Teach me full concept of tetracyclines pharmacology mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to write a comprehensive MBBS-level tetracyclines pharmacology lesson. Let me compile the full answer.
Tetracyclines - Complete Pharmacology (MBBS Level)
1. Introduction and Classification
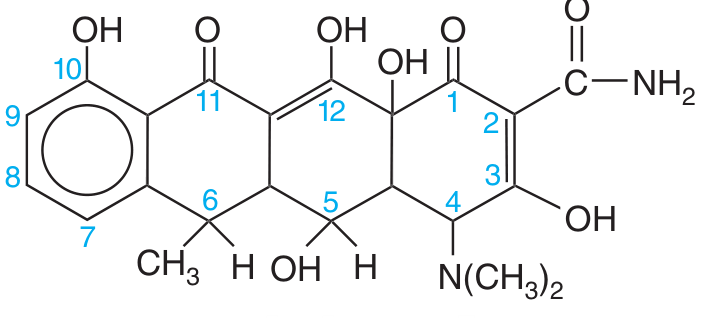
Tetracyclines are broad-spectrum bacteriostatic antibiotics derived from a basic four-ring (naphthacene) structure. They are one of the oldest classes of antibiotics, introduced in the late 1940s, and remain clinically relevant.
Here is the basic four-ring structure (shown for doxycycline):
Generations / Classification
| Generation | Drugs | Key Features |
|---|---|---|
| 1st generation | Tetracycline, Oxytetracycline, Chlortetracycline | Short half-life, incomplete absorption, renally excreted |
| 2nd generation (semisynthetic) | Doxycycline, Minocycline | Greater lipophilicity, longer half-life, once/twice daily |
| 3rd generation (newer derivatives) | Tigecycline (glycylcycline), Eravacycline (fluorocycline), Omadacycline (aminomethylcycline) | Overcome resistance mechanisms, broader spectrum |
Mnemonic: DC XY CYCLIN - Demeclocycline, Chlortetracycline, Oxytetracycline, Minocycline, Doxycycline, Tetracycline
2. Mechanism of Action
Tetracyclines inhibit bacterial protein synthesis by:
- Entering gram-negative bacteria by passive diffusion through porin channels in the outer cell membrane
- Then entering by active (energy-dependent) transport across the cytoplasmic membrane
- Binding to the 30S ribosomal subunit inside the cell
- Blocking aminoacyl-tRNA from accessing the acceptor (A) site on the mRNA-ribosome complex
- This prevents addition of new amino acids to the growing peptide chain
Result: Bacteriostatic (inhibit growth but do not kill)
Key point: Mammalian cells lack the active transport system used by bacteria to accumulate tetracyclines - this explains selective toxicity.
3. Antimicrobial Spectrum
Tetracyclines are truly broad-spectrum - a major advantage:
| Category | Organisms |
|---|---|
| Gram-positive cocci | Staphylococcus aureus (MSSA and MRSA - doxycycline/minocycline), Streptococcus pneumoniae (penicillin-susceptible), S. pyogenes |
| Gram-negative bacteria | Haemophilus influenzae, Neisseria gonorrhoeae, Vibrio cholerae, Brucella spp., Yersinia pestis (plague), Klebsiella granulomatis (granuloma inguinale) |
| Atypical organisms | Mycoplasma pneumoniae, Chlamydia trachomatis, Chlamydia psittaci |
| Rickettsiae | R. rickettsii (Rocky Mountain spotted fever), R. prowazekii (typhus) - drug of choice |
| Spirochetes | Borrelia burgdorferi (Lyme disease), Leptospira spp., Treponema pallidum (syphilis in penicillin allergy) |
| Others | Coxiella burnetii (Q fever), Ehrlichia, Actinomyces, Bacillus anthracis (anthrax), Mycobacterium marinum |
| Protozoa | Some activity (amoebiasis - not preferred) |
Note: Gram-positives are intrinsically more susceptible than gram-negatives because gram-negatives can efflux tetracyclines.
4. Mechanisms of Resistance
Three major mechanisms:
A. Efflux Pumps (most common)
- Genes encode membrane proteins that actively pump tetracycline out of the bacterial cell
- Plasmid-mediated, easily transferred
- Minocycline and doxycycline are more resistant to efflux (lower MICs)
- Newer agents (tigecycline, eravacycline) have structural modifications that reduce affinity for efflux pumps
B. Ribosomal Protection Proteins
- Proteins bind the tetracycline-ribosome complex and dislodge the drug, leaving the binding site available for tRNA
- Newer generation agents overcome this by enhanced ribosome binding affinity
C. Enzymatic Inactivation ("Destructases")
- Less common - enzymes modify the tetracycline molecule
D. Mutation at ribosomal target site
- Rare
Cross-resistance: Organisms susceptible to tetracycline are susceptible to doxycycline and minocycline - but resistance to tetracycline does NOT reliably predict resistance to doxycycline/minocycline.
5. Pharmacokinetics (ADME)
Absorption
| Drug | Oral Absorption | Food Effect |
|---|---|---|
| Tetracycline | ~60-80% (incomplete) | Significantly reduced - must take on empty stomach |
| Doxycycline | ~90% | Not affected by food or dairy |
| Minocycline | ~90% | Not significantly affected |
| Tigecycline / Eravacycline | IV only | N/A |
| Omadacycline | ~33% oral | Take ≥4 h after, ≥2 h before meals |
Critical chelation interaction: Divalent and trivalent cations (Ca²⁺, Mg²⁺, Al³⁺, Fe²⁺/³⁺, Zn²⁺) chelate tetracyclines and drastically impair absorption. Therefore:
- Dairy products, antacids, iron supplements, zinc, bismuth subsalicylate all reduce absorption
- Tetracycline must be taken 1 hour before or 2 hours after these products
Distribution
- Widely distributed throughout the body including urine and prostate
- Accumulate in: liver (reticuloendothelial cells), spleen, bone marrow, bone, dentine and enamel of unerupted teeth
- Cross the blood-brain barrier even without meningeal inflammation
- Cross the placenta - enter fetal circulation and amniotic fluid
- Found in high concentrations in breast milk
Metabolism and Excretion
| Drug | Primary Excretion | Dose Adjustment |
|---|---|---|
| Tetracycline | Kidneys (renal) | Reduce/avoid in renal failure |
| Doxycycline | Feces (biliary) + urine (unchanged) | No adjustment in renal or hepatic failure - safest in renal impairment |
| Minocycline | Liver (extensively metabolized) | No accumulation in hepatic failure |
| Tigecycline | Bile/feces (unchanged) | Dose adjustment in severe hepatic impairment |
Half-lives:
- Tetracycline: 6-8 hours (dose 4x/day)
- Doxycycline: ~16-22 hours (dose once or twice daily)
- Minocycline: ~16 hours (dose twice daily)
Enterohepatic recirculation: Tetracycline is concentrated in bile and partially reabsorbed - this extends its effect but also enables accumulation.
6. Therapeutic Uses / Clinical Indications
Infections where tetracyclines (especially doxycycline) are drug of choice (DOC):
| Condition | Organism | Drug |
|---|---|---|
| Rocky Mountain spotted fever | Rickettsia rickettsii | Doxycycline |
| Typhus (scrub, murine, epidemic) | Rickettsia spp. | Doxycycline |
| Q fever | Coxiella burnetii | Doxycycline |
| Ehrlichiosis / Anaplasmosis | Ehrlichia, Anaplasma | Doxycycline |
| Lyme disease (early) | Borrelia burgdorferi | Doxycycline |
| Chlamydia (urogenital, LGV) | Chlamydia trachomatis | Doxycycline |
| Psittacosis / atypical pneumonia | Chlamydia psittaci, Mycoplasma | Doxycycline |
| Brucellosis | Brucella spp. | Doxycycline + Streptomycin/Rifampicin |
| Tularemia | Francisella tularensis | Doxycycline |
| Plague | Yersinia pestis | Doxycycline |
| Cholera | Vibrio cholerae | Doxycycline (single dose) |
| Granuloma inguinale | Klebsiella granulomatis | Doxycycline |
| Anthrax (cutaneous/prophylaxis) | Bacillus anthracis | Doxycycline |
Other important uses:
- Acne vulgaris - doxycycline or minocycline (anti-inflammatory + antibacterial)
- Rosacea - doxycycline (low-dose anti-inflammatory)
- Malaria prophylaxis - doxycycline (causal prophylaxis for P. falciparum in chloroquine-resistant areas)
- SIADH - Demeclocycline (unique - blocks ADH action on collecting tubule; used in chronic SIADH)
- Sexually transmitted infections - non-gonococcal urethritis (Chlamydia)
- MRSA skin infections - doxycycline/minocycline
- Periodontal disease - subgingival doxycycline (Periochip)
- Bullous pemphigoid, dermatitis herpetiformis - tetracyclines (anti-inflammatory)
- Acinetobacter and doxycycline-resistant MRSA - minocycline
7. Adverse Effects
A. GI Effects (most common)
- Nausea, vomiting, epigastric pain, diarrhea
- Esophageal ulceration - if tablet taken without sufficient water (especially doxycycline)
- Superinfection / pseudomembranous colitis (C. difficile)
B. Teeth and Bone Effects
- Permanent discoloration of teeth (yellow-gray-brown) and dental enamel hypoplasia if given during tooth development (pregnancy - 2nd trimester onward, and children <8 years)
- Growth retardation of bones in premature/young infants
- Tetracyclines fluoresce under UV and bind to newly mineralized bone (used as a histological marker for bone formation rates)
C. Hepatotoxicity
- Dose-related fatty liver (especially with high IV doses or in pregnancy)
- Pancreatitis reported
D. Renal Effects
- Outdated/degraded tetracycline causes Fanconi syndrome (proximal tubular dysfunction - glycosuria, aminoaciduria, phosphaturia) - do NOT use expired tetracycline
- Worsens existing renal failure (antianabolic effect - increases nitrogen load)
- Demeclocycline causes nephrogenic diabetes insipidus (used therapeutically in SIADH)
E. Photosensitivity
- Doxycycline is especially associated with photosensitization (skin burns on sun exposure)
- Advise sunscreen use
F. CNS Effects
- Minocycline - vestibular toxicity (dizziness, vertigo, ataxia) - dose-related
- Intracranial hypertension (pseudotumor cerebri) - rare, especially in young women
G. Other
- Superinfection with Candida (oral or vaginal) or resistant organisms
- Anti-anabolic effect: increases BUN (blood urea nitrogen) by inhibiting protein synthesis - worsens uremia
- Lupus-like syndrome (minocycline - long-term use)
- Hyperpigmentation of skin, teeth, nails (minocycline - long-term)
8. Contraindications
| Contraindication | Reason |
|---|---|
| Pregnancy (Category D) | Teeth discoloration, bone growth retardation in fetus |
| Children < 8 years | Permanent teeth staining and enamel hypoplasia |
| Breastfeeding | High concentrations in breast milk |
| Renal failure | Tetracycline accumulates (use doxycycline if must use) |
| Expired tetracycline | Produces Fanconi syndrome |
Exception: Doxycycline is still used in children <8 years for life-threatening rickettsial infections - benefit outweighs risk.
9. Drug Interactions
| Interacting Drug/Substance | Effect | Mechanism |
|---|---|---|
| Antacids, dairy, iron, zinc, calcium | Reduced tetracycline absorption | Chelation with divalent/trivalent cations |
| Phenytoin, carbamazepine, barbiturates, alcohol | Reduced doxycycline levels | Enzyme induction - increased doxycycline metabolism |
| Warfarin | Increased anticoagulant effect | Gut flora suppression - less Vitamin K synthesis |
| Digoxin | Increased digoxin levels | Gut flora suppression - less digoxin metabolism in gut |
| Oral contraceptives | Possible reduced efficacy | Gut flora disruption (debated) |
| Penicillins | Antagonism - avoid combination | Tetracyclines (bacteriostatic) antagonize penicillin (needs actively dividing cells) |
| Methoxyflurane anesthesia | Renal failure | Synergistic nephrotoxicity |
10. Special Notes on Individual Drugs
Doxycycline
- Most widely used tetracycline today
- Long half-life (once or twice daily dosing)
- Safe in renal failure (excreted in feces)
- More lipophilic - better tissue penetration
- DOC for most rickettsial, chlamydial, spirochetal infections
Minocycline
- Most lipophilic - excellent CNS penetration
- Active against doxycycline-resistant MRSA and Acinetobacter
- Unique ADR: vestibular toxicity (dizziness, vertigo)
- Used for acne (long-term)
- Can cause lupus-like syndrome and hyperpigmentation with prolonged use
Demeclocycline
- Unique use: SIADH treatment - inhibits ADH effect on renal tubules, causing nephrogenic diabetes insipidus
- Causes photosensitivity
Tigecycline (glycylcycline)
- IV only
- Overcomes efflux pump and ribosomal protection resistance
- Broad spectrum including MRSA, VRE, multi-drug resistant gram-negatives
- NOT reliable for bacteremia (low serum levels due to extensive tissue distribution)
- NOT for urinary tract infections
11. Quick Comparison Table
| Feature | Tetracycline | Doxycycline | Minocycline |
|---|---|---|---|
| Oral absorption | 60-80% | ~90% | ~90% |
| Food effect | Reduced | No effect | No effect |
| Half-life | 6-8 h | 16-22 h | 16 h |
| Lipophilicity | Low | High | Highest |
| Excretion | Kidney | Feces + urine | Liver (metabolized) |
| Renal failure | Avoid | Safe | Safe |
| Special ADR | - | Photosensitivity | Vestibular toxicity |
| Dosing | 4x/day | Once-twice daily | Twice daily |
12. High-Yield MBBS Summary Points
- MOA: Bind 30S ribosome → block aminoacyl-tRNA from A site → bacteriostatic
- Chelation: Divalent cations (Ca, Mg, Fe, Al, Zn) reduce absorption - never take with dairy/antacids
- Teeth staining: Avoid in pregnancy and children <8 years
- Doxycycline is safe in renal failure - excreted by feces (unlike tetracycline which is renally cleared)
- Rickettsial infections (RMSF, typhus) - doxycycline is DOC, even in children if life-threatening
- Demeclocycline - used in SIADH (causes nephrogenic DI)
- Expired tetracycline - causes Fanconi syndrome
- Minocycline - vestibular toxicity (dizziness/vertigo)
- Doxycycline - photosensitivity
- Bacteriostatic - antagonizes bactericidal drugs like penicillins
- Resistance: mainly efflux pumps and ribosomal protection proteins (plasmid-mediated)
- Tetracyclines deposit in bone and newly mineralizing teeth - forms fluorescent complexes (used in bone histology)
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Fitzpatrick's Dermatology 5e; Comprehensive Clinical Nephrology 7e
This is a shared conversation. Sign in to Orris to start your own chat.