ECG findings for usmle
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Now I have comprehensive material to write a thorough USMLE-focused ECG review. Let me compile it all.
ECG Findings for USMLE - High-Yield Review

Normal ECG Intervals
From Goldman-Cecil Medicine (Table 42-1):
| Parameter | Normal Value |
|---|---|
| Heart rate | 50-100 bpm |
| P wave duration | <0.12 sec (120 ms) |
| PR interval | 0.09-0.20 sec (90-200 ms) |
| QRS duration | 0.075-0.11 sec (75-110 ms) |
| QTc (male) | 390-450 ms |
| QTc (female) | 390-460 ms |
| QRS axis | -30 to +90 degrees |
Paper speed: 25 mm/sec - each small box (1 mm) = 0.04 sec; each big box (5 mm) = 0.2 sec.
Basic Waveform Meanings
| Wave/Segment | Represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | Conduction through atria + AV node + His-Purkinje to ventricles |
| QRS complex | Ventricular depolarization |
| ST segment | Plateau of ventricular action potential (isoelectric) |
| T wave | Ventricular repolarization |
| QT interval | First ventricular depolarization to last ventricular repolarization |
| J (Osborn) wave | Positive deflection at J point - seen in hypothermia, hypercalcemia, brain injury |
Note: Atrial repolarization is not visible on a normal ECG - it is buried underneath the QRS.
High-Yield ECG Findings by Condition
Ischemia / Infarction
| Finding | Interpretation |
|---|---|
| ST elevation in 2 contiguous leads | STEMI - transmural ischemia, acute injury |
| ST depression | Subendocardial ischemia (NSTEMI/UA) or posterior MI (ST elevation in V1-V2 = posterior MI) |
| T wave inversion | Ischemia or ventricular strain |
| Pathologic Q waves (>0.04 sec wide, >1/3 of R height) | Old/completed MI - irreversible necrosis |
| New LBBB | STEMI equivalent - treat as acute MI |
| Hyperacute T waves | Very early STEMI (first minutes) |
STEMI localization:
- Inferior (II, III, aVF) - RCA
- Lateral (I, aVL, V5-V6) - LCx
- Anterior (V1-V4) - LAD
- Posterior (ST depression + tall R in V1/V2, confirmed by ST elevation in V7-V9) - RCA/LCx
AV Blocks
| Block | ECG Finding |
|---|---|
| 1st degree AV block | PR > 200 ms, every P conducts |
| 2nd degree - Mobitz I (Wenckebach) | Progressive PR prolongation until a P wave is dropped (P not followed by QRS); benign |
| 2nd degree - Mobitz II | Fixed PR interval with sudden dropped QRS; often needs pacemaker |
| 3rd degree (complete) AV block | P waves and QRS complexes march independently; regular P-P and R-R but no relationship between them |
Bundle Branch Blocks (QRS ≥ 0.12 sec)
RBBB: "WiLLiaM MaRRoW" - in V1, W pattern (rSR'); in V6, M pattern.
- Wide QRS with rSR' ("rabbit ears") in V1
- Wide S wave in V5-V6
- Discordant T waves in right precordial leads
- Can be normal variant
LBBB: "WiLLiaM MaRRoW" - in V1, W pattern; in V6, M pattern (broad, notched R).
- Wide QRS with broad, notched R in I, aVL, V5-V6
- Deep S in V1-V2
- Discordant ST/T throughout precordium
- Never a normal variant - always pathologic; in acute chest pain = STEMI equivalent
Axis deviations:
- Left axis deviation (-30 to -90°): LBBB, inferior MI, left anterior fascicular block (LAFB), LVH
- Right axis deviation (+90 to +180°): RBBB, RVH, left posterior fascicular block (LPFB), PE, dextrocardia
Hypertrophy
| Finding | Meaning |
|---|---|
| LVH (Cornell voltage): S in V3 + R in aVL ≥ 28 mm (men), ≥ 20 mm (women) | Left ventricular hypertrophy (HTN, AS, HCM) |
| RVH: R > S in V1, right axis deviation, ST depression in V1-V3 | Cor pulmonale, pulmonary HTN, PE |
| Left atrial enlargement: P wave > 0.12 sec, biphasic P in V1 (deep negative terminal component) | Mitral stenosis, HTN |
| Right atrial enlargement (P pulmonale): tall, peaked P wave > 2.5 mm in II | Cor pulmonale, tricuspid stenosis |
Arrhythmias
| Arrhythmia | ECG Finding |
|---|---|
| Sinus tachycardia | HR >100, normal P before each QRS |
| Atrial fibrillation | Irregularly irregular, no P waves, fibrillatory baseline |
| Atrial flutter | Sawtooth flutter waves at ~300/min, ventricular rate usually 150 (2:1 block) |
| AVNRT (SVT) | Narrow-complex tachycardia, rate 150-250; P buried in or just after QRS |
| Ventricular tachycardia | Wide-complex tachycardia (QRS > 0.12 sec), rate >100, AV dissociation, fusion beats, capture beats |
| Ventricular fibrillation | Chaotic, no organized rhythm - cardiac arrest |
| Torsades de pointes | Polymorphic VT, twisting QRS axis, associated with long QT |
Wolff-Parkinson-White (WPW)
ECG triad during sinus rhythm (Tintinalli):
- PR interval < 120 ms (short PR)
- Delta wave - slurred upstroke of QRS
- Slightly widened QRS
Associated tachycardias:
- Orthodromic AVRT (65%): narrow QRS, regular, rate 160-220
- Antidromic AVRT (5-10%): wide QRS, looks like VT
- Atrial fibrillation with WPW (25%): wide, bizarre, irregular QRS at rate >200 - life-threatening; do NOT give AV nodal blockers (adenosine, beta-blockers, CCBs, digoxin)
Electrolyte Abnormalities
Hyperkalemia - progressive changes with rising K+:
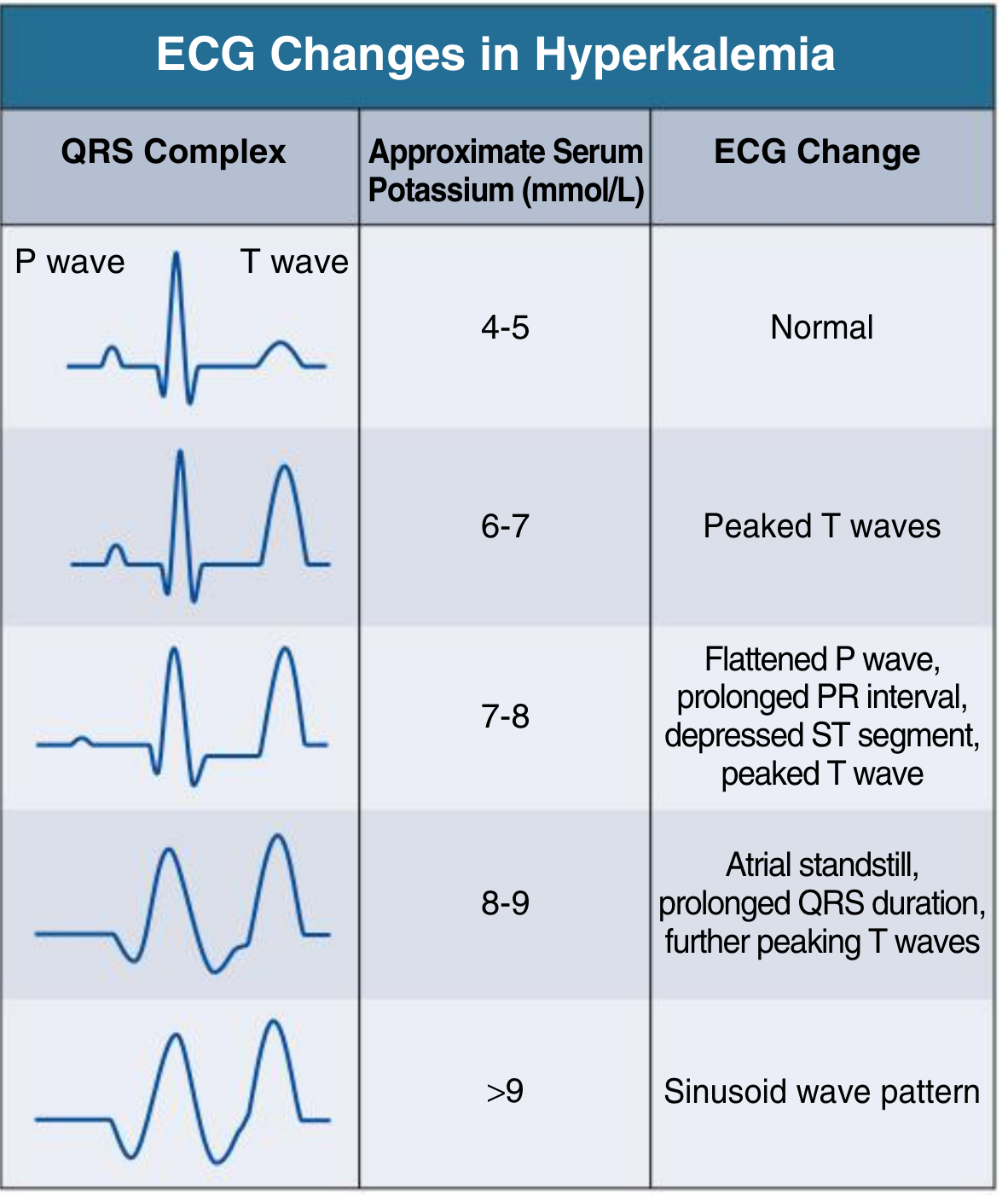
| K+ (mmol/L) | ECG Change |
|---|---|
| 4-5 | Normal |
| 6-7 | Peaked (tented) T waves - earliest finding |
| 7-8 | Flat P wave, prolonged PR, depressed ST |
| 8-9 | Atrial standstill, wide QRS |
| >9 | Sine wave pattern → VF |
Hypokalemia:
- Flattened/inverted T waves
- Prominent U wave (appearing after T wave, especially in V2-V3)
- Prolonged QU interval
- ST depression
Hypercalcemia: Short QT interval
Hypocalcemia: Long QT interval
Pericarditis
- Diffuse ST elevation (concave/saddle-shaped) in nearly all leads
- PR depression (very specific for pericarditis - opposite of ST change)
- No reciprocal changes (unlike STEMI)
- Evolves through 4 stages
Long QT Syndrome
- QTc > 450 ms (men) / 460 ms (women)
- Risk of Torsades de pointes and sudden death
- Causes: drugs (quinidine, sotalol, amiodarone, macrolides, antipsychotics), electrolytes (hypo-K, hypo-Mg, hypo-Ca), congenital (Romano-Ward, Jervell-Lange-Nielsen)
Pulmonary Embolism
Classic (but insensitive) ECG finding: S1Q3T3
- S wave in lead I
- Q wave in lead III
- T wave inversion in lead III
- Also: sinus tachycardia (most common), right heart strain (RVH, RBBB, RAD)
Digitalis Toxicity
- "Scooping" (reverse tick) ST depression - characteristic shape
- Shortened QT interval (therapeutic level)
- Toxicity: PVCs, heart blocks (especially 2nd/3rd degree), junctional rhythms, bidirectional VT
Quick Summary Table for USMLE
| Condition | Key ECG Mnemonic/Finding |
|---|---|
| STEMI | ST elevation + reciprocal ST depression |
| Old MI | Q waves in territory |
| Pericarditis | Diffuse ST elevation + PR depression |
| 1° AV block | Long PR (>200 ms) |
| Mobitz I | "Longer, longer, longer...DROP" (PR) |
| Mobitz II | Fixed PR, sudden drop |
| Complete block | P and QRS march independently |
| WPW | Short PR + delta wave |
| AFib | Irregularly irregular, no P waves |
| Atrial flutter | Sawtooth @ 300, rate 150 (2:1) |
| Hyperkalemia | Peaked T → wide QRS → sine wave |
| Hypokalemia | Flat T + prominent U wave |
| Long QT | Torsades |
| PE | S1Q3T3 (+ sinus tach) |
| Hypothermia | J (Osborn) waves |
| Digoxin effect | Scooping ST depression |
Sources: Costanzo Physiology 7e, Goldman-Cecil Medicine 15e, Tintinalli's Emergency Medicine, Comprehensive Clinical Nephrology 7e
This is a shared conversation. Sign in to Orris to start your own chat.