Everything about plantar reflex, theory and clinical aspects
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"plantar reflex" OR "Babinski sign" clinical significance
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
plantar reflex Babinski sign neural pathway mechanism surrogate signs clinical significance review
Reading Web Page
plantar reflex mechanism surrogate signs neural pathway clinical significance
Reading File
I now have a comprehensive body of information. Let me compile the full, authoritative response.
The Plantar Reflex — Theory and Clinical Aspects
Historical Background
The plantar reflex's pathological form — the Babinski sign — was first formally described by Joseph Babinski in 1896 (the great toe sign) and again in 1903 (the toe abduction/fan sign). However, it was Remak who in 1893 first observed extensor plantar response in transverse myelitis, preceding Babinski's paper. In modern usage, the toe and fan signs are conflated under the single term "Babinski sign."
Anatomy & Physiology of the Plantar Reflex
The Normal (Flexor) Plantar Reflex
The plantar reflex is a nociceptive segmental spinal reflex that serves to protect the sole of the foot. The reflex arc involves:
- Afferent limb: Nociceptive stimulus applied to the sole → sensory fibers of the S1 dermatome (lateral plantar surface) → dorsal horn of the spinal cord (lumbosacral segments L4–S2)
- Interneurons: Spinal cord circuitry
- Efferent limb: Alpha motor neurons → plantar flexion of all toes
In the normal adult, stroking the lateral sole from heel to toe causes downward (plantar) flexion of all toes — a protective withdrawal.
The Corticospinal Tract (CST) and Its Role
The CST is a descending white matter tract from the cerebral cortex → internal capsule → brainstem → spinal cord, synapsing onto alpha motor neurons (the lower motor neuron, LMN). Key facts:
- 60% of CST fibers originate from the primary motor cortex, premotor areas, and supplementary motor areas
- The remaining 40% originate from primary sensory areas, parietal cortex, and operculum
- The CST exerts tonic inhibitory control over the segmental spinal flexor reflex circuitry
- It maintains territorial integrity of receptive fields: normally, the receptive field for toe extension (dorsum of foot) and toe flexion (sole of foot) remain segregated
When the CST is intact, nociceptive input from the sole activates only S1 anterior horn cells → plantar flexion (normal response).
When the CST is damaged, descending inhibition is lost:
- The receptive field of the toe extensor reflex enlarges at the expense of the flexor field
- Nociceptive input from the sole now spreads to L4/L5 anterior horn cells → contraction of extensor hallucis longus and extensor digitorum longus (via the deep peroneal nerve) → dorsiflexion of the great toe + fanning of other toes (Babinski sign)
The Babinski sign is thus a component of a larger nociceptive synergistic flexion reflex of the leg — "triple flexion" — physiologically a defensive/protective nocifensive response, in which the hip, knee, and ankle flex (dorsiflex). It occurs because of disinhibition or release of spinal motor programs from supraspinal control.
Why Infants Have a Positive Plantar Response
In infants up to approximately 12–18 months, the corticospinal tracts are not fully myelinated/mature. The extensor (Babinski) response is therefore normal in this age group. As the CST matures and myelinates, the plantar response transitions to the adult flexor pattern. Persistence or re-emergence beyond this age is always abnormal.
How to Elicit the Plantar Reflex
Technique (Babinski's method):
- Use a blunt instrument (key, orange stick, or reflex hammer handle)
- Apply firm, continuous pressure to the lateral plantar surface of the foot, starting from the lateral heel, sweeping forward toward the little toe, and arcing medially across the ball of the foot to the base of the great toe
- The stimulus must be firm but not necessarily painful
- Observe the first movement of the hallux
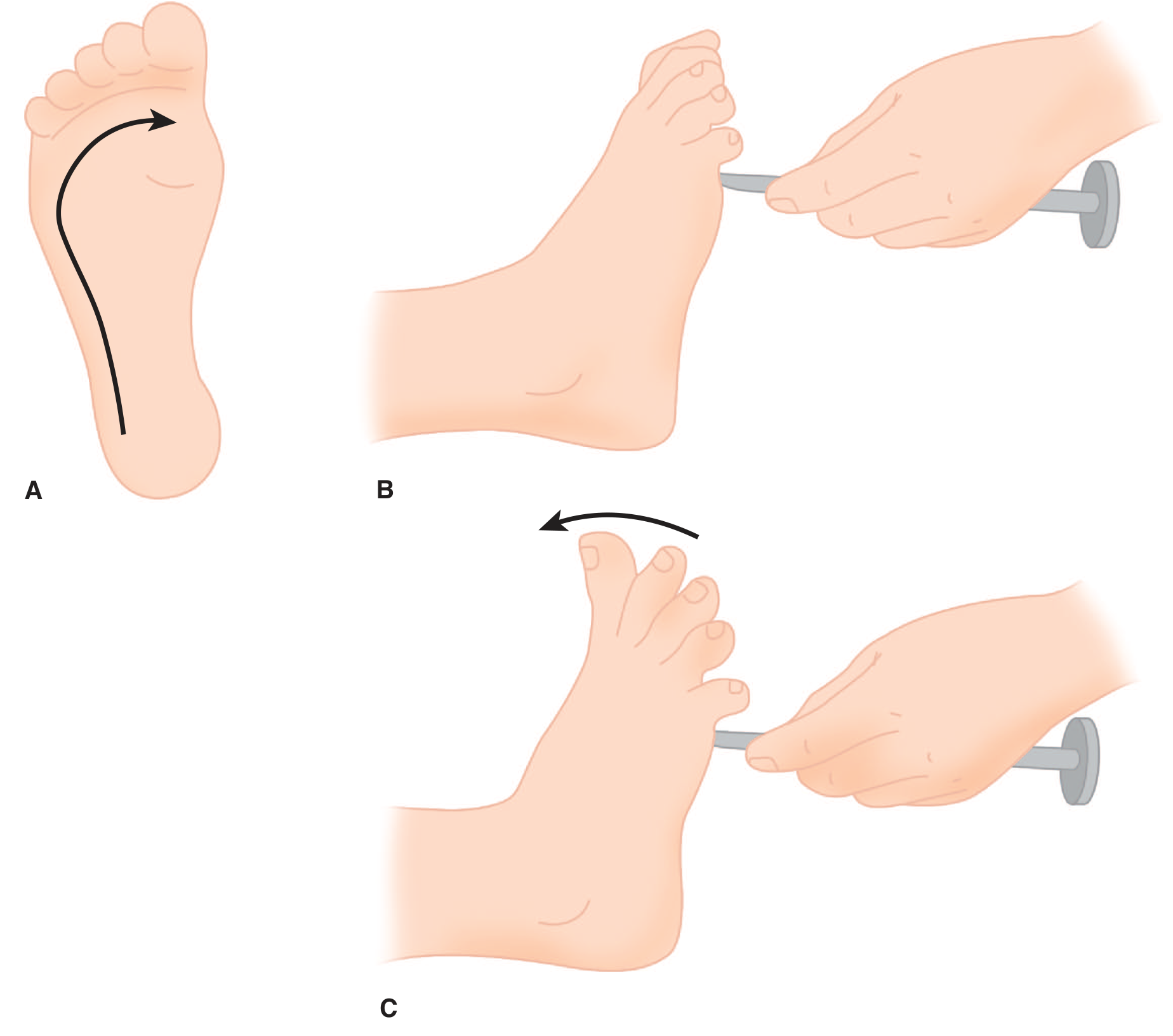
Figure: A. The plantar response is elicited by stroking from the heel to the ball of the foot. B. The normal plantar response consists of flexion of the toes. C. The extensor plantar response (Babinski sign) = extension of the great toe coupled with fanning of the remaining digits. — Adams & Victor's Principles of Neurology, 12th ed.
Interpreting the Response
| Response | Significance |
|---|---|
| Toes flex downward | Normal in adults — intact CST |
| Great toe dorsiflexes + other toes fan | Babinski sign = UMN lesion |
| Toes silent (no movement) | If contralateral side shows flexion → the silent side is abnormal |
| Triple flexion (hip + knee flex + ankle dorsiflexes) | Same significance as Babinski; spinal cord circuitry only; seen in severe UMN lesions, coma |
Pitfalls:
- A quick withdrawal response (rapid leg withdrawal) does NOT signify disease and must be distinguished from the true Babinski response
- The pathological Babinski is a slower, sustained movement
- Severe weakness of the toe extensors may prevent elicitation of the sign even when the CST is damaged
- Avoidance/withdrawal can interfere with interpretation → use surrogate maneuvers in such cases
Surrogate Signs (Equivalent Responses)
Several dozen alternative maneuvers have been described, all with the same clinical significance as the Babinski response. The most important:
| Sign | Stimulus |
|---|---|
| Chaddock | Stroke under the lateral malleolus |
| Oppenheim | Firm pressure applied down the medial side of the tibia |
| Gordon | Squeeze the calf muscle |
| Throckmorton | Strike the metatarsophalangeal joint of the great toe |
| Stransky | Abduct and release the little toe |
| Schaeffer | Pinch the Achilles tendon |
| Bing | Prick the dorsum of the foot |
These alternatives are especially valuable when the patient has a strong withdrawal response to sole stimulation, when the sole is hypersensitive (calluses, wounds), or when the patient cannot relax. The mechanism for all surrogates is likely the same as the Babinski response: expansion of the receptive field for extensor hallucis longus activation due to CST failure.
Clinical Significance: Conditions Producing a Positive Babinski Sign
Upper Motor Neuron Lesions (Structural)
The Babinski sign indicates damage anywhere along the corticospinal tract, including:
- Cerebral cortex: Stroke, tumor, abscess, contusion, AVM
- Internal capsule: Lacunar infarct, hemorrhage
- Brainstem: Infarct, demyelination, herniation
- Spinal cord: Trauma, infarct (anterior spinal artery), myelitis, compression (tumor, disc herniation, epidural abscess), multiple sclerosis, syringomyelia, ALS
- Parasagittal lesions (bilateral Babinski): Parasagittal meningioma, hydrocephalus, falcine herniation
Accompanying UMN signs (Adams & Victor):
- Spasticity, hypertonia (clasp-knife)
- Hyperactive deep tendon reflexes, clonus
- Weakness (upper > lower limb; extensors > flexors in leg)
- Loss of superficial abdominal and cremasteric reflexes (important ancillary signs)
- Pronator drift
- Hoffmann sign (upper limb equivalent)
Versus LMN signs (which show plantar flexion or absent reflex): flaccidity, atrophy, fasciculations, hyporeflexia.
Metabolic/Toxic/Physiological States
The Babinski sign may also appear transiently in:
- Hypoglycemia (reversible with glucose)
- Hypoxia and severe anemia
- General anesthesia (both induction and deep stages)
- Hepatic encephalopathy (along with asterixis, hyperreflexia)
- Postictal state (Todd's paresis after a seizure — resolves within minutes to hours)
- Deep sleep (transient)
- Hypothermia
- Drug intoxication (e.g., phenytoin toxicity)
These transient states are critical to recognize: a positive Babinski post-seizure does not imply a permanent structural lesion.
The Plantar Reflex in Specific Clinical Contexts
Spinal Shock
After acute spinal cord injury, spinal shock produces initial areflexia below the lesion. The sequence of reflex return (Ditunno et al., 2004) is:
- Phase 1 (0–24 h): Areflexia/hyporeflexia; the delayed plantar reflex is the first pathological reflex to appear
- Phase 2 (Day 1–3): Cutaneous reflexes return (bulbocavernosus, cremasteric); deep tendon reflexes remain absent; Babinski sign may appear in elderly
- Phase 3 (Day 4–30): Deep tendon reflexes return; Babinski recovery closely parallels ankle jerk return; delayed plantar reflex diminishes
- Phase 4 (1–12 months): Hyperreflexia, spasticity, autonomous dysreflexia
— Bradley and Daroff's Neurology in Clinical Practice
Emergency Medicine
In spinal cord emergencies, hyperreflexia, clonus, or a Babinski sign suggests upper motor neuron pathology (cord impingement). Assessment of patellar/Achilles reflexes and plantar response are essential. Abnormal plantar reflex alongside loss of sphincter control indicates urgent decompressive intervention. — Rosen's Emergency Medicine
Coma Assessment
In comatose patients, triple flexion (spinal cord circuitry only, no brainstem required) must be distinguished from decorticate/decerebrate posturing (requires brainstem). Triple flexion does not exclude brain death if deep tendon reflexes are intact without brainstem signs. — Neuroanatomy Through Clinical Cases, 3rd ed.
Comparison: UMN vs. LMN Lesions
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Plantar reflex | Extensor (Babinski +) | Flexor or absent |
| Tone | Spastic (clasp-knife) | Flaccid |
| Reflexes | Hyperreflexia, clonus | Hyporeflexia/areflexia |
| Atrophy | Absent (disuse only, late) | Present, early |
| Fasciculations | Absent | Present |
| Weakness distribution | Pyramidal pattern | Segmental/root/nerve |
Physiological Mechanism — Summary
The essential mechanism (NCBI Clinical Methods / Landau 1971):
The abnormal plantar reflex is the elicitation of toe extension from the "wrong" receptive field — the sole of the foot. The key phenomenon is recruitment of extensor hallucis longus, with consequent overpowering of the toe flexors. The corticospinal tract normally maintains territorial integrity of receptive fields. When it fails, the receptive field of the normal toe extensor reflex enlarges at the expense of the flexor field, so that nociceptive input spreads beyond S1 anterior horn cells to L4/L5 anterior horn cells, activating extensor hallucis longus and extensor digitorum longus via the deep peroneal nerve.
Key Teaching Points
- The plantar reflex is a nociceptive segmental spinal reflex; its normal response is toe flexion (protective)
- The Babinski sign = extensor response = reliable marker of corticospinal (UMN) dysfunction anywhere along the tract
- Positive in normal infants up to ~12–18 months (immature CST); always abnormal beyond that age
- Absent Babinski does not exclude a UMN lesion — severe toe extensor weakness may prevent it
- Surrogate signs (Chaddock, Oppenheim, Gordon, etc.) have identical significance
- Triple flexion has the same significance as Babinski but requires only spinal circuitry
- Transient positivity occurs in metabolic states (hypoglycemia, anesthesia, hypoxia, postictal) — not necessarily structural
- In spinal shock, the delayed plantar reflex is the first abnormal sign to appear; Babinski's return parallels the ankle jerk
- The superficial abdominal and cremasteric reflexes are abolished in UMN lesions and serve as important ancillary signs
Sources: Adams & Victor's Principles of Neurology, 12th ed. | Neuroanatomy Through Clinical Cases, 3rd ed. | Ganong's Review of Medical Physiology, 26th ed. | Gray's Anatomy for Students | Bradley and Daroff's Neurology in Clinical Practice | Rosen's Emergency Medicine | NCBI Clinical Methods (NBK397) | StatPearls (NBK519009)
This is a shared conversation. Sign in to Orris to start your own chat.