Enterohepatic circulation explain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have rich content from multiple authoritative textbooks and a detailed diagram. Let me compile the comprehensive answer.
Enterohepatic Circulation
Definition
Enterohepatic circulation (EHC) refers to the cyclic movement of substances - primarily bile acids - between the liver, biliary tract, gallbladder, small intestine, and back to the liver via the portal venous system. The anatomic components are: liver, biliary tract, gallbladder, small intestine, portal vein, and to a lesser extent the colon and systemic circulation.
It can be thought of as a series of storage chambers (gallbladder, small intestine), valves (sphincter of Oddi, ileocecal valve), mechanical pumps (small intestine peristalsis), and chemical pumps (hepatocytes, cholangiocytes, ileocytes).
- Sleisenger & Fordtran's GI and Liver Disease, p. 1204
- Harrison's Principles of Internal Medicine 22E, p. 2771
The Bile Acid Pool - Key Numbers
| Parameter | Value |
|---|---|
| Total bile acid pool | 2-4 g |
| Daily cycles through EHC | 5-10 times |
| Daily amount secreted | 15-30 g |
| Intestinal reabsorption efficiency | ~95% |
| Daily fecal loss | 0.2-0.6 g |
| Daily hepatic synthesis to replace loss | ~0.5 g |
- Harrison's 22E, p. 2771; Lippincott Biochemistry 8th Ed., p. 633
Step-by-Step Circuit
1. Hepatic Synthesis & Secretion
- The liver synthesizes primary bile acids: cholic acid and chenodeoxycholic acid from cholesterol (rate-limiting step: CYP7A1, i.e., cholesterol 7-alpha-hydroxylase).
- These are conjugated with glycine or taurine in hepatocytes to form bile salts.
- Bile salts are actively secreted into bile canaliculi via BSEP (Bile Salt Export Pump, ABCB11), an ATP-dependent transporter.
2. Gallbladder Storage (Fasting State)
- Between meals, the sphincter of Oddi contracts. Bile flows into the gallbladder, where it is concentrated ~10-fold by water and electrolyte absorption.
- Almost the entire bile acid pool may be sequestered in the gallbladder overnight for delivery with the first meal.
3. Postprandial Release
- Fat and amino acids in the duodenum trigger release of CCK (cholecystokinin) from intestinal mucosa.
- CCK causes: gallbladder contraction + sphincter of Oddi relaxation → bile empties into duodenum.
- Intraluminal bile acid concentration reaches 5-10 mmol/L (well above the critical micellar concentration of ~1.5 mmol/L).
4. Intestinal Functions
- Bile acids form mixed micelles with phospholipids and cholesterol, which:
- Activate pancreatic lipase on triglycerides
- Solubilize long-chain fatty acids, monoglycerides, cholesterol
- Shuttle hydrophobic lipids across the unstirred water layer to the mucosal surface for absorption
- Facilitate absorption of fat-soluble vitamins (A, D, E, K)
5. Ileal Reabsorption (Active - Primary Route)
- Conjugated bile acids are actively reabsorbed in the terminal ileum via ASBT (Apical Sodium-dependent Bile Salt Transporter, SLC10A2) - a Na⁺-bile salt co-transporter.
- They exit the ileocyte basolaterally via OST-alpha/OST-beta transporters into the portal blood.
- Unconjugated bile acids may be passively absorbed along the entire small intestine (less efficient).
Why the ileum? Keeping active absorption at the terminal ileum ensures bile acids remain at high concentration throughout the entire small intestine to maximize fat digestion.
6. Portal Return to the Liver
- Bile acids are transported in portal blood bound to albumin.
- Hepatocytes extract them with >90% first-pass efficiency via:
- NTCP (Na⁺-taurocholate co-transporting polypeptide, SLC10A1) - for conjugated bile acids
- OATPs (Organic Anion Transporting Polypeptides) - for unconjugated bile acids
- The liver reconjugates, processes, and re-secretes them into bile - completing the circuit.
Here is the transport protein diagram from Sleisenger & Fordtran showing all cell-level transporters:
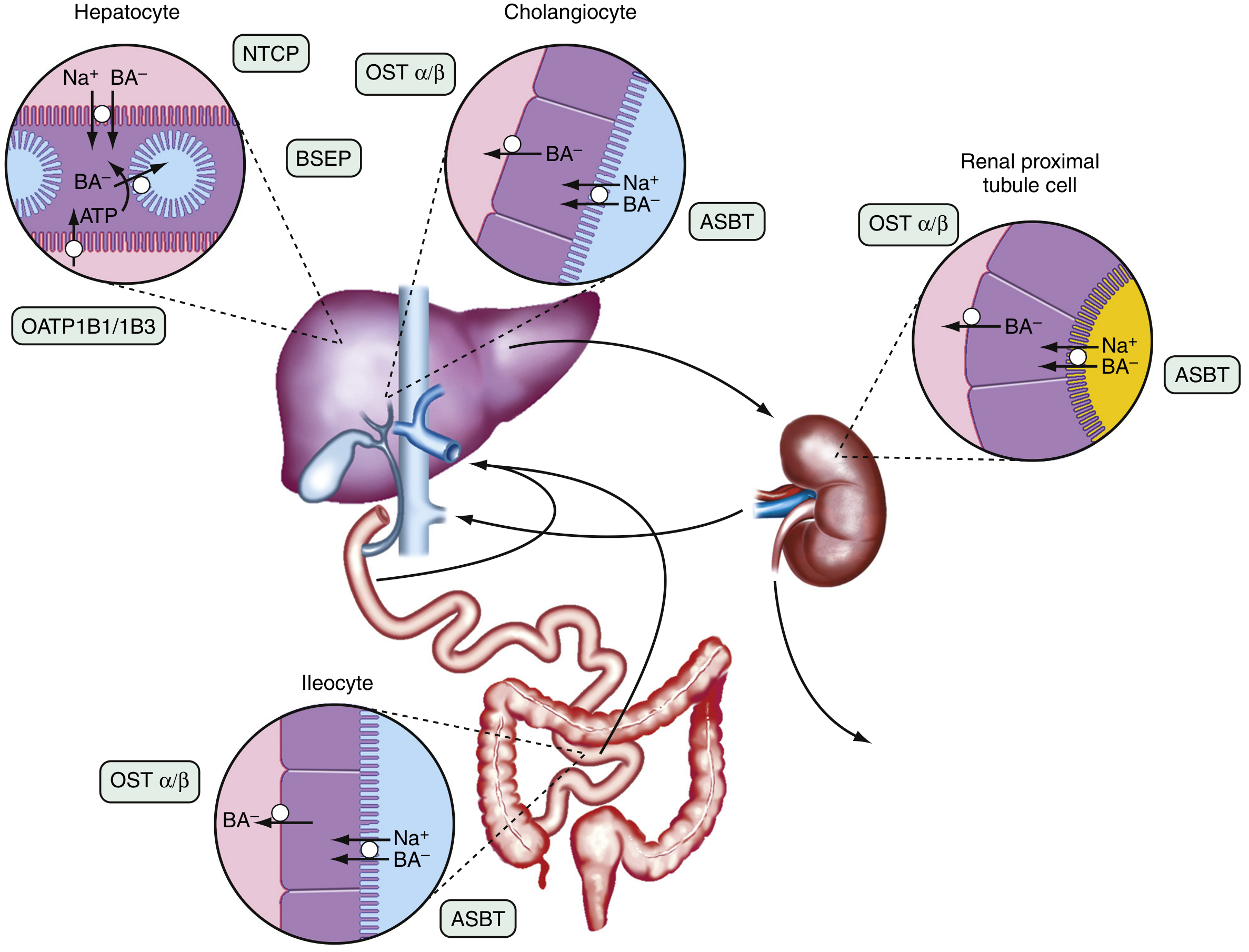
Fig. 64.3 - Enterohepatic circulation of bile acids showing individual transport proteins. NTCP: Na⁺-taurocholate cotransporting polypeptide; BSEP: bile salt export pump; ASBT: apical sodium bile acid transporter; OATP: organic anion transporting polypeptide; OST: organic solute transporter. (Sleisenger & Fordtran)
Secondary Bile Acids & Bacterial Modification
- Bacteria in the colon deconjugate bile salts (remove glycine/taurine) and dehydroxylate at C-7:
- Cholic acid → Deoxycholic acid
- Chenodeoxycholic acid → Lithocholic acid (poorly absorbed; mostly excreted)
- A small proportion of these secondary bile acids are absorbed by colonic epithelium and returned to the liver, where they may be re-conjugated and hydroxylated.
- Lippincott Biochemistry 8th Ed., p. 634
Regulation of the Cycle
| Regulator | Role |
|---|---|
| CYP7A1 | Rate-limiting enzyme for bile acid synthesis from cholesterol; inhibited by returning bile acids (negative feedback) |
| FGF19 (Fibroblast Growth Factor 19) | Released by ileal enterocytes in response to bile acids; suppresses hepatic CYP7A1 and promotes gallbladder relaxation |
| FXR (Farnesoid X Receptor) | Nuclear receptor activated by bile acids; upregulates BSEP and represses bile acid synthesis |
| LXR (Liver X Receptor) | Oxysterol sensor; upregulates cholesterol transporter ABCG5/G8 |
| CCK | Triggers postprandial gallbladder emptying |
| TGR5 | G-protein-coupled receptor activated by bile acids; indirectly mediates gallbladder relaxation via FGF19 |
- Harrison's 22E, p. 2771; Sleisenger & Fordtran
Functions of EHC (Beyond Bile Acid Recycling)
- Primary mechanism for excreting excess cholesterol - cholesterol is consumed during bile acid synthesis and excreted in micelles in stool
- Fat digestion - micelle formation is required for dietary lipid absorption
- Fat-soluble vitamin absorption (A, D, E, K)
- Lipophilic drug absorption
- Regulation of water movement - in hepatocytes (into bile) and across small bowel
- Feedback regulation of cholesterol and bile acid synthesis
- Sabiston Textbook of Surgery, p. 1873
Clinical Significance & Disorders
1. Ileal Resection / Disease (Crohn's disease)
- Loss of terminal ileum disrupts active ASBT-mediated reabsorption
- Large quantities of bile salts lost in stool - hepatic synthesis cannot compensate (max ~5 g/day)
- Depleted bile acid pool → impaired fat absorption → steatorrhea and fat-soluble vitamin deficiency
- Excess bile acids reaching colon → secretory diarrhea (bile acid diarrhea)
- Costanzo Physiology 7th Ed.; Harrison's 22E
2. Cholelithiasis (Gallstones)
- If bile acids decrease relative to cholesterol and phospholipids in bile, cholesterol precipitates → cholesterol gallstones
- Caused by decreased bile acids or increased cholesterol secretion into bile
- Lippincott Biochemistry 8th Ed., p. 634
3. Cholestasis
- Classified as intrahepatic (hepatocyte transport defect) or extrahepatic (biliary obstruction)
- EHC disorders fall into 4 categories:
- Defects in bile acid formation (synthesis/conjugation)
- Defects in membrane transport (BSEP, NTCP mutations)
- Disturbances in bacterial transformation
- Disturbances in circulation between organs
- Sleisenger & Fordtran, p. 1455
4. Pharmacological Applications
- Bile acid sequestrants (cholestyramine, colestipol, colesevelam): bind bile acids in gut, prevent reabsorption → liver draws more cholesterol into bile acid synthesis → lowers LDL cholesterol. Used in hypercholesterolemia.
- These resins also affect drugs undergoing EHC (e.g., digoxin, warfarin) by binding them in the gut
- Activated charcoal (multi-dose): interrupts EHC of drugs with long half-lives (e.g., carbamazepine, dapsone, diazepam, amitriptyline) - used in overdose management
- Cholestyramine in thyrotoxicosis: reduces EHC of thyroid hormones, helping lower thyroid hormone levels
- Katzung Pharmacology 16th Ed.; Tintinalli's Emergency Medicine
5. Drugs with Significant EHC
Drugs secreted in bile, released in gut, and reabsorbed include:
- Diazepam (secondary plasma peak 6-12 h after dose)
- Morphine, chloramphenicol, rifampicin, oral contraceptives, NSAIDs
- This prolongs their half-life and can produce secondary plasma concentration peaks
- Morgan & Mikhail's Clinical Anesthesiology 7e
Summary Diagram (Lippincott)

(Note: If the Lippincott image does not load, refer to the Sleisenger & Fordtran transport diagram above for the full circuit.)
Quick Summary
Liver (synthesis + conjugation)
↓ BSEP
Bile canaliculi → Bile ducts → Gallbladder (concentration, storage)
↓ CCK-triggered release
Duodenum/Small Intestine (micelle formation → fat absorption)
↓ 95% reabsorbed in terminal ileum via ASBT
Portal vein
↓ NTCP / OATPs
Liver (extraction >90%, reconjugation, re-secretion) → cycle repeats 5-10x/day
↓ 5% lost
Colon (bacterial modification → secondary bile acids) → Feces (0.5 g/day lost)
The liver synthesizes ~0.5 g/day to replace fecal losses, under negative feedback control by returning bile acids via FXR and FGF19.
This is a shared conversation. Sign in to Orris to start your own chat.