A 28-year-old married Nulliparous woman presents to gynecology OPD with chronic pelvic pain and dyspareunia. She also experiences severe dysmenorrhea starting two days before menstruation and lasting for first three days of the cycle. She is undergoing treatment for primary infertility. Diagnose the condition. Describe its clinical features in detail.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
I now have all the content needed for a thorough answer. Let me compile the comprehensive response.
Diagnosis: Endometriosis
This 28-year-old nulliparous woman presents with the classic triad of endometriosis:
- Secondary dysmenorrhea - starting 2 days before menstruation and persisting through the first 3 days of the cycle
- Deep dyspareunia - pain during intercourse
- Chronic pelvic pain
- Primary infertility (the presenting complaint in 30-40% of women with endometriosis)
Definition
Endometriosis is defined as the presence of endometrial-like tissue (glands and/or stroma) outside the uterus. It is a common, estrogen-dependent, chronic inflammatory condition affecting approximately 10% of women of reproductive age. The condition varies from a few minimal peritoneal lesions to deep infiltrating nodules and massive ovarian cysts with extensive adhesions causing significant distortion of pelvic anatomy.
- Berek & Novak's Gynecology, p. 617
- Robbins & Kumar Pathologic Basis of Disease, p. 2754
Clinical Features in Detail
1. Pain Symptoms
Dysmenorrhea (Most Common Symptom)
- The hallmark feature. Secondary dysmenorrhea in endometriosis classically starts before the onset of menstrual bleeding and continues throughout the period - exactly as in this patient (2 days pre-menstrual onset, lasting 3 days into the cycle).
- It may begin after years of pain-free menses (distinguishing it from primary dysmenorrhea), though in adolescents it may be present from menarche.
- The pain is typically bilateral and may radiate to the lower back, thighs, and rectum.
- Berek & Novak's Gynecology, p. 628
Dyspareunia (Deep)
- A highly characteristic symptom, described as deep dyspareunia - pain felt deep in the pelvis rather than at the introitus.
- It is caused by endometriotic deposits in the uterosacral ligaments, posterior cul-de-sac, or rectovaginal septum.
- There is a strong association between posterior cul-de-sac lesions and dyspareunia.
- Berek & Novak's Gynecology, p. 628-629
Chronic Pelvic Pain (Non-menstrual)
- Constant or intermittent pelvic pain unrelated to the menstrual cycle.
- Results from intrapelvic bleeding, periuterine adhesions, and the release of inflammatory mediators (prostaglandins, cytokines).
- All endometriosis lesion types - including minimal to mild disease - are associated with pelvic pain.
- Robbins & Kumar, p. 2765
Dyschezia (Painful Defecation)
- Pain on opening the bowels, particularly during menstruation, due to endometriotic deposits on the bowel serosa, rectovaginal septum, or uterosacral ligaments.
- Deep lesions are consistently associated with gastrointestinal symptoms and painful defecation.
- Bailey and Love's Surgery, p. 1602
Other Pain Manifestations
- Lower back pain
- Dysuria and hematuria if bladder involvement
- Cyclic shoulder tip pain if diaphragmatic involvement
- Cyclic hemoptysis or pneumothorax if pulmonary (rare)
2. Menstrual Abnormalities
- Menstrual irregularities are common.
- Premenstrual spotting may occur.
- Heavy menstrual bleeding (menorrhagia) in some cases.
- Associated with luteinized unruptured follicle syndrome, anovulation, and hyperprolactinemia.
- Berek & Novak's Gynecology, p. 629
3. Infertility
Infertility is the presenting complaint in 30-40% of women with endometriosis.
Mechanisms of infertility include:
- Distorted pelvic anatomy with adhesions - interference with tubal pick-up of the oocyte
- Altered peritoneal environment - increased macrophages, cytokines, prostaglandins in peritoneal fluid that are toxic to sperm and embryos
- Endocrine/ovulatory abnormalities - impaired folliculogenesis, abnormal LH surge, luteal phase defects
- Immunological factors - increased autoantibodies to endometrial antigens
- Endometriomas compressing normal ovarian cortex and reducing ovarian reserve
- Fallopian tube involvement impeding ovum transport
The infertility is thought to reflect involvement of fallopian tubes and the peritoneal environment rather than a single mechanism.
- Berek & Novak's Gynecology, pp. 625-626
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 299
4. Gastrointestinal and Urinary Symptoms
- Nausea, vomiting, bloating, early satiety, altered bowel habits (cyclic)
- Cyclic rectal bleeding, constipation, or obstruction if bowel involvement
- Dysuria, urinary frequency, or hematuria if bladder/ureteral involvement
- Berek & Novak's Gynecology, p. 628
5. Physical Examination Findings
In many women, especially with minimal-mild disease, examination may be entirely normal. The classic findings in more severe disease include:
| Finding | Significance |
|---|---|
| Uterosacral / cul-de-sac nodularity | Palpable tender nodules along the uterosacral ligaments on rectovaginal exam - pathognomonic when present |
| Fixed retroverted uterus | Advanced disease with posterior adhesions; reduced uterine mobility ("frozen pelvis") |
| Lateral/cervical displacement | Due to uterosacral scarring |
| Adnexal mass/tenderness | Ovarian endometrioma (chocolate cyst), often densely adherent |
| Painful swelling of rectovaginal septum | Deep infiltrating endometriosis |
| Pinpoint cervical ostium | Associated risk factor |
| Blue-domed lesions in posterior fornix | Deep lesions growing into the vagina, visible on speculum examination |
| Tenderness on bimanual examination | Particularly in the posterior pelvis |
- Berek & Novak's Gynecology, pp. 630-631
Key point: The severity of pain does NOT correlate well with the extent/stage of disease. Women with minimal lesions may have severe pain, while some with extensive endometriomas may be nearly asymptomatic.
6. Extra-pelvic Manifestations
Endometriosis can occur at virtually any site, with symptoms appearing in a cyclical pattern:
- Intestinal tract (colon) - most common extra-pelvic site: abdominal/back pain, cyclic rectal bleeding, obstruction
- Urinary tract (ureter/bladder): dysuria, hematuria, ureteral obstruction
- Diaphragm: cyclic shoulder tip pain
- Lung/pleura: hemoptysis, pneumothorax, hemothorax during menses (catamenial pneumothorax)
- Umbilicus: palpable mass with cyclic pain
- Scars (e.g., episiotomy, Caesarean section scars): palpable nodule with cyclic pain
- Berek & Novak's Gynecology, p. 629
7. Macroscopic Pathology / Laparoscopic Appearance
Lesions appear in multiple forms:
- Classic "powder burn" or "gunshot" lesions: black, dark brown, or bluish puckered nodules containing old hemorrhage
- Red implants: petechial, vesicular, polypoid, "red flame-like" - active early lesions
- White/clear lesions: serous/clear vesicles, white plaques, fibrotic scarring
- Endometriomas ("chocolate cysts"): ovarian cysts 3-5 cm filled with thick dark brown fluid (old blood), densely adherent to peritoneum
- Deep infiltrating endometriosis (DIE): tissue >5 mm beneath the peritoneum, in uterosacral ligaments, vagina, bowel, bladder, or ureters
Widespread disease causes extensive fibrous adhesions, obliteration of the pouch of Douglas, and distortion of pelvic anatomy.
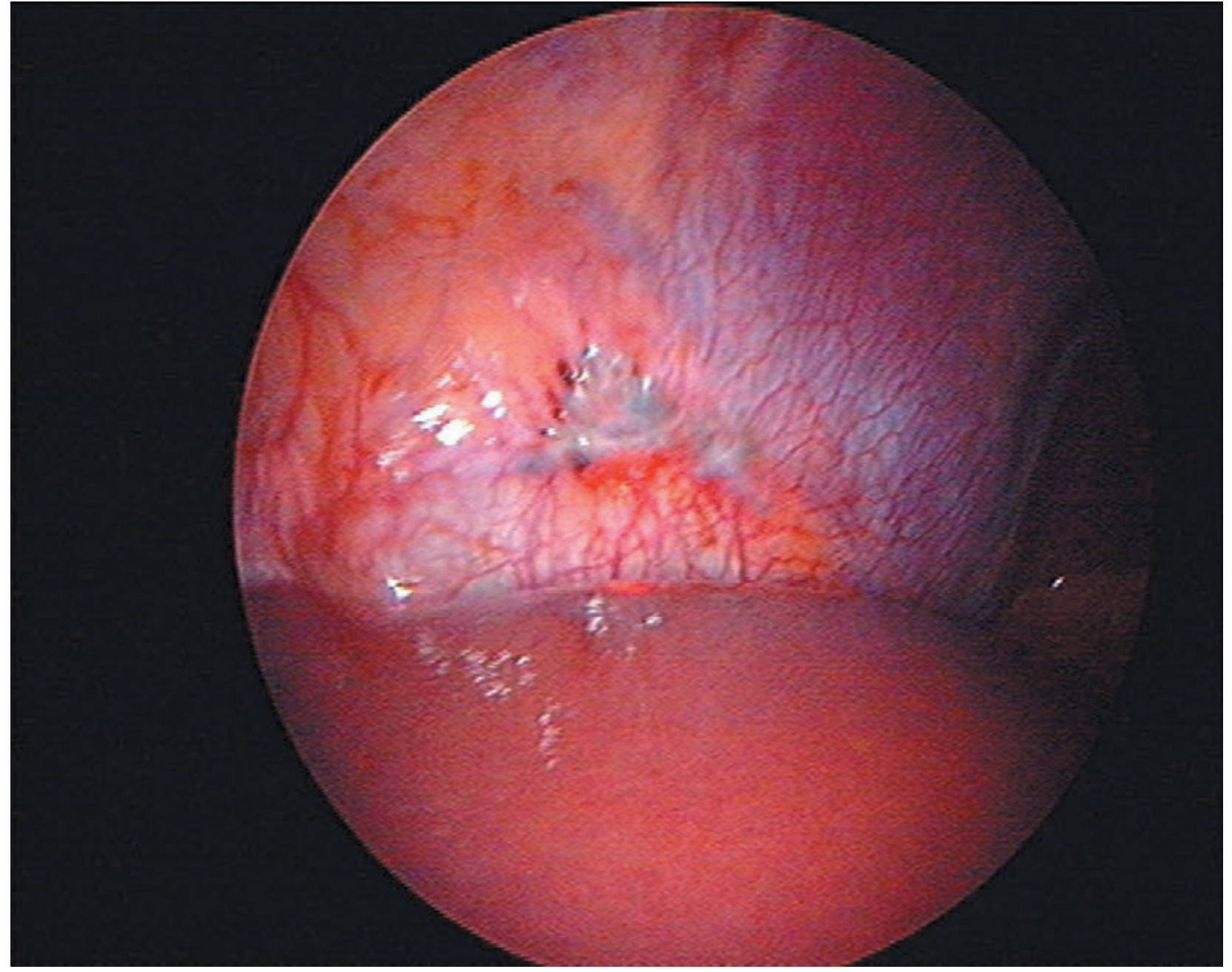
Endometriosis on the peritoneal surface - diaphragm (Bailey & Love)
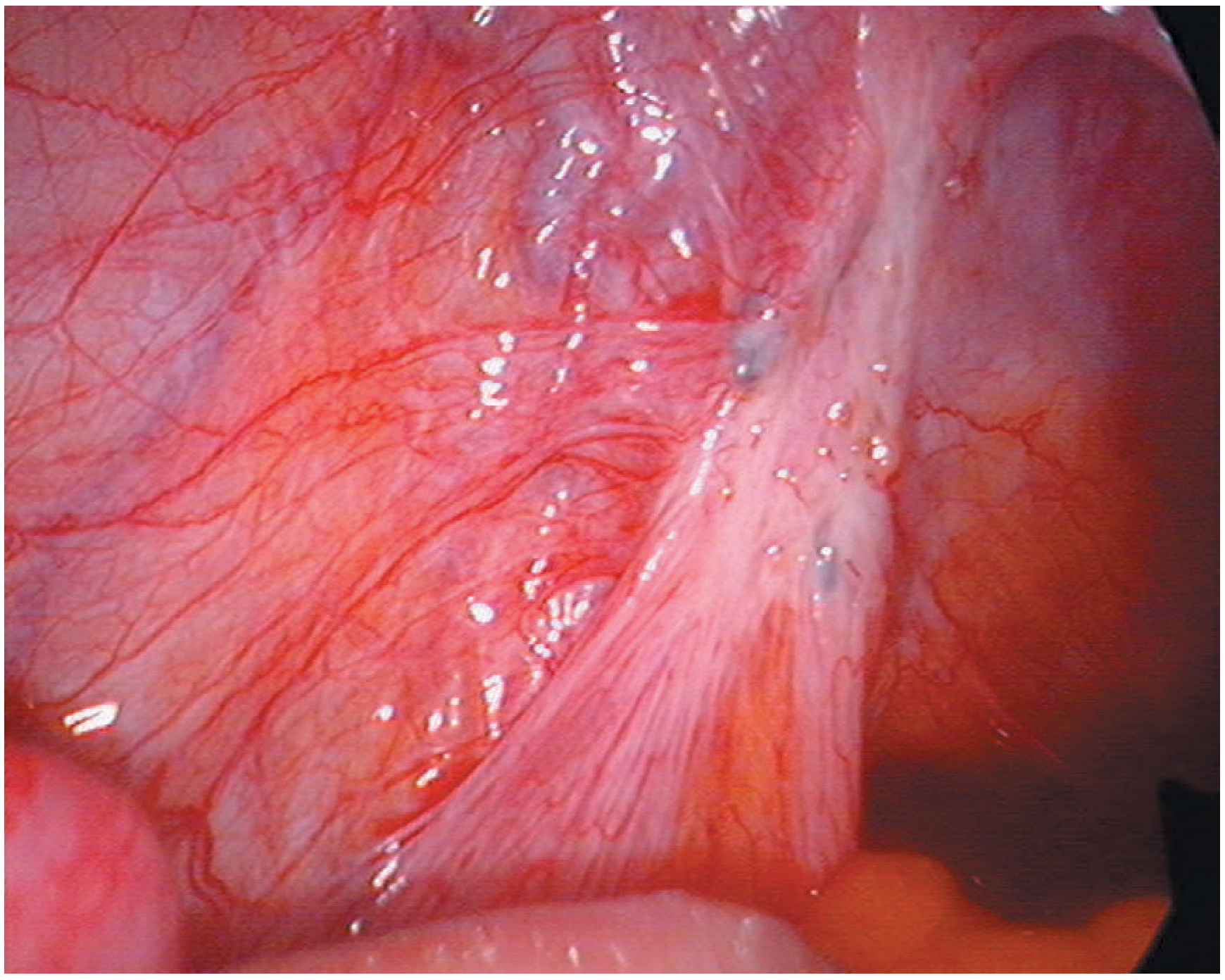
Endometriosis on the uterosacral ligament (Bailey & Love)
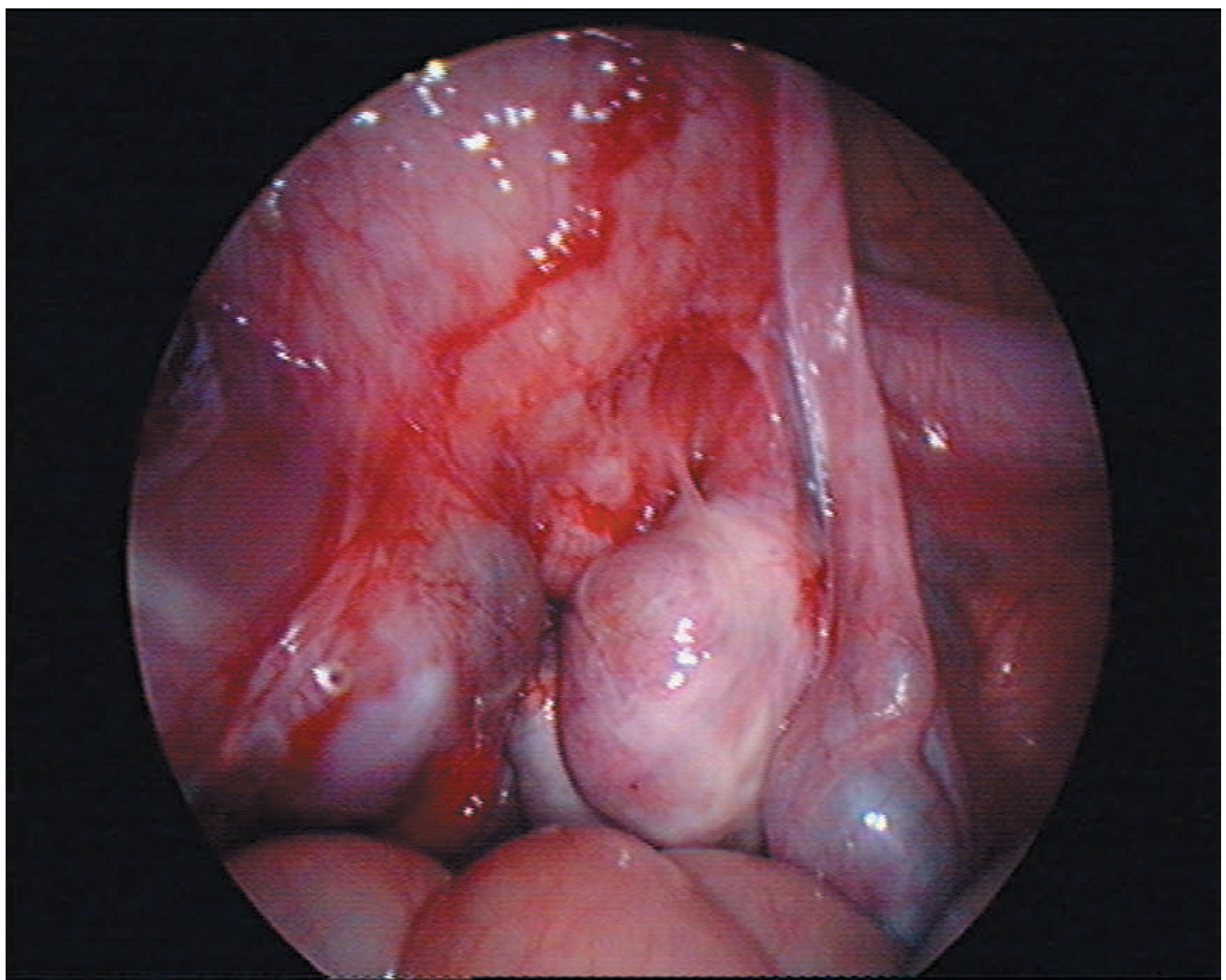
Bilateral ovarian endometriosis with pelvic adhesions (Bailey & Love)
- Bailey and Love's Surgery, pp. 1602-1603
- Robbins & Kumar, p. 2754
8. Histology
Diagnosis requires identification of:
- Endometrial glands AND stroma outside the uterus
- With or without hemosiderin (evidence of prior bleeding)
- In long-standing cases, secondary fibrosis may obscure the tissue
- Atypical endometriosis (cytologic atypia) is a precursor to endometrioid and clear cell ovarian carcinoma
- Robbins & Kumar, p. 2756-2758
Staging (ASRM Classification)
The American Society for Reproductive Medicine (ASRM) classifies endometriosis into 4 stages based on laparoscopic findings (peritoneal implants, ovarian endometriomas, adhesions, cul-de-sac obliteration):
| Stage | Description |
|---|---|
| I - Minimal | Few superficial implants |
| II - Mild | More/deeper implants |
| III - Moderate | Endometriomas, filmy adhesions |
| IV - Severe | Large endometriomas, dense adhesions, obliterated cul-de-sac |
Important caveat: ASRM staging correlates poorly with pelvic pain severity or infertility prognosis. The Endometriosis Fertility Index (EFI) better predicts non-IVF pregnancy rates after surgical treatment.
Epidemiological Risk Factors in this Patient
This patient fits the classic epidemiological profile:
- Reproductive age (peak incidence 25-35 years)
- Nulliparity - "career women" or delayed childbearing
- Family history - 7x increased risk if first-degree relative affected
- The average delay between symptom onset and diagnosis is 8-12 years due to symptom overlap with other conditions
Diagnosis Confirmation
-
Gold standard: Laparoscopy with histological confirmation - the definitive diagnostic procedure
-
Transvaginal ultrasound (TVUS): reliably detects endometriomas and severe pelvic disease; cannot detect peritoneal implants
-
MRI: detects hemosiderin deposits suggesting deep endometriosis
-
Serum CA-125: elevated in moderate-severe disease (13-95 U/mL) but of limited diagnostic value compared to laparoscopy
-
Empiric treatment with hormonal therapy may be justified without laparoscopy in women with classic symptoms
-
Berek & Novak's Gynecology, pp. 633-634
-
Bailey and Love's Surgery, pp. 1603-1604
Summary: This patient's classic triad of pre-menstrual onset secondary dysmenorrhea, deep dyspareunia, chronic pelvic pain, and primary infertility in a nulliparous woman of reproductive age is the textbook presentation of endometriosis. Definitive diagnosis requires diagnostic laparoscopy with histological confirmation of endometrial glands/stroma at ectopic sites.
This is a shared conversation. Sign in to Orris to start your own chat.