Give all details and classification of thyroid lesion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
thyroid neoplasm classification WHO 2022
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive material from Robbins & Kumar Basic Pathology and Cummings Otolaryngology. Let me compile the full, detailed answer.
Thyroid Lesions - Classification and Full Details
Sources: Robbins & Kumar Basic Pathology; Cummings Otolaryngology Head and Neck Surgery; Fischer's Mastery of Surgery
MASTER CLASSIFICATION OF THYROID LESIONS
THYROID LESIONS
├── A. NON-NEOPLASTIC
│ ├── Goiter (Diffuse / Multinodular)
│ └── Thyroiditis
│ ├── Hashimoto
│ ├── Subacute Granulomatous (de Quervain)
│ ├── Painless (Subacute Lymphocytic)
│ └── Riedel
├── B. BENIGN NEOPLASMS
│ └── Follicular Adenoma
│ ├── Nonfunctioning (cold nodule)
│ └── Toxic Adenoma (hot nodule)
└── C. MALIGNANT NEOPLASMS (Thyroid Carcinoma)
├── Papillary Thyroid Carcinoma (PTC) - >85%
├── Follicular Thyroid Carcinoma (FTC) - 5-15%
├── Anaplastic (Undifferentiated) Carcinoma - <5%
└── Medullary Thyroid Carcinoma (MTC) - ~5%
PART I: NON-NEOPLASTIC LESIONS
1. Goiter
Diffuse Goiter
Caused by reduced thyroid hormone synthesis, most commonly from dietary iodine deficiency. Low T3/T4 drives a compensatory TSH rise, causing follicular cell hypertrophy and hyperplasia. Endemic goiter applies when >10% of a population in a given region is affected. Sporadic goiter is more common in females, peaking at puberty or young adulthood; causes include goitrogenic foods (Brassicaceae vegetables, calcium) and inherited enzyme defects (dyshormonogenetic goiter).
Morphology:
- Follicles lined by crowded columnar cells (hyperplastic phase) or flattened cuboidal cells (involution/colloid phase)
- Cut surface: brown, gelatinous, translucent
Multinodular Goiter (MNG)
Virtually all long-standing diffuse goiters convert to MNG. The gland is lobulated, asymmetrically enlarged, and may reach massive size. Cut surface shows irregular nodules with variable colloid, fibrosis, hemorrhage, calcification, and cystic change. Patients are generally euthyroid but may develop secondary hyperthyroidism (Plummer disease/toxic MNG) or experience compressive symptoms (dysphagia, stridor, SVC obstruction).
2. Thyroiditis
| Type | Mechanism | Key Features | Outcome |
|---|---|---|---|
| Hashimoto | Autoimmune (anti-TPO, anti-Tg Abs) | Dense lymphocytic infiltrate, germinal centers, Hurthle cell change, hypothyroidism | Permanent hypothyroidism |
| Subacute Granulomatous (de Quervain) | Post-viral; neutrophils → macrophages/granulomas | Painful neck, fever, ESR↑, transient hyper then hypothyroid | Self-limited, 6-8 wks |
| Painless (Subacute Lymphocytic) | Autoimmune variant of Hashimoto | Painless goiter, lymphocytic infiltrate, transient thyrotoxicosis | Returns to euthyroid; minority progress to hypothyroidism |
| Riedel | IgG4-related disease | Dense fibrosclerosis extending beyond thyroid, rock-hard fixed mass, may mimic malignancy | May be hypothyroid |
PART II: BENIGN NEOPLASMS
Follicular Adenoma
The most common benign thyroid tumor. A solitary, spherical lesion enclosed by a well-defined, intact fibrous capsule - the hallmark feature that distinguishes it from follicular carcinoma.
Molecular Pathogenesis:
- Toxic adenoma: Gain-of-function mutations in the TSH receptor (TSHR) or the Gs-alpha subunit (GNAS) → constitutive TSH signaling → autonomous thyroid hormone secretion → hyperthyroidism
- Nonfunctioning adenoma: Mutations in RAS (<20%) and PTEN (shared with follicular carcinoma)
Morphology:
- Solitary, compresses adjacent thyroid
- Uniform follicles containing colloid, minimal mitoses
- Cells may show Hurthle (oxyphil) cell change
- Intact, complete capsule - mandatory criterion
Clinical Features:
- Most present as painless nodules
- Nonfunctioning: cold nodule on radionuclide scan (up to 10% of cold nodules are malignant)
- Toxic adenoma: warm/hot nodule, features of thyrotoxicosis
- FNA + ultrasound essential pre-operatively
- Surgically excised to evaluate capsular integrity
- Excellent prognosis; do not recur
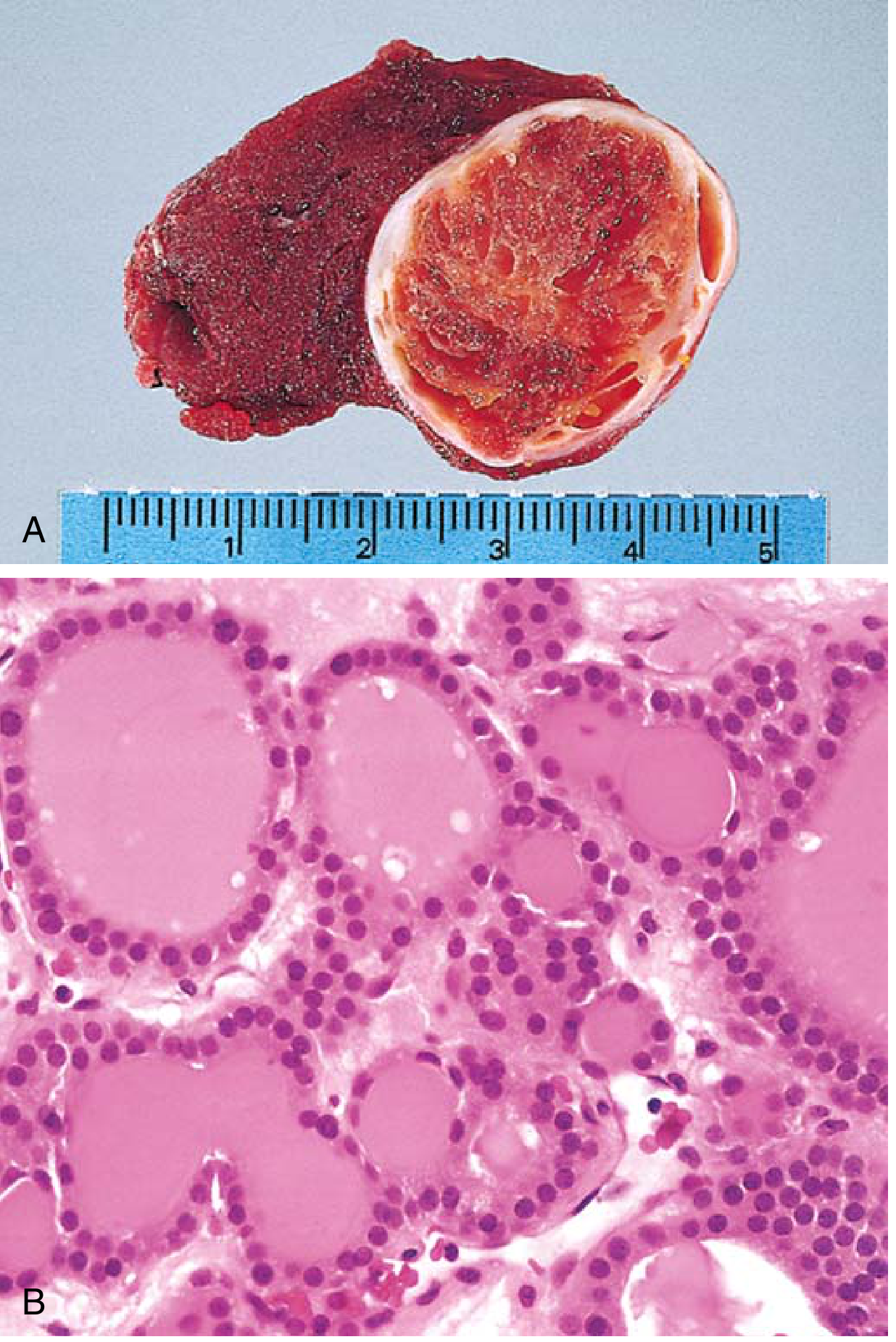
Fig. 18.10 - Follicular adenoma of the thyroid. (A) Solitary, well-circumscribed nodule. (B) Well-differentiated follicles with colloid.
PART III: MALIGNANT NEOPLASMS (Thyroid Carcinomas)
Most thyroid carcinomas (except MTC) are derived from follicular epithelium. Three follicular cell-derived malignancies all share constitutive activation of signaling pathways downstream of receptor tyrosine kinases.
Frequency Overview
| Type | Frequency | Cell of Origin |
|---|---|---|
| Papillary Thyroid Carcinoma (PTC) | >85% | Follicular epithelium |
| Follicular Thyroid Carcinoma (FTC) | 5-15% | Follicular epithelium |
| Anaplastic Carcinoma | <5% | Follicular epithelium (dedifferentiated) |
| Medullary Thyroid Carcinoma (MTC) | ~5% | Parafollicular C cells |
1. Papillary Thyroid Carcinoma (PTC)
Most common thyroid malignancy (>85%)
Molecular Pathogenesis (MAP kinase pathway activation):
- BRAF point mutation: 40-65% (most common single alteration)
- RAS mutations: 10-30%
- RET/NTRK gene fusions (translocations): 10-20%
- These are mutually exclusive - each one constitutively activates MAPK signaling
- Ionizing radiation (especially in first 2 decades of life) is a major risk factor; incidence surged among children after Chernobyl (1986)
Morphology:
- Solitary or multifocal; may be encapsulated or infiltrative
- Diagnostic nuclear hallmarks (sufficient even without papillary architecture):
- Branching papillae with fibrovascular stalks lined by cuboidal cells
- Ground-glass (Orphan Annie eye) nuclei - optically clear/empty due to finely dispersed chromatin
- Intranuclear pseudo-inclusions - cytoplasmic invaginations
- Intranuclear grooves
- Psammoma bodies - concentrically calcified structures in papillary cores (rarely in follicular or medullary carcinomas)
- Lymphatic invasion common; blood vessel invasion uncommon in smaller lesions
- Cervical lymph node metastasis in up to 50% of cases
Variants (>12 recognized):
- Encapsulated follicular variant (common; carries PAX8-PPARG fusion in ~1/3)
- Tall cell, columnar cell, diffuse sclerosing, oncocytic, hobnail, and others
Clinical Features:
- Usually a painless neck mass (within thyroid or as cervical node metastasis)
- Nonfunctional; FNA is diagnostic pre-operatively
- 10-year survival >95% - indolent course
- Isolated cervical node metastases do not significantly worsen prognosis
- Hematogenous metastasis to lungs in a minority
- Prognosis influenced by: age >40, extrathyroidal extension, distant metastases
2. Follicular Thyroid Carcinoma (FTC)
5-15% of thyroid cancers; F:M ratio 3:1; peak age 40-60 years
Molecular Pathogenesis (PI3K/AKT pathway):
- RAS mutations (shared with adenomas and anaplastic carcinoma)
- PIK3CA gain-of-function (encodes PI3K)
- PTEN loss-of-function (negative regulator of PI3K)
- PAX8-PPARG fusion [t(2;3)(q13;p25)] - found in up to 50%; PAX8 regulates thyroid development, PPARG governs terminal differentiation
- Iodine deficiency increases FTC risk; iodine-sufficient areas show stable/declining incidence
Morphology:
- Single nodule; may be well-circumscribed or widely infiltrative
- Grossly indistinguishable from follicular adenoma
- On microscopy: uniform cells forming small colloid-containing follicles
- Diagnosis of carcinoma requires demonstration of capsular and/or vascular invasion (requires extensive sampling of the tumor-capsule interface)
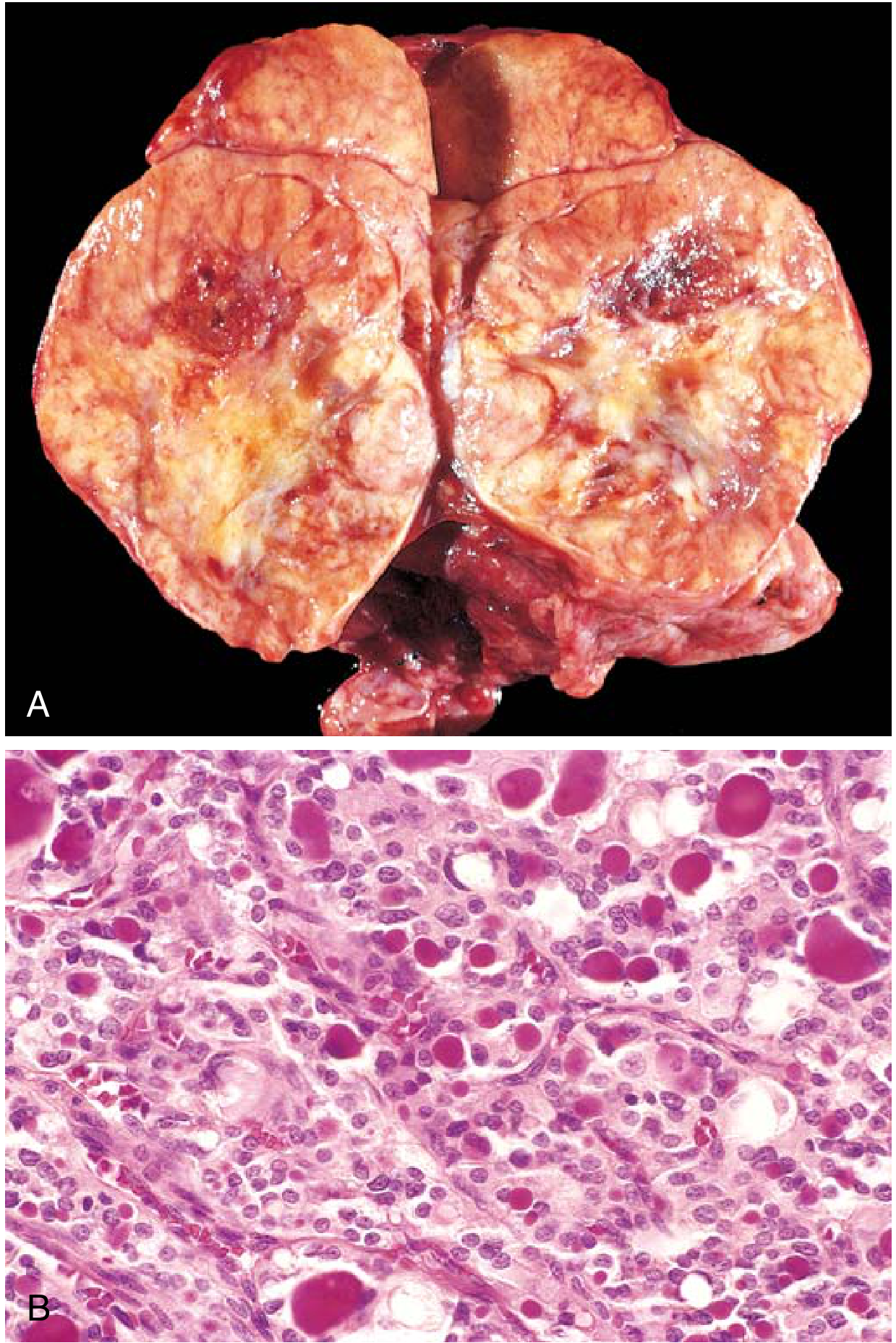
Fig. 18.13 - Follicular thyroid carcinoma. (A) Light-tan cut surface with hemorrhagic foci replacing the thyroid lobe. (B) Glandular lumens containing recognizable colloid.
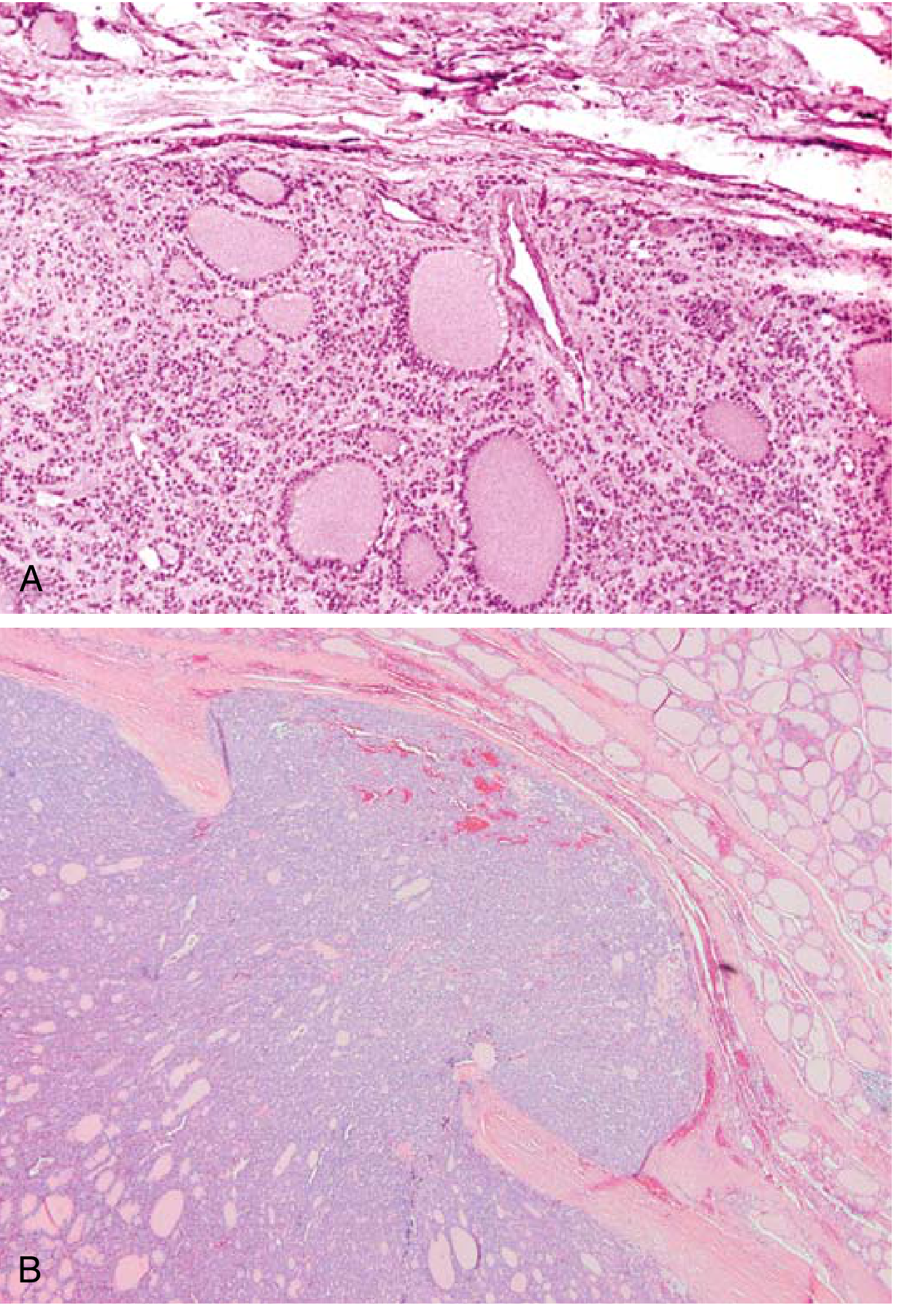
Fig. 18.14 - Capsular invasion. (A) Follicular adenoma with intact fibrous capsule and compressed normal parenchyma. (B) Follicular carcinoma showing capsular invasion (minimal here, may be widespread).
Subtypes by invasion:
- Minimally invasive FTC: Focal capsular ± vascular invasion; <10% die within 10 years
- Widely invasive FTC: Extensive invasion; ~50% die within 10 years
Clinical Features:
- Presents as solitary cold nodule
- Hematogenous spread (lungs, bone, liver) is characteristic - in contrast to PTC's lymphatic spread
- Regional lymph node metastasis is uncommon
- Rarely hyperfunctional
Hurthle Cell (Oncocytic) Carcinoma:
- A variant with brightly eosinophilic granular cytoplasm (oxyphil change)
- Worst survival among well-differentiated thyroid cancers
- Highest incidence of distant metastases among well-differentiated tumors
3. Anaplastic (Undifferentiated) Thyroid Carcinoma
<5% of thyroid cancers; most aggressive; near 100% mortality
Epidemiology: Mean age at diagnosis ~65 years; ~25% have a history of prior well-differentiated carcinoma; another ~25% harbor a concurrent well-differentiated tumor in the resected specimen.
Molecular Pathogenesis:
- Shares mutations with well-differentiated carcinomas (RAS, PIK3CA)
- Additional mutations unique to anaplastic carcinoma:
- TP53 loss-of-function (most important driver of dedifferentiation)
- Typically arises by progression/dedifferentiation from existing papillary or follicular carcinoma
Morphology:
- Bulky masses growing rapidly beyond the thyroid capsule into adjacent neck structures
- Microscopically: highly anaplastic cells - large and pleomorphic, or spindle-shaped, or a mixture
- Foci of papillary/follicular differentiation may be present (pointing to origin)
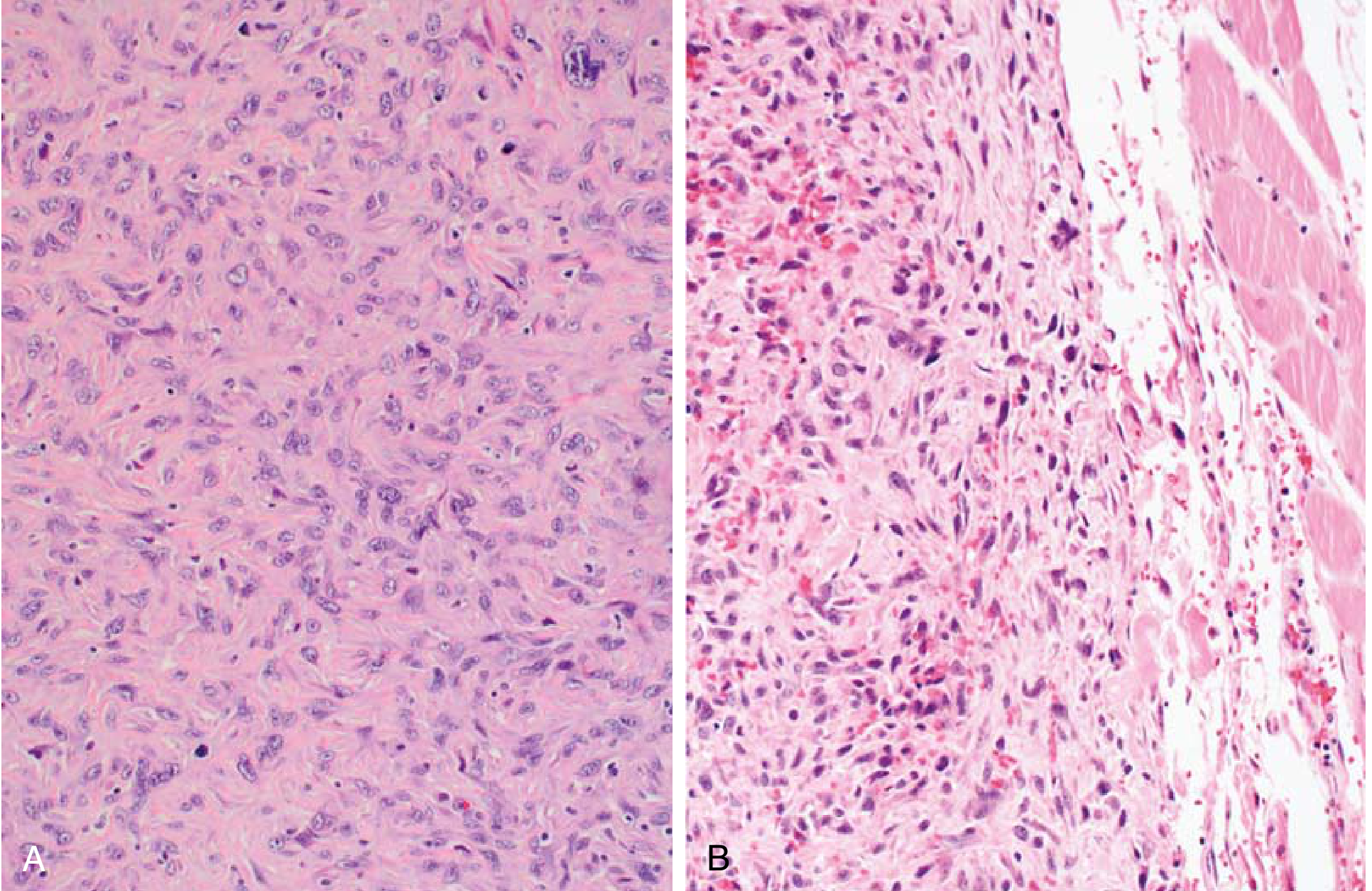
Fig. 18.15 - Anaplastic thyroid carcinoma. (A) Highly pleomorphic epithelioid and spindle cells. (B) Spindle cells infiltrating adjacent skeletal muscle.
Clinical Features:
- Rapid growth, invading vital neck structures
- Distant metastases common
- Death in most cases within 1 year due to aggressive local extension
- Unresponsive to most conventional therapies; BRAF-targeted therapy (dabrafenib + trametinib) used for BRAF V600E-mutated tumors
4. Medullary Thyroid Carcinoma (MTC)
~5% (some sources ~3%) of thyroid cancers; arises from parafollicular C cells
Unique biology:
- C cells are of neuroectodermal origin, located mainly in the lateral superior thyroid poles
- Secrete calcitonin (diagnostic and surveillance marker), CEA, serotonin, somatostatin, VIP, histaminidases, prostaglandins
Genetics/Etiology:
- Sporadic (70%): Unifocal; acquired RET mutations in ~50%; peak age 50-60 years; M = F
- Familial (30%): Germline RET mutations; autosomal dominant, ~100% penetrance; multicentric and bilateral in 90%
- Familial MTC alone (no associated endocrinopathy)
- MEN-2A: MTC + pheochromocytoma + primary hyperparathyroidism
- MEN-2B: MTC + pheochromocytoma + mucosal neuromas + Marfanoid habitus (most aggressive; MTC can appear in first year of life)
Morphology:
- Solid, firm, gray, nonencapsulated but well-circumscribed
- Polygonal to spindle-shaped cells in nests, trabeculae, or glandlike structures
- Amyloid deposits in stroma (derived from altered calcitonin molecules) - a distinctive feature
- Familial MTC: multicentric C-cell hyperplasia in surrounding parenchyma (precursor lesion)
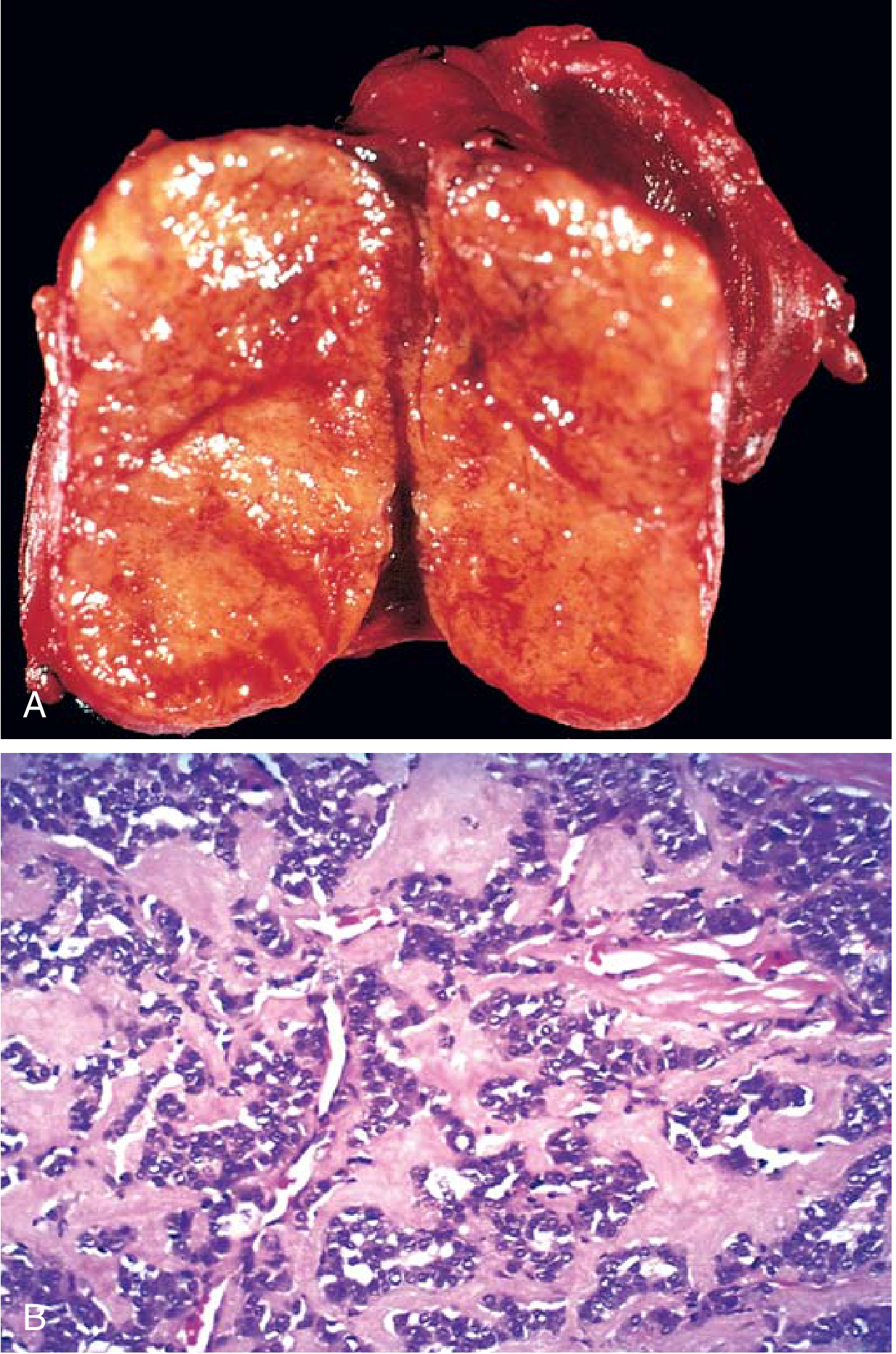
Fig. 18.16 - Medullary thyroid carcinoma. (A) Solid mass without fibrous capsule. (B) Abundant amyloid as homogeneous pink extracellular material.
Clinical Features:
- Neck mass ± cervical lymphadenopathy (palpable nodes in ≤20%)
- Local invasion symptoms: dysphagia, dyspnea, dysphonia
- Diarrhea/flushing from VIP or serotonin secretion
- Distant metastases in 50% at diagnosis (mediastinum, liver, lung, bone)
- Does NOT respond to radioiodine or TSH suppression (C cell origin)
Workup:
- Serum calcitonin + CEA
- RET mutation testing in all patients
- Screen for pheochromocytoma (24-hr urinary catecholamines/metanephrines + abdominal MRI)
- Screen for hyperparathyroidism (serum calcium)
Treatment:
- Total thyroidectomy + bilateral central neck dissection (level VI, VII)
- Lateral neck dissection for palpable nodes or elevated calcitonin (ipsilateral if >20 pg/mL, bilateral if >200 pg/mL)
- Targeted therapy for advanced disease: vandetanib or cabozantinib (RET inhibitors); newer RET-selective inhibitors (selpercatinib, pralsetinib) under study
COMPARATIVE SUMMARY TABLE
| Feature | PTC | FTC | Anaplastic | MTC |
|---|---|---|---|---|
| Frequency | >85% | 5-15% | <5% | ~5% |
| Cell origin | Follicular epithelium | Follicular epithelium | Follicular epithelium | Parafollicular C cells |
| Key mutation | BRAF V600E (40-65%) | PAX8-PPARG, RAS, PIK3CA | TP53 + RAS/PIK3CA | RET (germline/somatic) |
| Spread | Lymphatic (cervical LN) | Hematogenous (lung, bone) | Local invasion + distant | Both; 50% distant at dx |
| Marker | Thyroglobulin | Thyroglobulin | None specific | Calcitonin, CEA |
| Psammoma bodies | Yes | No | No | No |
| Radioiodine response | Yes | Yes | No | No |
| 10-year survival | >95% | ~85% (minimal inv.) | <5% | 70-80% (sporadic) |
| Familial association | Rare | Rare | None | 30% (MEN-2A/2B) |
BETHESDA SYSTEM (FNA Cytology Classification)
FNA is the primary diagnostic tool for thyroid nodules and uses the Bethesda System for Reporting Thyroid Cytopathology:
| Category | Description | Malignancy Risk | Management |
|---|---|---|---|
| I | Non-diagnostic/Unsatisfactory | N/A | Repeat FNA |
| II | Benign | ~0-3% | Clinical follow-up |
| III | Atypia of Undetermined Significance (AUS/FLUS) | ~10-30% | Repeat FNA or molecular testing |
| IV | Follicular Neoplasm / Suspicious for FN | ~25-40% | Surgical lobectomy |
| V | Suspicious for Malignancy | ~50-75% | Near-total thyroidectomy or lobectomy |
| VI | Malignant | ~97-99% | Total thyroidectomy |
ULTRASOUND RISK CLASSIFICATION (TI-RADS / ATA)
Features suggesting malignancy (in decreasing specificity):
- Hypoechogenicity / marked hypoechogenicity
- Microcalcifications (psammoma bodies)
- Irregular margins / infiltrative borders
- Taller-than-wide shape on transverse view
- Extrathyroidal extension
Features suggesting benign nodule:
- Purely cystic lesion
- Spongiform appearance (honeycomb pattern)
- Isoechoic/hyperechoic with smooth margins
- Comet-tail artifact (colloid crystals)
- Hot on radionuclide scan
Recent literature note: A 2024 review (PMID: 38672067) discusses updates to the WHO 2022 classification of thyroid tumors, including recognition of low-risk encapsulated follicular variant PTC as "non-invasive follicular thyroid neoplasm with papillary-like nuclear features" (NIFTP) - a borderline entity with essentially benign behavior that should be distinguished from invasive carcinoma.
- Robbins & Kumar Basic Pathology, Chapter 18 (Endocrine System)
- Cummings Otolaryngology Head and Neck Surgery, Chapter 28
- Fischer's Mastery of Surgery, 8th ed., Chapter on Well-Differentiated Thyroid Carcinoma
Give me all details about thyroid lesion
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
This is a comprehensive, multi-textbook reference on all thyroid lesions. Here is a summary of what was covered:
What Was Covered
The answer spans 10 major sections drawing from 5 authoritative textbooks (Robbins Pathologic Basis of Disease, Robbins Basic Pathology, Sabiston Surgery, Cummings Otolaryngology, and Scott-Brown's Otorhinolaryngology):
-
Normal thyroid anatomy and physiology - HPT axis, hormone synthesis, TSH signaling (with diagram)
-
Complete classification tree - All lesions from non-neoplastic to malignant, including the 2022 WHO updates
-
Non-neoplastic lesions in full detail:
- Diffuse and multinodular goiter (endemic vs sporadic)
- Hashimoto thyroiditis (with pathogenesis diagram and histology image)
- Graves disease (triad, TSI mechanism, treatment)
- de Quervain, painless/postpartum, and Riedel thyroiditis
-
Follicular adenoma - toxic vs nonfunctioning, molecular genetics, hot/cold nodule distinction
-
WHO 2022 borderline entities - NIFTP, HTT, UMP
-
All 6 malignant subtypes with morphology images, molecular alterations, spread patterns, prognosis, and targeted therapies - PTC (with Orphan Annie eye nuclei image), FTC (capsular invasion), OCA (new WHO 2022 term), PDTC, ATC (anaplastic), MTC (amyloid, RET/MEN-2)
-
Thyroid nodule evaluation - red flags, ATA risk stratification, FNA thresholds (with algorithm flowchart)
-
Bethesda System (Bethesda I-VI) with malignancy risks
-
AJCC 8th edition staging for DTC
-
Complete comparative summary table across all 6 malignant types
This is a shared conversation. Sign in to Orris to start your own chat.