activation
- In vascular endothelium: Ca²⁺-calmodulin → eNOS activation → NO → cGMP → vasodilation
Gi/o pathway (M2, M4):
Receptor → Gi/o → Inhibits adenylyl cyclase → ↓cAMP → ↓PKA
- Gβγ subunit → opens GIRK (G protein-coupled inwardly-rectifying K⁺) channels → K⁺ efflux → hyperpolarization
- Gβγ → inhibits voltage-dependent Ca²⁺ channels (VDCC)
- Net cardiac effect: ↓heart rate, ↓conduction velocity
(Goodman & Gilman's, Fig. 11-1)
5. Organ-by-Organ Pharmacological Effects
Heart (M2 dominant)
- SA node: ↓automaticity → negative chronotropic effect (bradycardia)
- Mechanism: ↓HCN channel activity (↓If pacemaker current); ↑IK-ACh (K⁺ efflux → hyperpolarization)
- AV node: ↓conduction velocity → negative dromotropic effect (↑PR interval; can cause AV block)
- Atria: ↓contractility (negative inotropic effect)
- Ventricles: less affected (fewer M2 receptors)
- Presynaptic M2: autoreceptors on vagal terminals, inhibit ACh release (feedback)
Blood Vessels (M3 on endothelium)
- ACh → M3 on endothelial cells → ↑IP3 → ↑Ca²⁺ → eNOS → NO production → vasodilation
- Note: If endothelium is damaged, ACh paradoxically causes vasoconstriction (direct M3 on vascular smooth muscle)
Respiratory (M3 on bronchial smooth muscle + glands)
- Bronchoconstriction (↑IP3 → smooth muscle contraction)
- ↑Bronchial secretion
- M1 on parasympathetic ganglia facilitates ganglionic transmission
Eye (M3)
- Pupillary sphincter (iris): M3 → contraction → miosis
- Ciliary muscle: M3 → contraction → accommodation for near vision (loss of far vision = loss of cycloplegia)
Gastrointestinal (M1, M3)
- ↑Peristalsis (↑GI motility); smooth muscle contraction
- Internal sphincters relax
- ↑Gastric acid secretion (M1 on parietal cells and via gastrin release)
- ↑Salivary secretion (M3)
Urinary Tract (M3 dominant, M2 also present)
- Detrusor muscle contraction → urination
- Internal urethral sphincter relaxation
- Both M2 and M3 mRNA predominate in human bladder; M3 drives contraction
Exocrine Glands (M3)
- Salivary, lacrimal, bronchial, sweat glands: all increase secretion
- Sweat glands are anatomically sympathetic but use ACh; blocked by atropine
CNS (M1 dominant; also M2, M4, M5)
- High receptor density in hippocampus, cortex (M1), striatum (M1, M4)
- M1: memory, cognition (target in Alzheimer's research)
- M4: striatum - modulates dopamine (target in schizophrenia)
- M5: on dopaminergic neurons in substantia nigra; cerebrovascular dilation
6. Distribution Summary
| Tissue | Subtype | Effect |
|---|---|---|
| SA/AV node, atria | M2 | Bradycardia, ↓conduction |
| Vascular endothelium | M3 | NO-mediated vasodilation |
| Bronchial SM + glands | M3 | Bronchoconstriction, ↑secretion |
| Bladder detrusor | M2+M3 (M3 functionally dominant) | Contraction (micturition) |
| GI smooth muscle | M3 | Contraction, ↑motility |
| Salivary/lacrimal glands | M3 | Secretion |
| Iris sphincter, ciliary | M3 | Miosis, accommodation |
| Cerebral cortex, hippocampus | M1 | Cognition, memory |
| Striatum | M1, M4 | Motor control, DA modulation |
| Autonomic ganglia | M1 | Ganglionic facilitation |
| Gastric parietal cells | M1 | ↑Acid secretion |
7. Clinically Selective Muscarinic Antagonists
| Drug | Selectivity | Clinical Use |
|---|---|---|
| Atropine | Non-selective | Bradycardia, organophosphate poisoning, preop |
| Scopolamine | Non-selective (CNS >> periphery) | Motion sickness, preoperative sedation |
| Pirenzepine | M1-selective | Peptic ulcer disease (↓gastric acid) |
| Ipratropium | Non-selective (quaternary - no CNS) | COPD, asthma (bronchodilation) |
| Tiotropium | M1/M3 > M2 (long-acting, kinetically selective) | COPD (once daily) |
| Oxybutynin, Tolterodine | M3 (bladder-selective) | Overactive bladder |
| Darifenacin, Solifenacin | M3-preferring | Overactive bladder (fewer cardiac SE) |
| Tropicamide | Non-selective (short duration) | Mydriasis/cycloplegia (eye exam) |
| Benzatropine, Trihexyphenidyl | Central | Parkinson's disease |
Note: Quaternary ammonium muscarinic antagonists (ipratropium, glycopyrrolate, methscopolamine) do NOT cross the blood-brain barrier - used when central effects are unwanted.
8. Muscarinic Agonists (Exam Summary)
| Drug | Properties | Use |
|---|---|---|
| Acetylcholine | Quaternary; rapid hydrolysis; poor oral bioavailability | Intraoperative miosis |
| Methacholine | β-methyl of ACh; resistant to AChE; predominantly muscarinic | Bronchoprovocation test |
| Carbachol | Resistant to all cholinesterases; nicotinic + muscarinic | Glaucoma (topical) |
| Bethanechol | Resistant to hydrolysis; selective muscarinic | Urinary retention, post-op/post-partum ileus |
| Pilocarpine | Tertiary amine (CNS penetration); partial agonist at some sites | Glaucoma, xerostomia |
| Muscarine | Quaternary; fungal toxin | Poisoning (Clitocybe, Inocybe mushrooms) |
Tertiary amines (pilocarpine, arecoline) are orally absorbed and cross the BBB. Quaternary amines (carbachol, bethanechol, muscarine) are poorly absorbed and do not cross the BBB.
9. Muscarinic Toxidrome ("SLUDGE / DUMBELS")
SLUDGE: Salivation, Lacrimation, Urination, Defecation, GI cramps, Emesis
DUMBELS: Defecation/Diarrhea, Urination, Miosis, Bradycardia/Bronchospasm/Bronchorrhea, Emesis, Lacrimation, Salivation/Sweating
Caused by: organophosphates/carbamates (AChE inhibitors), Amanita/Clitocybe mushroom poisoning
Treatment: Atropine (large doses for organophosphate poisoning) + pralidoxime (reactivates AChE before aging)
10. Allosteric Modulation (Advanced/Emerging)
Muscarinic receptors possess allosteric binding sites on extracellular loops distinct from the orthosteric site. These sites vary more among subtypes than the orthosteric site, enabling:
- PAMs (positive allosteric modulators): enhance agonist efficacy (e.g., VU0357017 at M1)
- NAMs (negative allosteric modulators): reduce agonist efficacy
- Bitopic ligands: interact with both orthosteric + allosteric sites simultaneously for high subtype selectivity
This is a major area of drug development for Alzheimer's disease (M1 PAMs) and schizophrenia (M4 PAMs).
High-Yield Exam Points
- M1, M3, M5 = Gq → PLC → IP3/DAG (odd numbers)
- M2, M4 = Gi → ↓cAMP + GIRK channels (even numbers)
- M2 = heart (bradycardia, ↓conduction)
- M3 = smooth muscle + glands (the "effector" receptor)
- M1 = CNS, ganglia, stomach
- Atropine (non-selective antagonist) dose-response: secretions first → mydriasis → tachycardia → bladder → GI → last is gastric secretion
- Muscarinic receptors on vascular endothelium are M3, but NO cholinergic nerve supply - ACh still causes vasodilation via endothelial NO
- All clinical effects of ACh can be blocked by atropine (competitive antagonism)
- Organophosphate poisoning = excess muscarinic (+ nicotinic) stimulation → treat with IV atropine
- Tiotropium is "kinetically selective" for M3 > M2 because it dissociates slowly from M1/M3 but quickly from M2
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Ed. (pp. 227-235); Katzung's Basic and Clinical Pharmacology, 16th Ed.; Campbell-Walsh Urology; Kaplan & Sadock's Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.