Fontan corculations
Reading File
Finding Sources
Searching PubMed
Fontan circulation management outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compose a thorough answer.
Fontan Circulation
Concept and Background
The Fontan circulation is a surgically created physiology used for patients with single-ventricle congenital heart defects - conditions where only one functional ventricle exists (e.g., tricuspid atresia, hypoplastic left heart syndrome, double-inlet left ventricle, and many others). It was first described by Fontan and Kreutzer in the early 1970s.
Core principle: Systemic venous blood (deoxygenated) is directed passively and directly into the pulmonary arteries without any intervening ventricular power source. The single functional ventricle pumps only oxygenated blood to the systemic circulation. Pulmonary blood flow therefore depends entirely on the pressure gradient between the systemic venous system and the pulmonary venous atrium.
- Miller's Anesthesia, 10e, p. 10879
Surgical Stages
The Fontan operation is performed in staged palliation, typically over the first 2-4 years of life:
Stage 1 - Initial Palliation (Neonatal)
- If pulmonary blood flow is too low: Modified Blalock-Taussig (BT) shunt - a Gore-Tex conduit between the subclavian artery and pulmonary artery
- If pulmonary blood flow is excessive: Pulmonary artery banding to protect against high pulmonary vascular resistance (PVR)
Stage 2 - Bidirectional Glenn Shunt (4-6 months)
The superior vena cava (SVC) is anastomosed to the superior aspect of the right pulmonary artery. This:
- Partially separates circulations (SVC blood goes directly to lungs)
- Volume-unloads the single ventricle (critical preparatory step before Fontan)
- Maintains systemic cardiac output while reducing volume overload
Stage 3 - Fontan Completion (2-4 years of age)
Inferior vena cava (IVC) flow is also directed to the pulmonary arteries, completing total cavopulmonary connection (TCPC).
- Fuster & Hurst's The Heart, 15th Ed., p. 2033
- Sabiston Textbook of Surgery, p. 2587
Surgical Variants
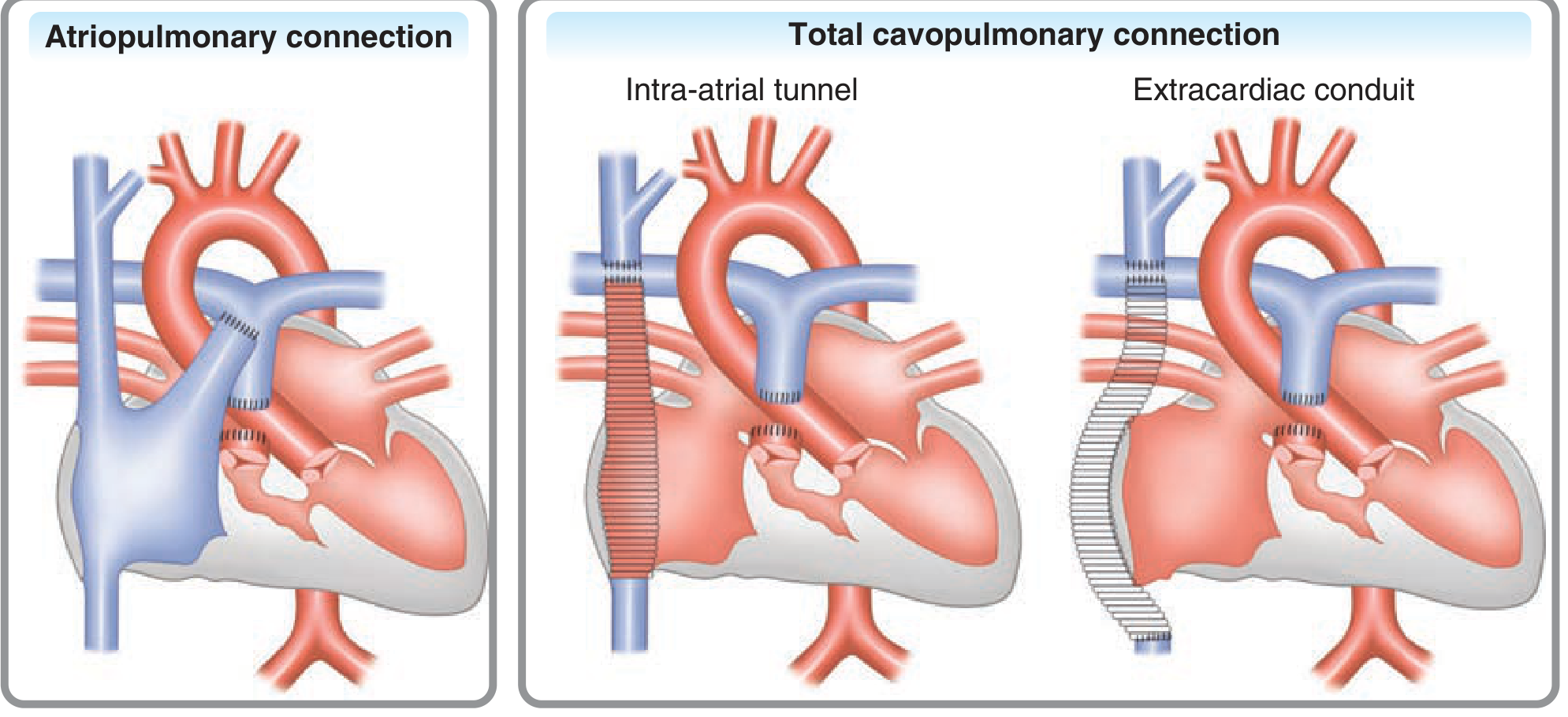
Figure: Three Fontan types - Atriopulmonary connection (historical); Total cavopulmonary connection via intra-atrial tunnel; Total cavopulmonary connection via extracardiac conduit (Fuster & Hurst's The Heart)
| Type | Description | Status |
|---|---|---|
| Atriopulmonary connection | Right atrial appendage directly anastomosed to pulmonary artery bifurcation | Historical - largely abandoned |
| Lateral tunnel (TCPC) | Surgically created intra-atrial baffle directs IVC flow to PA; SVC connected via Glenn | Widely used |
| Extracardiac conduit (TCPC) | Gore-Tex conduit from IVC to PA; no atrial suture lines | Most common currently |
The shift to TCPC improved flow dynamics, reduced thrombus risk, decreased atrial arrhythmias, and eliminated the massive right atrial dilation seen with atriopulmonary connections.
Prerequisites for an Effective Fontan Circulation
Since pulmonary blood flow is passive, any impediment to flow leads to Fontan failure. Ideal criteria include:
- Low pulmonary vascular resistance (PVR) and low mean pulmonary artery pressure
- Good ventricular function (low end-diastolic pressure, no significant diastolic dysfunction)
- Adequate pulmonary artery architecture - no branch PA stenosis or hypoplasia
- No significant AV valve regurgitation (increases atrial pressure)
- Unobstructed systemic arterial outlet and normal semilunar valve
- Normal pulmonary venous drainage and low left atrial pressure
- Normal sinus rhythm (atrial arrhythmias are very poorly tolerated)
Some "modifiable" contraindications (e.g., moderate AV valve regurgitation, branch PA stenosis) can be addressed surgically or by stenting before Fontan completion.
- Sabiston Textbook of Surgery, p. 2587
Fontan Physiology - Key Hemodynamics
- Central venous pressure rises acutely to 12-15 mmHg post-operatively
- Expected O2 saturation post-Fontan: ≥95% (lower values suggest Fontan failure or significant shunting)
- Pulmonary blood flow depends on respiratory mechanics: spontaneous ventilation augments Fontan flow; positive pressure ventilation (PPV) and PEEP impede it
- Any increase in PVR, decreased venous volume, or myocardial depressants is poorly tolerated
Fenestration
Some Fontan procedures include a fenestration - a deliberate small shunt between the Fontan circuit and the pulmonary venous atrium. This:
- Acts as a "pop-off valve" when pulmonary pressures are elevated
- Preserves ventricular preload at the cost of mild desaturation (right-to-left shunt)
- Reduces post-operative pleural effusions and ascites
- Can be closed percutaneously later if hemodynamics permit
Routine fenestration is used selectively - risks include hypoxia and systemic embolism.
Long-Term Complications
The Fontan circulation is not normal, and complications accumulate over time:
1. Fontan-Associated Liver Disease (FALD)
-
Ubiquitous in long-term survivors
-
Caused by chronically elevated central venous pressure leading to passive hepatic congestion, eventually progressing to cardiac cirrhosis
-
Serum transaminases and GGT may be mildly elevated; synthetic function preserved until late stages
-
Hepatocellular carcinoma (HCC) is a rare but serious complication - screen with AFP and imaging
-
Surveillance: ultrasound or MRI every 1-2 years
-
Combined heart-liver transplantation is increasingly performed for advanced FALD
-
Braunwald's Heart Disease, p. (ACHD chapter)
2. Protein-Losing Enteropathy (PLE)
- Serious complication from elevated systemic venous pressure leading to gut lymphatic dysfunction
- Protein loss via gut leads to hypoalbuminemia, edema, ascites, immunodeficiency
- High mortality if untreated
3. Atrial Arrhythmias
- Atrial flutter and fibrillation are very common (especially in old atriopulmonary connections with massive RA dilation)
- Very poorly tolerated hemodynamically due to loss of atrial contribution to ventricular filling and passive PA flow
- Modern TCPC designs reduced (but did not eliminate) arrhythmia risk
4. Thromboembolism
- Sluggish venous flow in the Fontan circuit promotes thrombus formation
- Risk of stroke and pulmonary embolism
- Chronic anticoagulation considered for high-risk patients
5. Progressive Ventricular Dysfunction
- The single ventricle (often a morphological RV acting as systemic ventricle) is inherently prone to long-term failure
- HF therapies proven in two-ventricle patients may not be efficacious here
6. Plastic Bronchitis
- Rare - formation of bronchial casts from lymphatic leak into airways
Survival and Outcomes
From the Australian and New Zealand Fontan Registry:
-
90% survive to age 30
-
80% survive to age 40
-
Only 53% are in NYHA class I at age 30
-
Survival significantly worse for atriopulmonary connections vs. cavopulmonary connections
-
Common causes of death: thromboembolism, heart failure, protein-losing enteropathy, arrhythmias
-
Miller's Anesthesia, 10e, p. 10880
Anesthesia / Perioperative Considerations
Fontan patients presenting for non-cardiac surgery require careful management:
- Avoid PPV with high PEEP - directly impairs passive pulmonary blood flow; favor early extubation
- Avoid hypovolemia - reduces venous pressure driving pulmonary flow
- Avoid vasodilators - reduce systemic venous return
- Avoid myocardial depressants
- Maintain normal PVR - avoid hypoxia, hypercarbia, acidosis, high airway pressures (all raise PVR)
- Failing Fontan patients are at extreme risk during abdominal surgery or procedures with large fluid shifts
- Check coagulation status - hepatic dysfunction from FALD can cause coagulopathy
- Chronic anticoagulation is common - manage perioperatively
Pregnancy in Fontan Patients
-
Impaired ability to increase cardiac output during pregnancy
-
Risk of SVT (~9%), heart failure (~4%); maternal mortality low with careful selection
-
Fetal/neonatal outcomes poor: miscarriage 45%, high rates of prematurity and cesarean delivery
-
Antiplatelet therapy (low-dose aspirin) recommended; LMWH for those with arrhythmias or prior embolism
-
Vaginal delivery preferred; delivery at a specialized center with a maternal heart team is mandatory
-
Braunwald's Heart Disease, p. 1084
Recent Evidence (2024-2026)
Three recent systematic reviews are worth noting:
- Cardiac rehabilitation in Fontan patients shows benefit [PMID: 39597002] (Medicina, Nov 2024) - exercise training is feasible and improves outcomes
- Extracardiac conduit long-term outcomes meta-analysis [PMID: 39952466] (Can J Cardiol, Jun 2025) - confirms good intermediate-term survival
- Combined heart-liver transplantation for failing Fontan [PMID: 40320589] (Transplantation, Nov 2025) - single-arm meta-analysis showing good survival, supporting this as a valid option for end-stage disease
Summary: The Fontan circulation is a life-sustaining but inherently abnormal palliation for single-ventricle hearts. Blood flows passively through the pulmonary circuit, making patients exquisitely sensitive to anything that raises PVR or reduces venous preload. While modern TCPC techniques have improved outcomes, the majority of patients develop significant multi-organ complications over decades, and the long-term trajectory is one of progressive Fontan failure requiring transplantation.
This is a shared conversation. Sign in to Orris to start your own chat.