Create a detailed information about the 1 defibrillator 2 ICU care bundle 3 Pacemaker 4 infusion pump including types, uses , placement, indications, contra indications including images
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
defibrillator types uses indications contraindications placement ICU care bundle pacemaker infusion pump medical
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
ICU care bundle components ventilator central line CLABSI sepsis bundle 2024
Reading Web Page
https://nsccm.org.np/protocols/show-content/icu-protocol/icu…
Searching the Web
infusion pump types syringe pump volumetric pump PCA pump uses indications contraindications medical
Reading File
Reading Web Page
https://www.trivitron.com/blog/what-are-infusion-and-syringe…
Searching the Web
defibrillator types AED ICD manual placement pads indications contraindications image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Here is a detailed, well-organized reference covering all four topics:
1. DEFIBRILLATOR
What Is a Defibrillator?
A defibrillator is a medical device that delivers a controlled electric shock to the heart to depolarize a critical mass of myocardial cells simultaneously, allowing the heart's natural pacemaker to re-establish a normal rhythm. It is used specifically when the heart is in a life-threatening arrhythmia - ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT).
Types of Defibrillators
| Type | Description |
|---|---|
| AED (Automated External Defibrillator) | Semi- or fully automated; analyzes rhythm and delivers shock without specialist input. Found in airports, malls, public spaces. |
| Manual External Defibrillator | Requires trained clinician to interpret ECG and manually select energy level and deliver shock. Standard in hospitals, ED, ICU. |
| Advanced Life Support (ALS) Defibrillator | Combines manual defibrillation with cardiac monitoring, cardioversion, pacing capability. |
| Implantable Cardioverter-Defibrillator (ICD) | Surgically placed inside the chest. Continuously monitors rhythm and delivers internal shocks when life-threatening arrhythmia is detected. |
| Wearable Cardioverter-Defibrillator (WCD) | External vest worn by patient at high risk while waiting for ICD implantation. |
Indications
- Ventricular fibrillation (VF) - primary indication
- Pulseless ventricular tachycardia (pVT)
- Synchronized cardioversion for: atrial fibrillation, atrial flutter, SVT with hemodynamic compromise, stable VT
- ICD indications (Class I):
- Hemodynamically unstable VT/VF with no reversible cause
- Ischemic cardiomyopathy + NYHA II-III + LVEF ≤ 35% (at least 40 days post-MI)
- Non-ischemic dilated cardiomyopathy + NYHA II-III + LVEF ≤ 35%
- Channelopathies: Long QT, Brugada, CPVT with documented VT/syncope
- ARVC with sustained VT or cardiac arrest
- Survivors of cardiac arrest due to VF/VT not from reversible causes
Contraindications
- Absolute: VF/pVT have no absolute contraindications to external defibrillation
- Relative / Precautions:
- Patient is conscious and has a pulse (do not shock a perfusing rhythm)
- "Do Not Resuscitate" (DNR) orders in place
- Defibrillation over an implanted device - pads must be placed at least 8 cm from any ICD/PPM generator
- Wet patient or water contact - must dry skin first
- Transdermal medication patches - remove before pad placement
- Explosive environment
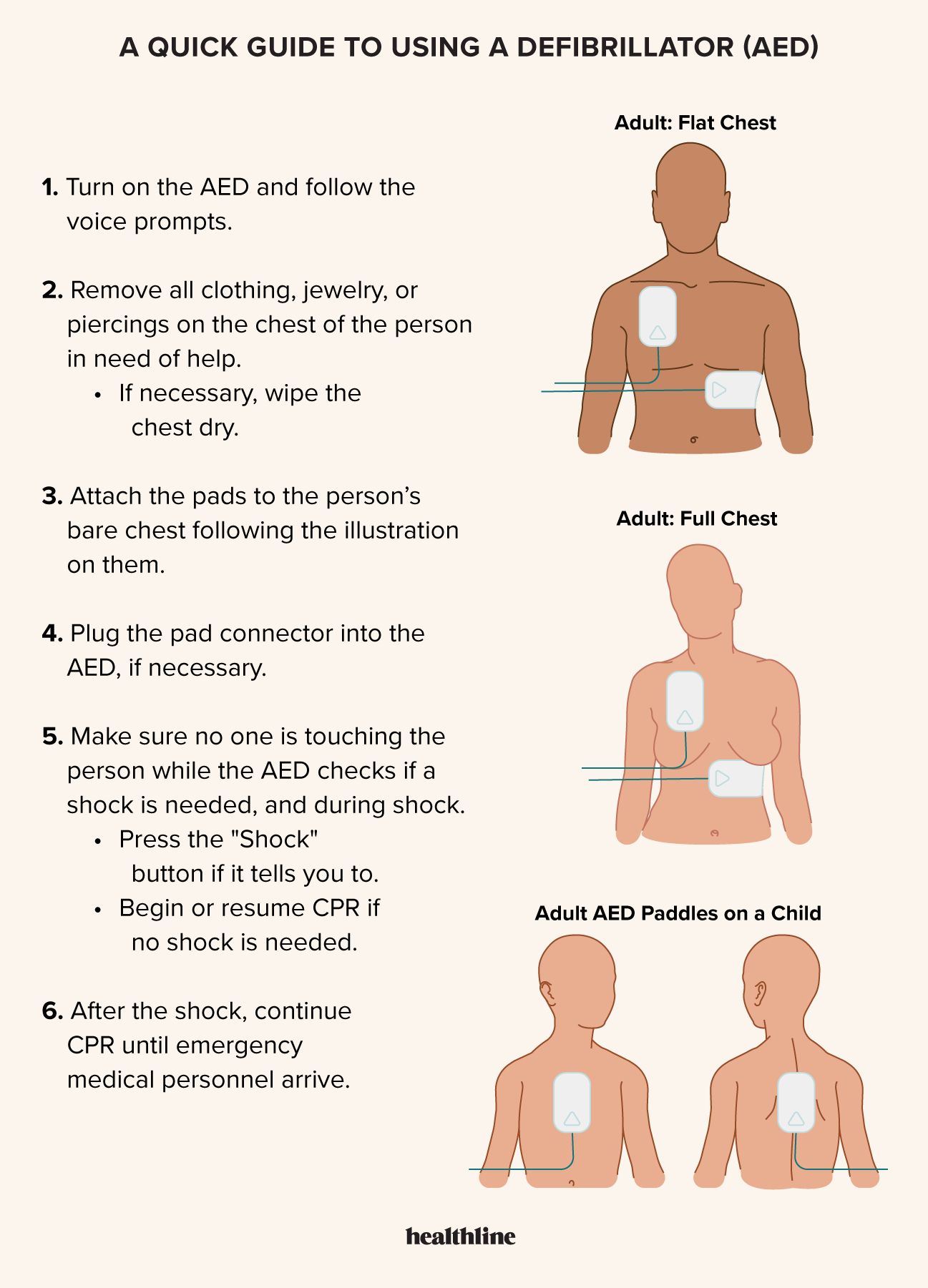
Pad/Paddle Placement

Standard Anterior-Lateral (most common):
- Right pad: right infraclavicular region (below right clavicle, right of sternum)
- Left pad: left lateral chest wall, 5th-6th intercostal space (apex / left axilla)
Anterior-Posterior:
- One pad anterior (left precordium), one pad posterior (left infrascapular region)
- Preferred for cardioversion of AF and when ICD/PPM is present anteriorly
In patients with ICD/Pacemaker:
- Place pads at least 8 cm away from the device generator
- Do not delay defibrillation to achieve optimal pad placement
Energy Settings
| Arrhythmia | Monophasic | Biphasic |
|---|---|---|
| VF/pVT | 360 J | 120-200 J (manufacturer specific) |
| AF cardioversion | 200 J | 100-120 J |
| Atrial flutter | 100 J | 50-100 J |
| SVT/stable VT | 100 J | 50-100 J |
(Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Merck Manual)
2. ICU CARE BUNDLE
Definition
An ICU care bundle is a set of 3-5 evidence-based interventions that, when implemented together consistently, produce significantly better patient outcomes than when applied individually. The concept was introduced by the Institute for Healthcare Improvement (IHI). The key principle is that "all-or-nothing" compliance drives quality improvement.
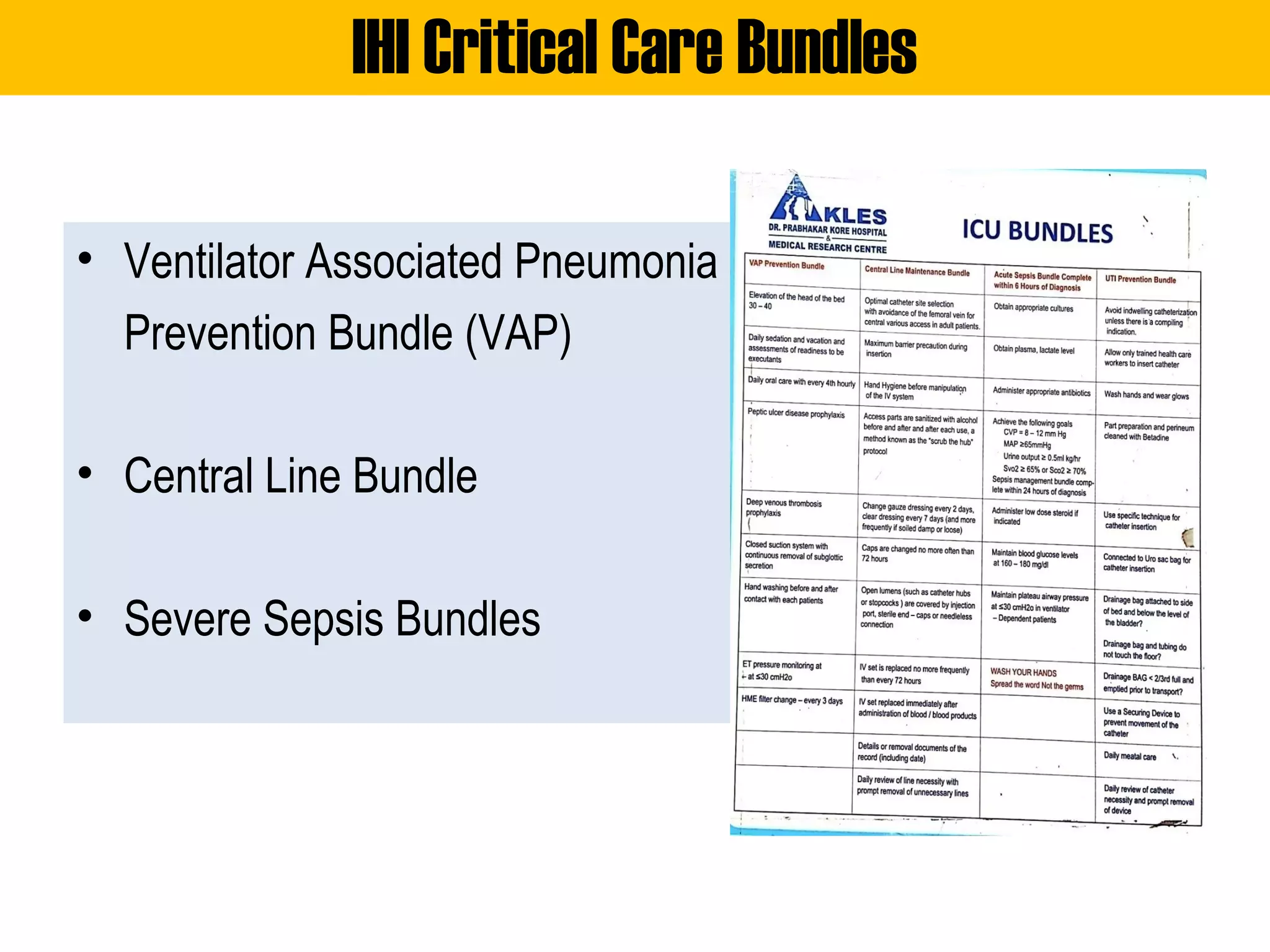
Major ICU Care Bundles
A. Sepsis Bundle (Hour-1 Bundle - Surviving Sepsis Campaign)
| Intervention | Action |
|---|---|
| Measure lactate | Obtain lactate level; remeasure if initial > 2 mmol/L |
| Blood cultures | Obtain before antibiotics |
| Broad-spectrum antibiotics | Administer IV within 1 hour |
| Fluid resuscitation | 30 mL/kg IV crystalloid for hypotension or lactate ≥ 4 mmol/L |
| Vasopressors | Start if MAP < 65 mmHg despite fluids |
Goal: MAP ≥ 65 mmHg, urine output ≥ 0.5 mL/kg/hr
B. Ventilator-Associated Pneumonia (VAP) Bundle

| Component | Detail |
|---|---|
| Head of bed elevation | 30-45° to prevent aspiration |
| Daily sedation vacation (SAT) | Stop sedation daily at 6 AM; assess readiness to wean |
| Spontaneous Breathing Trial (SBT) | Assess daily for extubation readiness |
| Oral hygiene | Chlorhexidine 0.2% oral care every 6 hours |
| ET tube cuff pressure | Maintain 20-30 cmH₂O |
| Subglottic secretion aspiration | Continuous or frequent suctioning |
| Peptic ulcer prophylaxis | IV/oral ranitidine or proton pump inhibitor |
| DVT prophylaxis | LMWH or mechanical (pneumatic compression) |
| Use orogastric (OG) tube | Preferred over NG tube in ventilated patients |
| HME filter change | Every 3 days |
(Source: Barash Clinical Anesthesia 9e; Current Surgical Therapy 14e; NSCCM protocols)
C. Central Line Bundle (CLABSI Prevention)
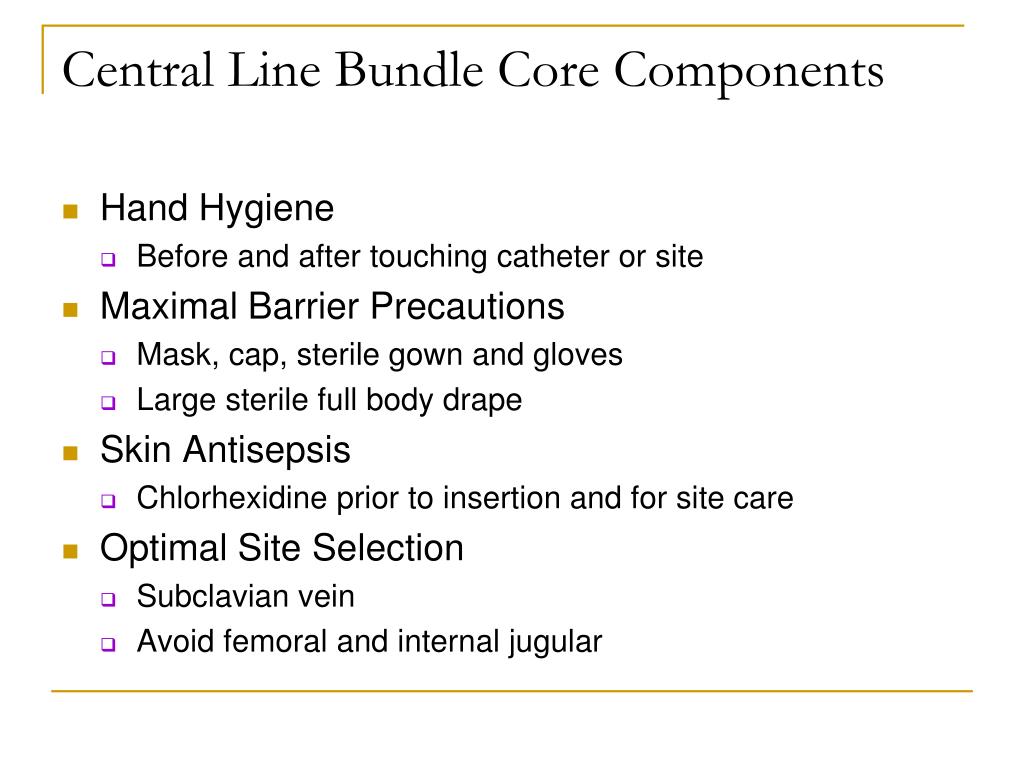
During Insertion:
- Hand hygiene with antiseptic solution (70% alcohol)
- Maximal sterile barrier precautions (cap, mask, sterile gown, gloves, full-body drape)
- Chlorhexidine skin antisepsis at insertion site
- Optimal site selection - prefer subclavian vein; avoid femoral vein
- Complete the Central Line Insertion Checklist (independent observer)
Maintenance:
- Change gauze dressing every 2 days; transparent dressing every 7 days
- Change caps every 72 hours
- Replace IV set no more than every 72 hours (immediately after blood/blood products)
- "Scrub the hub" protocol - disinfect all access ports with alcohol
- Daily review of line necessity; remove promptly when no longer needed
D. UTI Prevention Bundle (CAUTI Prevention)
| Component |
|---|
| Avoid indwelling catheterization unless there is a compelling indication |
| Allow only trained staff to insert catheter |
| Aseptic insertion technique |
| Hand hygiene + sterile gloves |
| Secure the catheter to prevent movement |
| Daily review: is catheter still needed? |
| Drainage bag below bladder level; never let it touch the floor |
| Drainage bag emptied when < 2/3 full and before patient transport |
Why Bundles Work
As stated in Barash's Clinical Anesthesia (9e):
"Implementing a simple ventilator care bundle may reduce the incidence of VAP and antibiotic utilization. Other studies have shown reduced rates of CLABSI by implementing protocols and bundles. An important additional benefit of utilizing standardized care processes is improved ability to track outcomes and engage in quality assurance and quality improvement programs."
3. PACEMAKER
What Is a Pacemaker?
A pacemaker is an implantable or external electronic device that senses intrinsic cardiac activity and delivers timed electrical impulses to stimulate myocardial contraction when the heart's own rate is too slow or absent.
(Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine)
Types of Pacemakers
| Type | Description |
|---|---|
| Temporary External Transcutaneous | Pads placed on chest; used in emergencies; uncomfortable, unreliable for extended use |
| Temporary Transvenous | Lead inserted via subclavian/internal jugular vein into RV; used in ICU for acute bradycardia |
| Permanent Single-Chamber (VVI/AAI) | Lead in right ventricle or right atrium only |
| Permanent Dual-Chamber (DDD) | Leads in both RA and RV; maintains AV synchrony |
| Biventricular / Cardiac Resynchronization Therapy (CRT) | Three leads (RA, RV, LV via coronary sinus); for heart failure + LBBB |
| Leadless Pacemaker | Capsule implanted directly in RV (e.g., Micra, AVEIR); no subcutaneous pocket |
| ICD with pacing capability | Combines anti-tachycardia pacing with defibrillation |
NBG Pacemaker Code (First 3 Positions)
| Position | Meaning | Common Values |
|---|---|---|
| 1st letter | Chamber paced | A (atrium), V (ventricle), D (dual) |
| 2nd letter | Chamber sensed | A, V, D, O (none) |
| 3rd letter | Response to sensing | I (inhibit), T (trigger), D (dual), O (none) |
Examples: VVI = ventricle paced, ventricle sensed, inhibited; DDD = dual paced, dual sensed, dual response
Indications
Temporary Pacing:
- Symptomatic bradycardia not responding to atropine
- Complete heart block (3rd degree AV block) with hemodynamic instability
- Sinus arrest or sick sinus syndrome with syncope
- Bilateral bundle branch block post-MI
- Bridge to permanent pacemaker
Permanent Pacemaker Indications (Class I - ACC/AHA/HRS):
- Symptomatic sinus bradycardia (syncope, pre-syncope, heart failure)
- Complete (3rd degree) AV block
- 2nd degree AV block (Mobitz Type II)
- Symptomatic sick sinus syndrome
- Chronotropic incompetence with symptoms
- Hypersensitive carotid sinus syndrome with recurrent syncope
- CRT for LBBB + LVEF ≤ 35% + NYHA Class II-IV on optimal medical therapy
Contraindications
- No absolute contraindications for temporary pacing when clinically indicated
- Relative contraindications:
- Coagulopathy (bleeding risk during transvenous placement)
- Active systemic infection / bacteremia (risk of device infection)
- Severe tricuspid stenosis or mechanical TV prosthesis (transvenous route blocked)
- Unwillingness or inability to comply with follow-up (permanent)
- Terminal illness with no expected benefit
Pacemaker Placement
Temporary Transvenous (Emergency):
- Access: Right internal jugular vein preferred (or subclavian/femoral)
- Seldinger technique: guidewire → dilator + sheath → pacing catheter through sheath
- Advance balloon-tipped catheter - inflate balloon at 10-12 cm depth after entering SVC
- Blind method (emergency): Advance to 20 cm, set rate 80 bpm, output 20 mA, asynchronous mode - capture seen as pacing spike + QRS on monitor
- ECG-guided: Connect distal catheter terminal to V1 lead of ECG; large P waves = atrium, ST elevation + QS pattern = right ventricular endocardium (correct position)
- Deflate balloon; secure lead; confirm position with CXR
Permanent Pacemaker:
- Access: Subclavian or cephalic vein
- Leads guided fluoroscopically to RA appendage and/or RV apex
- Pulse generator placed in subcutaneous pocket below left clavicle
- Battery life: 7-12 years; weight ~30 g
(Source: Roberts and Hedges' Clinical Procedures in Emergency Medicine, pp. 327-343)
Complications
| Complication | Notes |
|---|---|
| Pneumothorax / hemothorax | During subclavian/jugular access |
| Lead dislodgement | Most common early complication |
| Cardiac perforation / tamponade | Lead tip migration |
| Infection / pocket hematoma | Local or systemic |
| Pacemaker syndrome | Loss of AV synchrony in VVI; symptoms: vertigo, syncope, hypotension |
| Failure to capture / failure to sense | Device malfunction |
| Phrenic nerve / diaphragm stimulation | Lead position too close to phrenic nerve |
| Runaway pacemaker | Rapid uncontrolled pacing - emergency |
4. INFUSION PUMP
What Is an Infusion Pump?
An infusion pump is an electronic medical device that delivers fluids, medications, blood products, or nutrients into a patient's body in controlled amounts through an intravenous (IV), subcutaneous, epidural, or enteral route. It replaces the need for manual drip calculations and ensures precision in high-risk drug delivery.
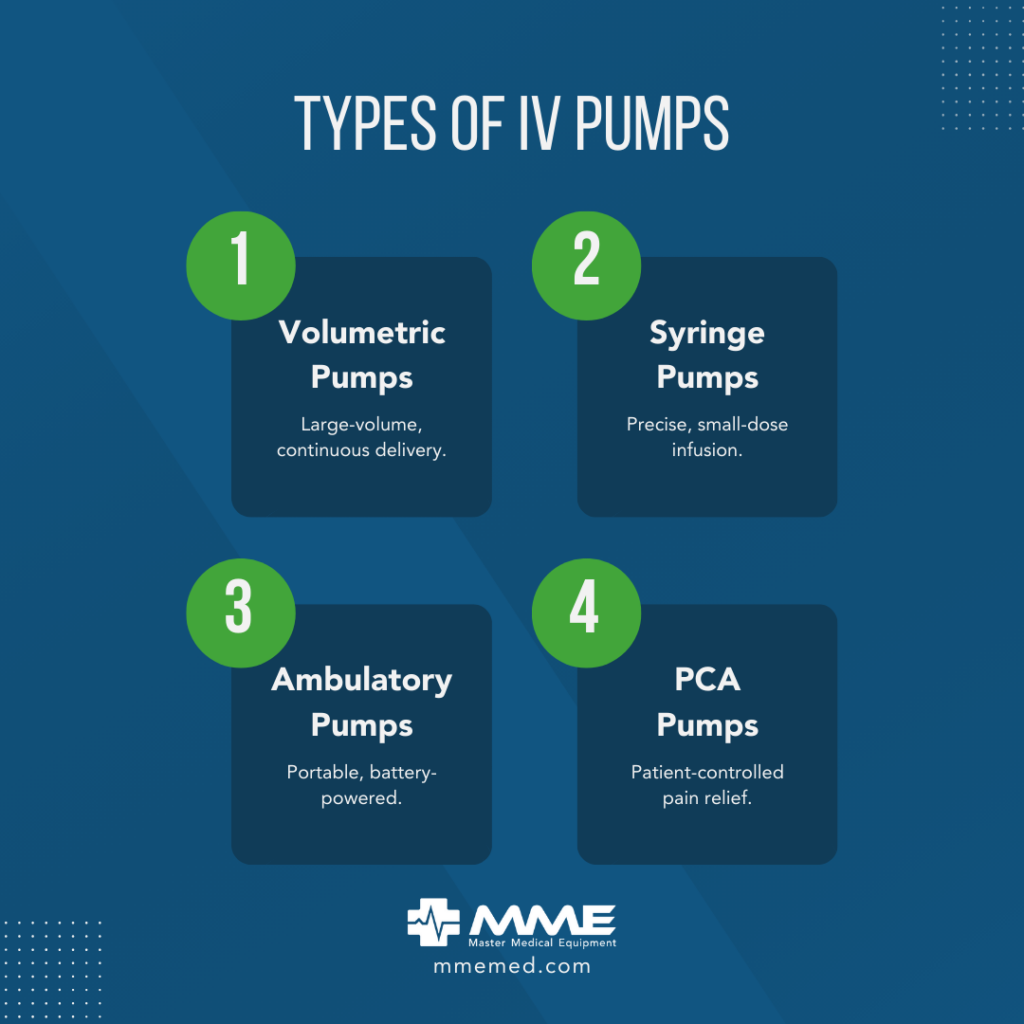
Types of Infusion Pumps
| Type | Description | Key Use |
|---|---|---|
| Volumetric Pump (Large-Volume Pump) | Delivers large volumes of fluid at a set rate (mL/hr); driven by peristaltic or cassette mechanism | IV fluids, antibiotics, TPN, continuous infusions |
| Syringe Pump | Uses a motorized syringe driver; ideal for small, precise volumes at very low flow rates | ICU vasoactives, inotropes, sedation, insulin, neonates |
| PCA Pump (Patient-Controlled Analgesia) | Allows patient to self-administer preset bolus doses within lockout intervals | Post-operative pain, cancer pain, epidural analgesia |
| Ambulatory Pump | Small, portable, battery-powered; worn by patient | Outpatient chemo, home IV antibiotics, insulin |
| Elastomeric Pump | Disposable balloon reservoir that deflates at a controlled rate; no electronics | Post-surgical pain infusions, outpatient antibiotics |
| Implantable Pump | Surgically placed in subcutaneous tissue; delivers drug directly to target (e.g., intrathecal baclofen, hepatic arterial chemotherapy) | Spasticity, cancer pain, hepatic artery infusion |
| Smart Pump | Volumetric or syringe pump with dose error reduction software (DERS), drug libraries, connectivity | ICU safety; reduces medication errors |
| Insulin Pump (CSII) | Continuous subcutaneous insulin infusion; mimics basal-bolus dosing | Type 1 and brittle Type 2 diabetes |
| Enteral Pump | Delivers formula through nasogastric, PEG, or jejunostomy tube | Nutritional support for patients unable to eat |
Indications
- Administration of drugs requiring precise dose control (vasopressors, inotropes, insulin, heparin, chemotherapy, opioids)
- Continuous or intermittent antibiotic therapy
- IV fluid replacement and blood product administration
- Parenteral nutrition (TPN/PN)
- Patient-controlled analgesia (PCA) - acute and chronic pain management
- Epidural analgesia (labor, post-surgical)
- Spinal spasticity management (intrathecal baclofen)
- Hepatic artery chemotherapy infusion for liver metastases
- Home infusion therapy (outpatient IV antibiotics, immunoglobulin, biologics)
- Pediatric/neonatal high-risk drug delivery requiring sub-mL/hr accuracy
Contraindications / Precautions
| Situation | Concern |
|---|---|
| Incompatible IV lines | Do not co-infuse incompatible drugs through same line (precipitation risk) |
| Arterial lines | Infusion pumps are designed for venous access only unless specifically designed for arterial use |
| Infiltrated/non-patent IV site | Will cause tissue damage or extravasation injury |
| Ambient temperature extremes | Affects elastomeric pump flow rates |
| Pump programming errors | "10x" dose errors can be fatal - requires double-check protocols; smart pumps with DERS mitigate this |
| MRI environment | Most infusion pumps are not MRI-compatible; use MRI-safe alternatives |
| Power failure | Battery backup required for life-critical infusions |
| Air-in-line | Alarms and detector systems must be functional; air emboli risk |
| Implantable pumps | Contraindicated in: active infection, inadequate body mass for pocket, patient unable to care for device |
Placement
| Route | Device Used | Notes |
|---|---|---|
| Peripheral IV | Volumetric, syringe, PCA | Most common; short-term |
| Central Venous Catheter | Volumetric, syringe, multi-channel pumps | For vasopressors, TPN, irritant drugs |
| Subcutaneous | Syringe pump, insulin pump | Analgesics, insulin, CSII |
| Epidural | Syringe or ambulatory pump | Epidural analgesia |
| Intrathecal | Implantable pump | Baclofen for spasticity, opioids for cancer pain |
| Enteral (NG/PEG/J-tube) | Enteral pump | Nutritional support |
| Hepatic artery (via surgically placed catheter) | Implantable pump | Regional chemotherapy |
Key Safety Features
- Drug libraries / DERS (Dose Error Reduction Software) - programmed concentration limits and alert thresholds
- Air-in-line detector
- Occlusion / back-pressure alarm
- Keep-vein-open (KVO) rate to maintain line patency
- Lockout interval (PCA pumps) - prevents overdose
- Battery backup for transport of critical patients
- Free-flow prevention - anti-siphon valve on tubing sets
Summary Comparison Table
| Device | Primary Function | Key Setting | Key Complication |
|---|---|---|---|
| Defibrillator | Terminate VF/pVT | Energy (J), synchronized vs. unsynchronized | Burns, failed cardioversion, device damage near ICD |
| Pacemaker | Maintain/restore heart rate | Rate, output, sensitivity, mode (VVI/DDD etc.) | Lead dislodgement, infection, pacemaker syndrome |
| ICU Care Bundle | Prevent ICU complications | Protocol compliance (all-or-nothing) | Non-compliance leads to VAP, CLABSI, sepsis mortality |
| Infusion Pump | Precise drug/fluid delivery | Rate (mL/hr), dose (mcg/kg/min), lockout | Programming error, extravasation, air embolism |
Sources:
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783), pp. 327-596
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e (9781975199074), ICU Protocols and Care Bundles chapter
- Current Surgical Therapy 14e - VAP Bundle
- NSCCM ICU Care Bundles Protocol
- Merck Manual - ICD Indications Table
- ACC/AHA/HRS Pacemaker Guidelines
- Surviving Sepsis Campaign Hour-1 Bundle (2018)
This is a shared conversation. Sign in to Orris to start your own chat.