what are the DDx of a HEADACHE in a 25 year old male, the headache is continuous in nature and doesnt respond to OTC analgesics!?
Reading File
Finding Sources
Finding Sources
Searching the Web
differential diagnosis continuous headache young adult not responding to OTC analgesics
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-structured answer. Let me compile it.
Differential Diagnosis: Continuous Headache in a 25-Year-Old Male, Not Responding to OTC Analgesics
The key clinical features driving this DDx are: young male, continuous (non-episodic) nature, and OTC analgesic failure. These features push the list heavily toward secondary causes that need to be excluded before settling on a primary headache disorder.
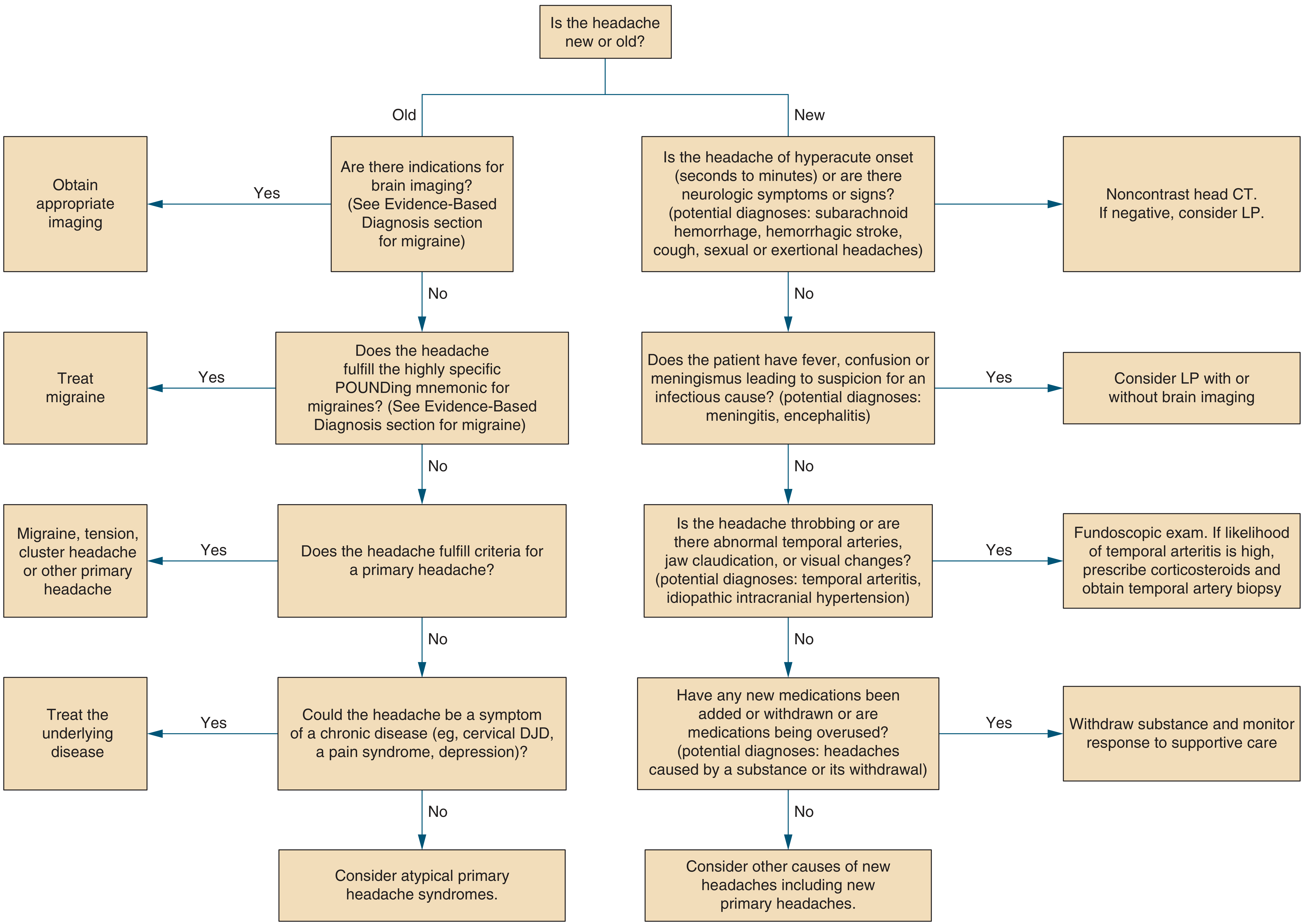
Here is the diagnostic flowchart to guide your approach:
SECONDARY CAUSES (Must Exclude First - "Red Flags")
These are dangerous diagnoses that require urgent workup. The continuous nature and analgesic failure should raise suspicion.
1. Cerebral Venous Sinus Thrombosis (CVST)
- Why first in a 25 M: Young patients are classic. The textbook from Grainger & Allison's Diagnostic Radiology specifically highlights a young male presenting with headache and seizures due to CVST.
- Progressive, often positional, may worsen over days to weeks
- Associated: papilledema, focal deficits, seizures
- Workup: MRI + MRV
2. Idiopathic Intracranial Hypertension (IIH / Pseudotumor Cerebri)
- Though classically seen in obese women, it CAN occur in young males
- Headache worsens with Valsalva, associated pulsatile tinnitus, transient visual obscurations, papilledema
- CSF opening pressure >25 cmH₂O on LP; normal neuroimaging
3. Intracranial Mass / Brain Tumor
- Continuous, progressive headache worse in the morning or with position change
- May be primary (glioma) or secondary (metastasis)
- Associated: focal neuro deficits, personality change, seizures, papilledema
- Workup: MRI with contrast
4. Meningitis / Meningoencephalitis
- Bacterial, viral, TB, fungal (especially cryptococcal in immunocompromised)
- Look for: fever, neck stiffness, photophobia, altered consciousness
- Workup: LP after CT head
5. Subarachnoid Hemorrhage (SAH) - or Post-SAH
- Classic "thunderclap" onset, but a small sentinel bleed can present as persistent, dull headache
- Do NOT miss - CT head (non-contrast) + LP if CT negative
6. Subdural Hematoma
- Can be chronic, especially after trivial or forgotten head trauma
- Continuous dull headache, may have mild cognitive slowing
- May lack obvious trauma history in young patients
7. Carotid or Vertebral Artery Dissection
- Persistent unilateral neck/head pain; may follow minor trauma, chiropractic manipulation, or be spontaneous
- Look for Horner syndrome, focal ischemic symptoms
- Workup: MRA/CTA neck
8. Malignant / Accelerated Hypertension
- Check BP - often overlooked in young males
- Occipital headache, may have blurred vision, nausea
9. Sinusitis / Intracranial Extension
- Typically frontal/facial, worsens with bending forward
- Complicated sinusitis can cause persistent headache through cavernous sinus or epidural abscess
10. Carbon Monoxide Poisoning
- Often underdiagnosed; bilateral, continuous, associated with nausea, fatigue
- Multiple household members affected is a clue
PRIMARY HEADACHE DISORDERS (Once Secondary Causes Excluded)
These can present as continuous or near-continuous headache and may not respond to OTC analgesics without specific treatment.
| Diagnosis | Key Features | OTC Response |
|---|---|---|
| Chronic Migraine | >15 headache days/month, unilateral/bilateral, throbbing, nausea/photo/phonophobia | Often inadequate - needs triptans, CGRP agents |
| New Daily Persistent Headache (NDPH) | Abrupt-onset continuous headache, exact date of onset recalled, no prior history | Poor to OTC; specific treatments needed |
| Chronic Tension-Type Headache | Bilateral, pressing/band-like, >15 days/month, no nausea | Often OTC-resistant when chronic |
| Hemicrania Continua | Strictly unilateral, continuous with superimposed jabs, ipsilateral autonomic features | Pathognomonic response to INDOMETHACIN only - not standard OTC NSAIDs |
| Medication Overuse Headache (MOH) | Paradoxically worsens with analgesic use >10-15 days/month; arises on a background of pre-existing headache | Worsens with OTC use |
| Cluster Headache | More frequent in men; severe unilateral periorbital pain, autonomic features; but typically episodic (30-90 min), not truly continuous | OTC ineffective; needs O₂, triptans, verapamil |
- Goldman-Cecil Medicine, Table 367-3
- Neuroanatomy through Clinical Cases, Table 5.2
SNNOOP10 Red Flags to Actively Seek
These features, when present, mandate urgent secondary workup:
-
S - Systemic symptoms (fever, weight loss)
-
N - Neoplasm history
-
N - Neurologic deficit (focal)
-
O - Onset sudden/abrupt (thunderclap)
-
O - Older age at new onset (less relevant here, but still)
-
P - Positional headache (worse lying flat - suggests IIH; worse upright - suggests low CSF pressure)
-
P - Papilledema
-
O - Optic disc pathology
-
P - Prior headache history change
-
10 - Sleep-related headache, pregnancy/postpartum, trauma, immune-compromise, etc.
-
AAFP Acute Headache Guidelines uses this framework in practice
Practical Workup Approach
- History: Onset (sudden vs gradual), character, location, associated symptoms, prior headache history, medications, trauma, systemic illness, sexual history/STIs
- Vitals + fundoscopy: BP, papilledema assessment
- CT head (non-contrast) - if red flags are present (trauma, thunderclap, focal signs, fever)
- MRI brain + gadolinium + MRV - if CVST, mass, or IIH suspected
- LP - if meningitis or SAH suspected after negative CT; check opening pressure for IIH
- Blood tests: CBC, ESR/CRP, metabolic panel, hypercoagulability panel (if CVST suspected)
- Indomethacin trial - if hemicrania continua is suspected (strictly unilateral, continuous, with autonomic features)
Bottom line: In a 25-year-old male with a continuous headache unresponsive to OTC analgesics, the diagnosis is NOT benign until proven otherwise. CVST, IIH, intracranial mass, meningitis, and SAH must be excluded before attributing this to a primary headache disorder. Among primary disorders, hemicrania continua and NDPH are the most likely to present exactly this way - continuous, unresponsive to standard analgesics - and require specific treatments.
Find recent clinical guidelines on evaluating new-onset continuous headaches
Reading File
Searching PubMed
"headache" AND "guideline" AND "evaluation"
Searching PubMed
"new daily persistent headache" OR "continuous headache" AND "diagnosis"
Searching the Web
clinical guidelines new onset continuous headache evaluation 2023 2024 AAN EHF
Reading Article
PMID: 39467289
Reading Article
PMID: 37032616
Searching PubMed
"headache" AND "neuroimaging" AND "secondary" AND "red flags"
Reading Article
PMID: 38419454
Reading Article
PMID: 34894320
Reading Article
PMID: 40864527
Searching the Web
ICHD-3 new daily persistent headache diagnostic criteria evaluation workup 2024
Excellent - I have comprehensive, current evidence. Let me compile the full answer.
Recent Clinical Guidelines: Evaluating New-Onset Continuous Headache
Here is a synthesis of the most current peer-reviewed guidelines, society recommendations, and evidence-based reviews, organized by topic and evidence strength.
1. The Gold-Standard Classification Framework: ICHD-3
The International Classification of Headache Disorders, 3rd Edition (ICHD-3) remains the foundational diagnostic reference. For a new-onset continuous headache that fits the presentation in our case, the specific ICHD-3 category is:
New Daily Persistent Headache (NDPH) - Code 4.10
ICHD-3 diagnostic criteria:
- Persistent headache fulfilling criteria B and C
- Distinct and clearly remembered onset, with pain becoming continuous and unremitting within 24 hours
- Present for >3 months
- Not better accounted for by another ICHD-3 diagnosis
Critical point: Before NDPH can be diagnosed, ALL secondary causes must be excluded. ICHD-3 criterion 4 is non-negotiable - secondary headaches that mimic NDPH are common and dangerous.
- If present for <3 months but otherwise meeting criteria: code as 4.10.1 Probable NDPH
2. Major Society Guidelines (2022-2025)
2023 VA/DoD Clinical Practice Guideline for Headache Management
[Sico et al., Ann Intern Med, 2024 - PMID: 39467289] - Practice Guideline
This is one of the most comprehensive recent multi-domain guidelines. Key evaluation-relevant recommendations:
- Includes 52 evidence-based recommendations covering evaluation, pharmacotherapy, and non-pharmacologic management
- Emphasizes structured evaluation of both primary and secondary headache disorders before treatment
- Updated ahead of schedule (normally 5-year cycle) due to rapidly expanding evidence
- Note: An erratum was published (PMID: 40258283)
European Academy of Neurology (EAN) - Cluster Headache Guidelines 2023
[May et al., Eur J Neurol, 2023 - PMID: 37515405] - Practice Guideline
Relevant because cluster headache (a TAC) must be in the DDx of any new continuous headache in a young male. EAN guidelines specify diagnostic criteria and workup pathways.
American College of Physicians (ACP) - 2025 Migraine Prevention Guideline
[Qaseem et al., Ann Intern Med, 2025 - PMID: 39899861] - Practice Guideline
While treatment-focused, the evaluation algorithm includes ruling out secondary causes before initiating prevention therapy.
3. Diagnostic Approach: Red Flags vs. Green Flags (2021, IHS Special Interest Group)
[Do et al., Curr Pain Headache Rep, 2021 - PMID: 34894320] - Review (Ashina M, lead author)
This is a key methodological update from an International Headache Society special interest group. Key findings:
- Introduced the concept of "green flags" (features suggesting primary headache) alongside the established red flag system
- Red flags = signal secondary etiology; green flags = support primary diagnosis
- A dual-flag approach reduces unnecessary testing while maintaining diagnostic safety
- Validated the SNNOOP10 list as the most systematic red flag framework in current use
SNNOOP10 (the current standard red-flag mnemonic):
| Letter | Red Flag |
|---|---|
| S | Systemic symptoms (fever, weight loss, night sweats) |
| N | Neoplasm history |
| N | Neurologic deficit or dysfunction |
| O | Onset sudden/abrupt (thunderclap) |
| O | Older age (>50 new onset) |
| P | Pattern change or progressive worsening |
| P | Papilledema |
| P | Positional headache |
| 1 | Precipitated by Valsalva/cough/exercise/sex |
| 0 | Post-traumatic onset |
4. Differentiating Primary vs. Secondary Etiologies - Neuroimaging Guidance
[Hernandez et al., J Integr Neurosci, 2024 - PMID: 38419454] - Review
Current evidence-based workup principles:
- A thorough history and neuro exam is the primary diagnostic tool - no validated biomarkers exist yet
- When red flags are present: neuroimaging is mandatory
- Imaging modality selection is guided by suspected secondary cause:
| Suspected Cause | Recommended Imaging |
|---|---|
| SAH, hemorrhage | Non-contrast CT head first (within 6 hrs); if negative, LP or CT angiography |
| CVST | MRI brain + MRV |
| Mass lesion / IIH | MRI brain with and without contrast |
| Arterial dissection | MRI/MRA or CTA neck |
| Spontaneous intracranial hypotension | MRI brain with gadolinium (pachymeningeal enhancement) |
| No red flags present | Primary headache more likely; neuroimaging may not be needed |
5. New Daily Persistent Headache (NDPH) - Best Available Evidence
Systematic Review & Meta-Analysis (2023)
[Cheema et al., Cephalalgia, 2023 - PMID: 37032616] - Systematic Review + Meta-Analysis (Tier 1)
46 studies, 2,155 NDPH patients. Key findings directly relevant to evaluation:
- 67% of NDPH has a chronic migraine phenotype - easily misclassified
- NDPH is less likely than chronic migraine to: have a family headache history, respond to injectable or neuromodulatory treatments
- NDPH is less vulnerable to medication overuse than chronic migraine (important differentiator)
- Conclusion: NDPH remains a diagnosis of exclusion; further high-quality evidence is needed
Epidemiology Meta-Analysis (2025 - Most Recent)
[Osiowski et al., Headache, 2025 - PMID: 40864527] - Systematic Review + Meta-Analysis (Tier 1)
30 studies, 74,253 individuals:
- General adult population prevalence: 0.06% (rare)
- In headache clinic populations: 1.23% of adults, 2.39% of children
- Among chronic daily headache patients: 3.91% of adults, 19.60% of children/adolescents
- Mean age of onset: ~37-40 years in adults (your 25-year-old patient is slightly younger than typical)
- Female predominance, but not statistically significant across all studies
- Delayed diagnosis is common due to variable clinical presentations and frequent misclassification
6. Recommended Evaluation Pathway (Evidence-Based Summary)
Based on the convergence of ICHD-3, VA/DoD 2023 CPG, IHS red flag framework, and current reviews:
Step 1: History
├── Onset: exact date/time recalled? (NDPH hallmark)
├── Was it truly sudden (thunderclap) → think SAH, RCVS, CVST
├── Character: migraine-like vs. tension-like vs. autonomic features
├── Positional component? Worse lying down = raised ICP; worse upright = low CSF pressure
├── Associated: fever, visual changes, focal deficits, weight loss
└── Medications: current and prior (exclude MOH)
Step 2: Physical Examination
├── BP measurement (mandatory)
├── Full neurological exam
└── Fundoscopy: papilledema = raised ICP until proven otherwise
Step 3: Imaging (if ANY red flag present)
├── CT head non-contrast → SAH, hemorrhage, acute hydrocephalus
├── MRI brain + gadolinium → mass, metastasis, SIH, meningitis
├── MRI + MRV → CVST
└── MRA/CTA neck → dissection
Step 4: LP (if indicated)
├── After negative CT in suspected SAH/meningitis
└── Opening pressure for IIH
Step 5: If all secondary causes excluded
└── Characterize primary disorder using ICHD-3 criteria
├── NDPH (exact onset recalled, continuous from day 1)
├── Chronic migraine
├── Hemicrania continua (indomethacin trial)
└── Chronic tension-type headache
Key References (Citable)
| Evidence | Citation |
|---|---|
| Systematic Review + Meta-Analysis | Cheema S, et al. New daily persistent headache: A systematic review and meta-analysis. Cephalalgia. 2023. PMID: 37032616 |
| Systematic Review + Meta-Analysis (2025) | Osiowski M, et al. Epidemiology of new daily persistent headache. Headache. 2025. PMID: 40864527 |
| Practice Guideline | Sico JJ, et al. 2023 VA/DoD Clinical Practice Guideline for Headache. Ann Intern Med. 2024. PMID: 39467289 |
| IHS Diagnostic Framework | Do TP, et al. Updates in the Diagnostic Approach of Headache. Curr Pain Headache Rep. 2021. PMID: 34894320 |
| Primary vs. Secondary DDx | Hernandez J, et al. Headache Disorders: Differentiating Primary and Secondary Etiologies. J Integr Neurosci. 2024. PMID: 38419454 |
| Classification | ICHD-3 Criteria for NDPH |
Bottom line from the guidelines: A new continuous headache in a young adult is a diagnosis of exclusion. Current guidelines (VA/DoD 2023, ICHD-3, IHS red flag framework) uniformly mandate ruling out secondary causes - especially CVST, IIH, intracranial mass, meningitis, and SAH - before labeling the patient with NDPH or any other primary headache disorder. MRI brain + MRV is the imaging modality of choice when the onset is not thunderclap.
This is a shared conversation. Sign in to Orris to start your own chat.