hiv associated lymphoma in TB negative patient and CD4 count more than 200
Reading File
Finding Sources
Finding Sources
Searching PubMed
"HIV" AND "lymphoma" AND "CD4"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
HIV-Associated Lymphoma in a TB-Negative Patient with CD4 Count >200
This is a clinically important scenario because the CD4 >200 context shifts the lymphoma profile significantly compared to advanced AIDS. Here is a structured breakdown.
Why Lymphoma Still Occurs Despite CD4 >200
Even with preserved CD4 counts and on effective ART, HIV-infected patients carry a persistently elevated lymphoma risk. Two distinct mechanisms drive this:
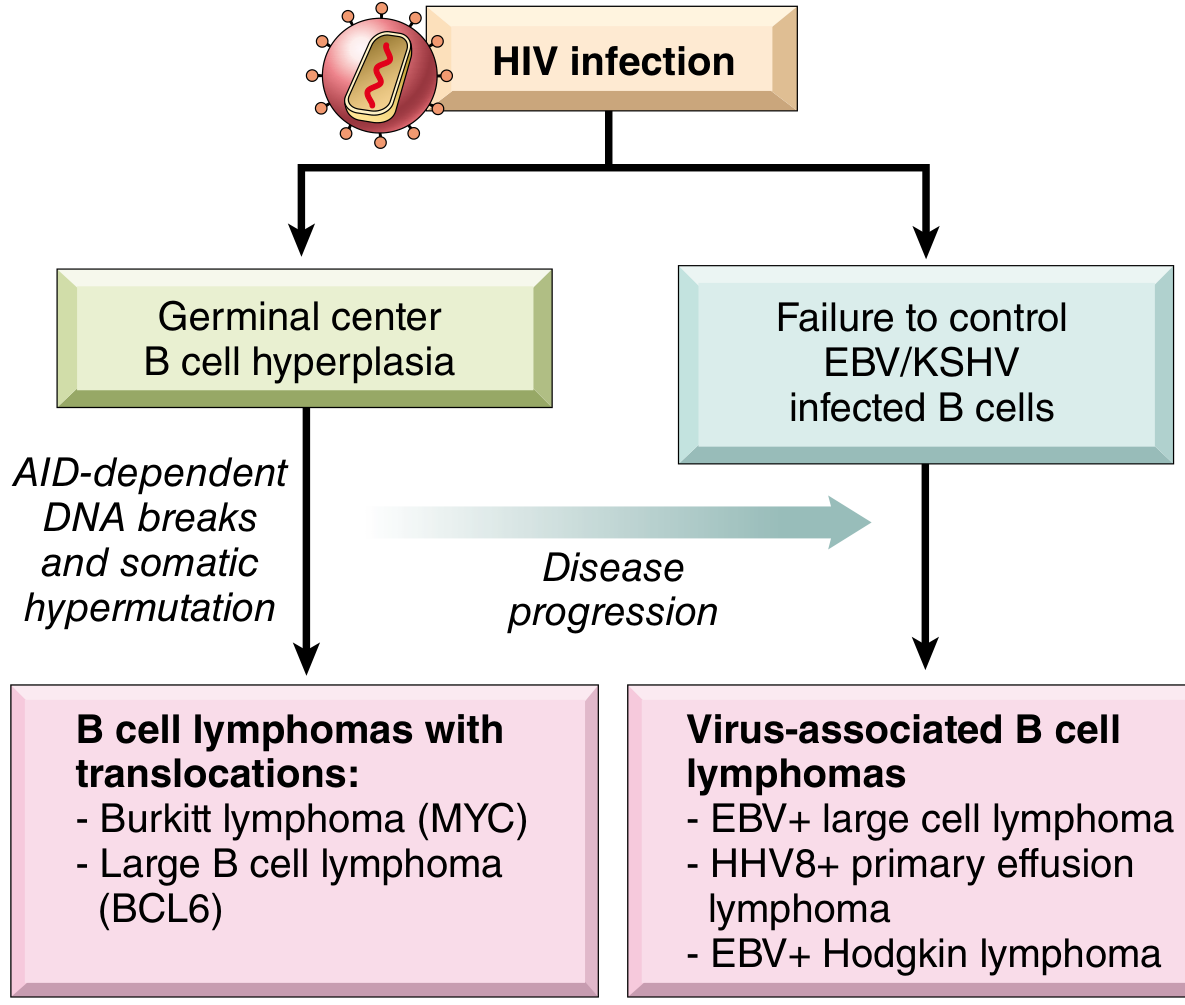
Mechanism 1 - Germinal center B-cell hyperplasia (CD4-independent pathway):
- Even with effective ART and normal/near-normal CD4 counts, HIV drives profound germinal center B-cell hyperplasia early in infection
- In germinal centers, B cells undergo somatic hypermutation and class switching - both processes involve AID-dependent DNA breaks, which are error-prone and can lead to oncogene translocations (MYC for Burkitt, BCL6 for DLBCL)
- Most lymphomas arising in patients with preserved CD4 counts are NOT associated with EBV or HHV-8 - they arise through this translocation-driven pathway
- This explains why the overall lymphoma rate remains elevated in HIV-infected patients even on ART with normal CD4 counts
Mechanism 2 - Failure to control EBV/KSHV-infected B cells (CD4-dependent pathway):
-
With significant immunosuppression (CD4 <200), cytotoxic T cells lose control of EBV/HHV-8-infected B cells
-
These then accumulate further mutations and develop into full-blown EBV+ or HHV-8+ lymphomas
-
At CD4 <50: Primary CNS lymphoma (median CD4 ~50/μL) - nearly 100% EBV+
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 244; Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 774
Types of HIV-Associated Lymphoma and Their CD4 Relationship
| Lymphoma Type | Typical CD4 | EBV/HHV-8 | Key Features |
|---|---|---|---|
| Burkitt lymphoma | Can occur even with CD4 >200 (earlier in HIV course) | 50% EBV+ | MYC translocation (t(8;14)); 1000x more common in HIV; highly curable |
| Diffuse Large B-Cell Lymphoma (DLBCL) | Variable; often earlier stage | ~40% EBV+ | Most common HIV lymphoma (~60%); systemic, extranodal |
| Plasmablastic lymphoma | Variable | EBV+, CD20- | Typically involves oral cavity/oropharynx |
| Primary CNS Lymphoma | Usually <50/μL | ~100% EBV+ | NOT the typical presentation at CD4 >200 |
| Primary Effusion Lymphoma (PEL) | Advanced AIDS | HHV-8 + EBV | Body cavity effusions; no discrete mass |
| Hodgkin Lymphoma | Variable (many have low CD4, but not always) | EBV+ Reed-Sternberg cells | 30x increased risk in HIV; Reed-Sternberg cells EBV+ |
At CD4 >200, Burkitt lymphoma and systemic DLBCL are the most likely diagnoses. Primary CNS lymphoma at CD4 >200 is uncommon. - Harrison's Principles of Internal Medicine 22E, p. 1656-1657
Clinical Presentation (at CD4 >200)
- At least 80% present with extranodal disease
- B symptoms (fever, night sweats, weight loss) in ~80% of cases
- Common extranodal sites: CNS (~1/3 of patients), GI tract (~25%), bone marrow (~20%), liver and lung (~10% each)
- Burkitt lymphoma: most frequent in patients aged 10-19 years; characteristic c-myc translocation
- Immunoblastic lymphoma: more common in older patients (>50 years, incidence >3%)
- Harrison's Principles of Internal Medicine 22E, p. 1656
Why TB Negativity Matters Here
The TB-negative status is clinically relevant for differential diagnosis. In an HIV patient presenting with:
- Lymphadenopathy + constitutional symptoms + TB-negative status
- The differential now favors lymphoma, Multicentric Castleman disease (MCD), or other malignancy over TB
TB and lymphoma can co-exist in HIV patients with low CD4 counts, and distinguishing them requires lymph node biopsy. At CD4 >200 (TB-negative), lymphoma moves to the top of the differential.
Pathology and EBV Association
- ~40% of HIV-related lymphomas overall are EBV-associated
- At higher CD4 counts, EBV-negative lymphomas predominate (driven by germinal center hyperplasia/translocation mechanism)
- EBV-negative Burkitt lymphoma and DLBCL are the key entities at CD4 >200
- African Burkitt: 97% EBV+; HIV-associated Burkitt: only 50% EBV+ - highlighting the different pathogenic pathway
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 774; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 244
Management Principles
-
ART (antiretroviral therapy) - cornerstone; has substantially reduced lymphoma incidence and improves outcomes in those who develop it
- Use ART regimens that avoid myelosuppressive antiretrovirals (to reduce synergistic toxicity with chemotherapy)
- Avoidance of cobicistat or HIV protease inhibitors - risk of drug-drug interactions with chemotherapy
-
Chemotherapy - standard combination chemotherapy (R-CHOP or CHOP-based regimens for DLBCL; DA-EPOCH-R for Burkitt)
- Rituximab (anti-CD20) added for CD20+ tumors - has significantly improved outcomes
- At CD4 >200: response rates up to 72%, median survival 33 months, disease-free intervals up to 9 years have been reported
- Goldman-Cecil Medicine, p. 479; Harrison's 22E, p. 1657
-
CNS prophylaxis - important since ~20% of systemic lymphoma patients have leptomeningeal involvement; lumbar puncture is mandatory in staging
-
Emerging therapies - CAR T-cell therapy is now being explored for HIV-positive lymphoma patients (per Hattenhauer et al., 2023)
-
Supportive care - growth factor support (G-CSF) to allow full-dose chemotherapy
Prognosis
- Patients with higher CD4 counts fare better but not as well as HIV-negative lymphoma patients
- Burkitt lymphoma in particular is considered highly curable with intensive chemotherapy
- Primary CNS lymphoma (typically at CD4 <50) has poor prognosis: 2-year survival only 20-30%
- At CD4 >200 with systemic lymphoma and TB-negative status: better prognosis group overall
Recent Literature (2026)
A 2026 review in Current HIV Research (Liu Y et al., PMID 40916417) provides updated coverage of pathogenesis-to-treatment strategies for HIV-associated lymphomas, confirming that ART + rituximab-based chemotherapy remains the standard and outcomes continue to improve in the ART era.
Summary for the Clinical Scenario:
A TB-negative HIV patient with CD4 >200 presenting with lymphadenopathy/B symptoms most likely has Burkitt lymphoma or systemic DLBCL (EBV-negative, arising from germinal center B-cell hyperplasia). Lymph node biopsy is mandatory. Management is ART + combination chemotherapy ± rituximab (for CD20+ disease), with good expected outcomes given the relatively preserved immune function.
This is a shared conversation. Sign in to Orris to start your own chat.