10 Common Heart Diseases with ECG Changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive material from authoritative textbooks. Here is a complete, well-organized reference on 10 common heart diseases with their ECG changes:
10 Common Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia, injury, and eventually necrosis of the myocardium.
ECG Changes (in sequence):
| Phase | Finding |
|---|---|
| Hyperacute (minutes) | Tall, peaked (hyperacute) T waves in the territory |
| Acute injury (hours) | ST-segment elevation ≥1 mm in 2+ contiguous leads; reciprocal ST depression in opposite leads |
| Evolving (hours-days) | Pathological Q waves (>40 ms wide, >25% of R wave amplitude); T-wave inversion |
| Old/established | Persistent Q waves; T waves may normalize |
Territory localization:
- Inferior (RCA): ST elevation in II, III, aVF
- Anterior (LAD): ST elevation in V1-V4
- Lateral (LCx): ST elevation in I, aVL, V5-V6
- Posterior (RCA/LCx): Tall R and ST depression in V1-V3 (mirror image)
- Right ventricular (RCA): ST elevation in V4R
ECG - Inferior-lateral MI (LCx occlusion):
ECG - Left main/proximal LAD occlusion:
2. Non-ST-Elevation ACS (NSTEMI / Unstable Angina)
Pathophysiology: Partial/dynamic coronary occlusion causing subendocardial ischemia without full-thickness necrosis.
ECG Changes:
- ST depression (horizontal or downsloping) ≥0.5-1 mm in 2+ contiguous leads - the hallmark
- T-wave inversion (deep, symmetric) in affected territory
- Transient ST changes that may resolve with symptom relief
- ECG may be entirely normal in 1-6% of true NSTEMIs
- No pathological Q waves (subendocardial infarction)
"The diagnosis of NSTEMI depends on abnormal elevation of cardiac biomarkers but may include ECG changes not meeting criteria for STEMI." - Tintinalli's Emergency Medicine
Key difference from STEMI: Absence of ST elevation or new LBBB; troponin elevation confirms NSTEMI over unstable angina.
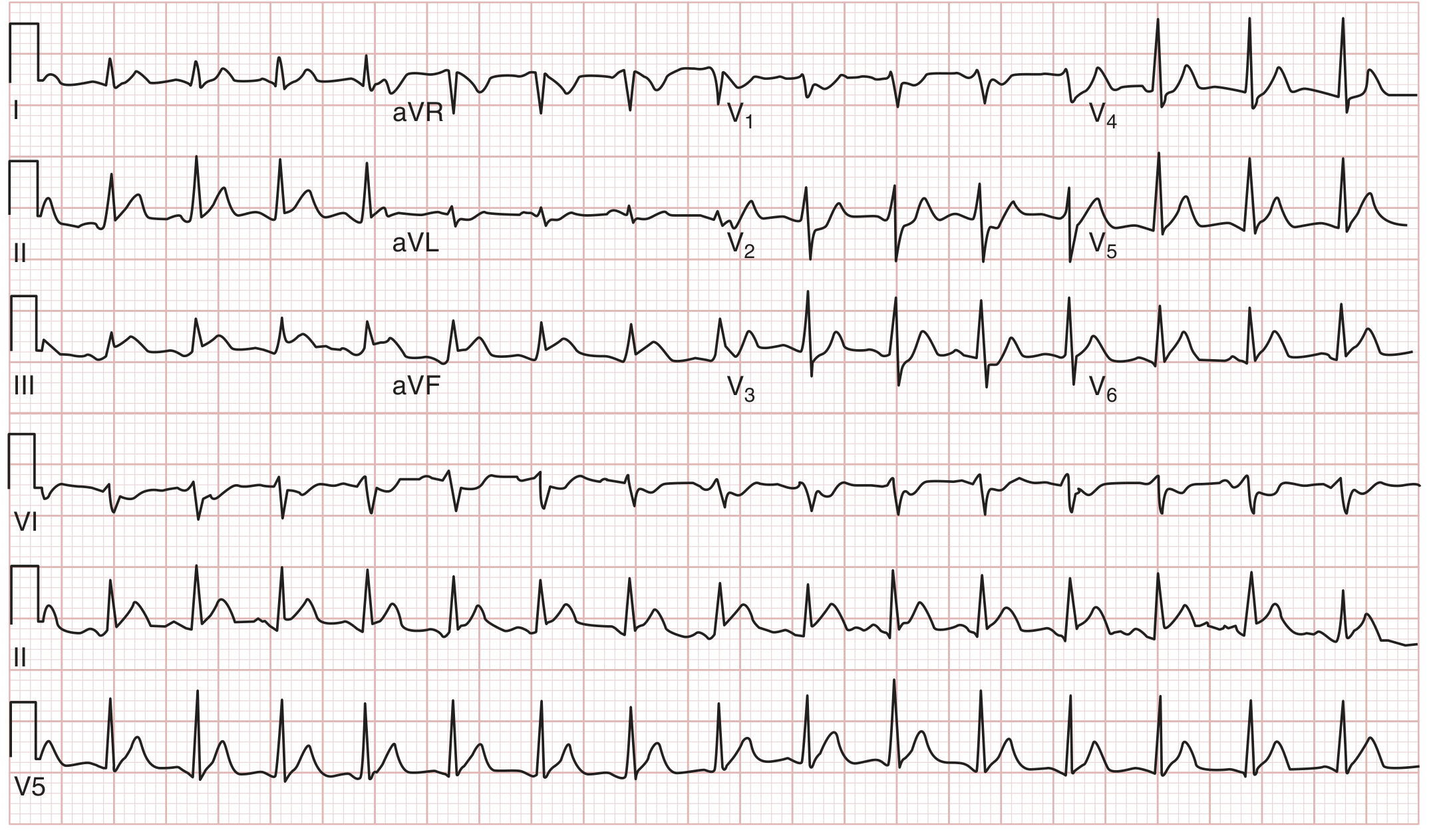
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized electrical activity from multiple re-entrant wavelets in the atria - often triggered by atrial enlargement, valve disease, hypertension, or heart failure.
ECG Changes:
| Feature | Finding |
|---|---|
| P waves | Absent - replaced by fibrillatory baseline (f waves at 350-600 bpm) |
| Baseline | Irregular, low-voltage oscillations (fine or coarse) |
| RR intervals | Irregularly irregular - the hallmark |
| QRS complexes | Normal morphology (unless aberrant conduction or pre-excitation) |
| Ventricular rate | Variable, typically 100-160 bpm if uncontrolled |

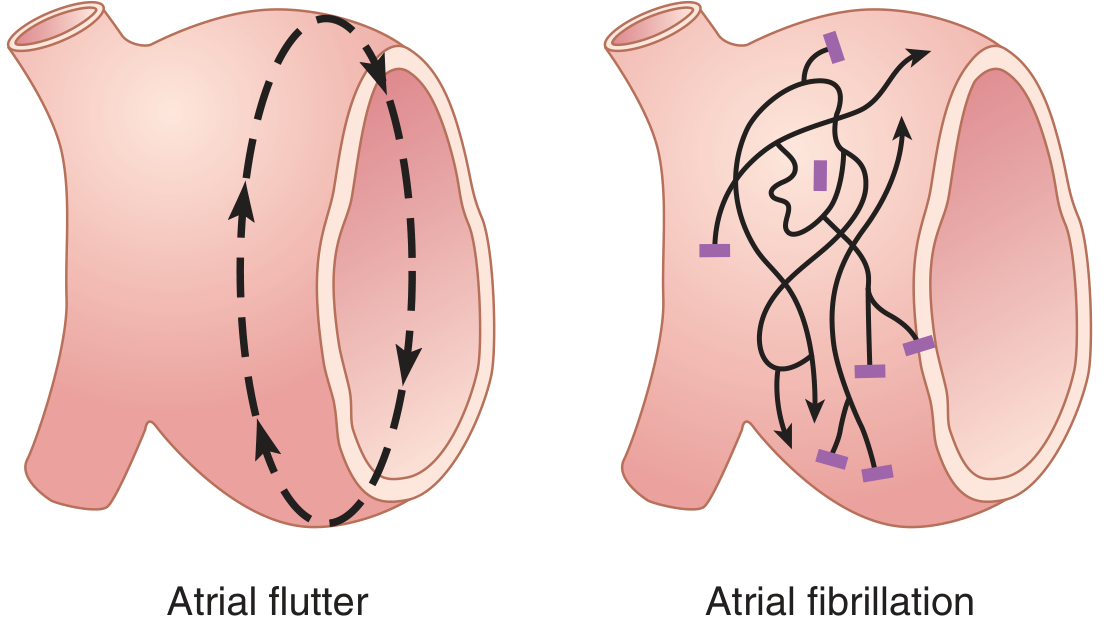
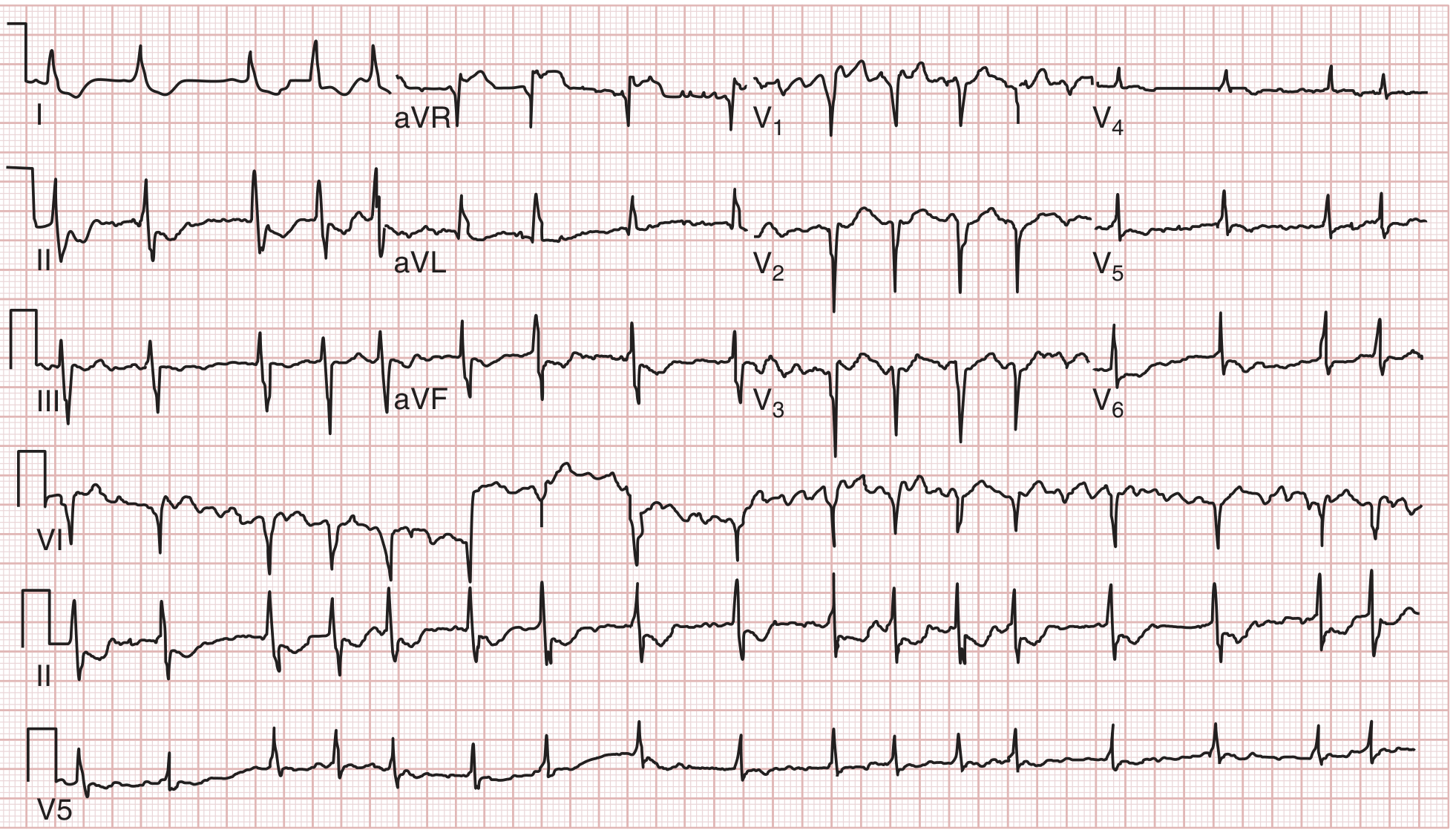
4. Atrial Flutter
Pathophysiology: A single large macro-re-entrant circuit in the right atrium (typically around the tricuspid annulus), producing regular atrial depolarizations at ~300 bpm.
ECG Changes:
| Feature | Finding |
|---|---|
| P waves | Replaced by "sawtooth" flutter waves (F waves) at ~300 bpm, best seen in II, III, aVF, V1 |
| Rhythm | Regular flutter waves; ventricular rate depends on AV conduction ratio |
| AV conduction | Typically 2:1 (ventricular rate ~150 bpm), 3:1, or 4:1 block |
| RR interval | Regular if fixed block ratio; irregular if variable |
| QRS | Normal morphology |
A useful bedside trick: a regular narrow-complex tachycardia at exactly 150 bpm should always raise suspicion for atrial flutter with 2:1 block until proven otherwise.
5. Complete Heart Block (Third-Degree AV Block)
Pathophysiology: Complete dissociation between atrial and ventricular conduction - no impulses pass through the AV node. Causes include ischemia (inferior MI most common), Lyme disease, medications (digoxin, beta-blockers), and degenerative conduction system disease.
ECG Changes:
| Feature | Finding |
|---|---|
| P waves | Present at regular rate (sinus rate, typically 60-100 bpm) |
| QRS complexes | Present at slower, independent "escape" rate |
| PR interval | Completely variable - no fixed relationship between P and QRS |
| AV dissociation | P waves and QRS complexes march through each other independently |
| Escape rhythm | Junctional (narrow QRS, rate 40-60) or ventricular (wide QRS, rate 20-40) |
Associated ECG findings:
- In inferior MI context: Wenckebach (Mobitz I) or complete block from RCA ischemia to AV node
- New LBBB in ischemia context = equivalent of ischemic ECG changes
"Prolonged PR interval, new LBBB, or new RBBB with left anterior hemiblock suggests spread of infection into the conduction system." - Tintinalli's Emergency Medicine (in the context of endocarditis/myocarditis)
6. Left Bundle Branch Block (LBBB)
Pathophysiology: Conduction delay or block in the left bundle branch, causing abnormal, sequential ventricular activation (right then left ventricle).
ECG Changes (the "WiLLiaM" pattern):
| Feature | Finding |
|---|---|
| QRS duration | Broad (≥120 ms) |
| V1 | Deep, broad S wave (W shape: rS or QS pattern) |
| V5-V6, I, aVL | Tall, notched R wave (no septal Q waves) - "M" shape |
| ST/T changes | Discordant - ST and T opposite direction to main QRS deflection |
| Axis | Usually left axis deviation |
Clinical significance:
- New LBBB in a patient with chest pain = treat as STEMI equivalent
- Sgarbossa criteria help identify superimposed MI in LBBB: concordant ST elevation ≥1 mm, concordant ST depression ≥1 mm in V1-V3, or excessive discordant ST elevation >25% of S wave depth
7. Right Bundle Branch Block (RBBB)
Pathophysiology: Conduction delay in the right bundle branch; right ventricle is depolarized late via myocardial cell-to-cell conduction.
ECG Changes (the "MaRRoW" pattern):
| Feature | Finding |
|---|---|
| QRS duration | Broad (≥120 ms) |
| V1 | RSR' ("rabbit ears" / M shape) - rSR' pattern |
| V5-V6, I | Wide, slurred S wave |
| T waves | Discordant (opposite direction to terminal QRS deflection) |
| Axis | Usually normal |
"A conduction delay or block in the right bundle branch results in a typical RBBB QRS pattern on the surface ECG (M-shape or rSR' in V1) and may represent a congenital abnormality or underlying organic heart disease." - Morgan and Mikhail's Clinical Anesthesiology
Clinical notes: Isolated RBBB is less ominous than LBBB; new RBBB + left anterior hemiblock (bifascicular block) in chest pain warrants urgent evaluation.
8. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric septal hypertrophy (usually autosomal dominant sarcomere gene mutation) causing dynamic LVOTO, diastolic dysfunction, and risk of sudden cardiac death - the most common cause of sudden death in young athletes.
ECG Changes:
| Feature | Finding |
|---|---|
| Voltage | Left ventricular hypertrophy (Sokolov-Lyon: S in V1 + R in V5/V6 ≥35 mm) |
| Septal Q waves | Deep, narrow Q waves in lateral leads (I, aVL, V5-V6) - from septal hypertrophy |
| T-wave changes | T-wave inversion in lateral leads; if present without Q waves = suggests ischemia |
| ST changes | ST depression in lateral leads |
| P waves | Left atrial abnormality (broad, notched P wave) if LA enlarged |
| Rhythm | May show AF, SVT, or ventricular arrhythmias |
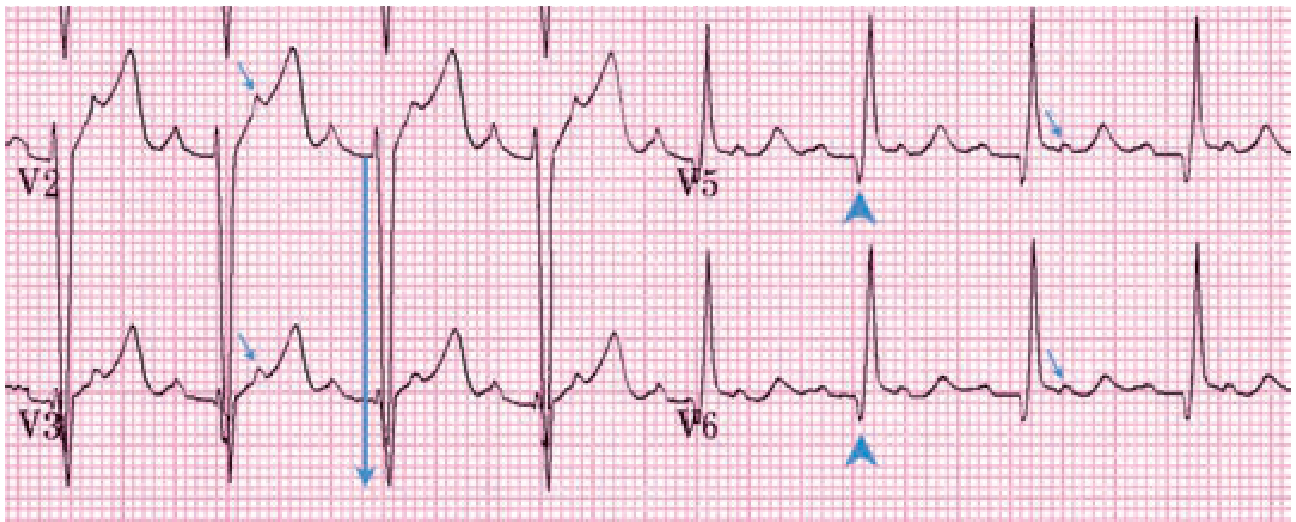
"An ECG tracing showing Q waves or inferolateral repolarization changes in an athlete favors the diagnosis of hypertrophic cardiomyopathy." - Goldman-Cecil Medicine
9. Wolff-Parkinson-White Syndrome (WPW)
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing pre-excitation of part of the ventricle before normal conduction arrives. This creates the classic ECG triad and predisposes to re-entrant tachycardias (AVRT) and - if AF develops - rapid ventricular response that can degenerate to VF.
ECG Changes (the classic triad in sinus rhythm):
| Feature | Finding |
|---|---|
| PR interval | Short (<120 ms) - pre-excitation bypasses AV node delay |
| Delta wave | Slurred upstroke of the QRS complex (initial slow inscription of the QRS) |
| QRS duration | Prolonged (≥120 ms) due to fusion of pre-excited and normally conducted impulses |
| ST/T changes | Secondary repolarization abnormalities (discordant to delta/QRS) |
During tachycardia:
- Orthodromic AVRT: Narrow QRS tachycardia (antegrade via AV node, retrograde via accessory pathway)
- Antidromic AVRT: Wide QRS tachycardia (antegrade via accessory pathway - looks like VT)
- AF with WPW: Irregularly irregular, very wide, bizarre QRS - life-threatening (avoid AV nodal blocking agents)
"AVNRT caused by an accessory bypass tract (WPW) may be evident on the ECG by the characteristic delta wave (slurred upstroke of QRS complex), short PR interval, and prolonged QRS complex." - Textbook of Family Medicine
10. Long QT Syndrome (LQTS)
Pathophysiology: Delayed ventricular repolarization due to genetic mutations in cardiac ion channel genes (most commonly KCNQ1/LQT1, KCNH2/LQT2, SCN5A/LQT3) or acquired causes (drugs, hypokalemia, hypomagnesemia). Prolonged repolarization creates early afterdepolarizations that trigger torsades de pointes (TdP) and sudden cardiac death.
ECG Changes:
| Feature | Finding |
|---|---|
| QTc interval | Prolonged (≥450 ms males, ≥460 ms females; dangerous if ≥500 ms) |
| QTc formula | Bazett: QTc = QTm / √RR (in seconds) |
| T-wave morphology | Broad, notched, or bifid T waves depending on LQTS subtype |
| LQT1 | Broad-based T waves; events triggered by exercise/swimming |
| LQT2 | Low amplitude, notched T waves; events with sudden noise/emotion |
| LQT3 | Long isoelectric ST segment with peaked T waves; events at rest/sleep |
| Torsades de pointes | "Twisting of the points" - polymorphic VT with QRS axis rotating around baseline |
"The long QT syndrome is characterized by prolongation of the corrected QT interval, syncope, and sudden death caused by torsades de pointes and ventricular fibrillation." - Tintinalli's Emergency Medicine
Important acquired causes of prolonged QTc: antipsychotics (haloperidol, ziprasidone), macrolide antibiotics, fluoroquinolones, antifungals (azoles), antiarrhythmics (class IA and III), tricyclic antidepressants, hypokalemia, hypomagnesemia.
Quick Reference Summary Table
| Disease | Rate | Rhythm | P Waves | PR | QRS | ST/T Changes | Key Feature |
|---|---|---|---|---|---|---|---|
| STEMI | Normal/fast | Regular | Normal | Normal | Usually normal | ST elevation territory | Pathological Q waves evolve |
| NSTEMI/UA | Normal/fast | Regular | Normal | Normal | Normal | ST depression / T inversion | No Q waves |
| Atrial Fibrillation | 100-160 | Irregularly irregular | Absent (f waves) | None | Normal | Variable | No P waves |
| Atrial Flutter | ~150 (2:1) | Regular | Sawtooth F waves ~300 | Fixed ratio | Normal | None | "Sawtooth" baseline |
| Complete Heart Block | Atria 60-100; Ventricles 20-60 | AV dissociation | Normal, regular | Variable | Wide (ventricular escape) | None | P and QRS completely independent |
| LBBB | Normal | Regular | Normal | Normal | Broad ≥120 ms, M in V5-V6 | Discordant ST/T | W in V1, M in V6 |
| RBBB | Normal | Regular | Normal | Normal | Broad ≥120 ms, RSR' in V1 | Discordant T in V1 | "Rabbit ears" in V1 |
| HCM | Normal | Regular (may have AF) | ±LA abnormality | Normal | Normal-wide | LVH voltage, lateral T inversion | Deep narrow septal Q waves (V5-V6) |
| WPW | Normal | Regular (sinus) | Normal | Short <120 ms | Broad (fusion) | Secondary changes | Delta wave |
| Long QT Syndrome | Normal | Regular (sinus) | Normal | Normal | Normal | Broad/notched T waves | QTc ≥450-500 ms, risk of TdP |
Sources: Guyton and Hall Textbook of Medical Physiology; Tintinalli's Emergency Medicine: A Comprehensive Study Guide; Goldman-Cecil Medicine; Textbook of Family Medicine; Morgan and Mikhail's Clinical Anesthesiology; Harrison's Principles of Internal Medicine 22E; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.