Explain about COPD
Reading File
Finding Sources
Searching PubMed
"chronic obstructive pulmonary disease" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative information from multiple textbooks. Let me compile the full answer.
Chronic Obstructive Pulmonary Disease (COPD)
Definition
COPD is a common, preventable, and treatable disease characterized by persistent, progressive airflow limitation that is not fully reversible. It most commonly manifests as emphysema and/or chronic bronchitis, and these two entities usually coexist in the same patient - though their relative contributions vary.
-
Emphysema: Enlargement of air spaces distal to terminal bronchioles due to destruction of alveolar walls
-
Chronic bronchitis: Clinically defined as a persistent productive cough for at least 3 consecutive months in at least 2 consecutive years
-
Robbins & Kumar Basic Pathology, p. 495
Epidemiology
COPD is the third most common cause of death in the United States, accounting for more than $40 billion per year in direct and indirect healthcare costs. It primarily affects patients older than 40 years and is more common in males, though the gender gap is narrowing. Only 15-30% of habitual smokers were historically thought to develop COPD, but radiographic studies now show progressive bronchial wall thickening and lung tissue loss even in smokers with normal spirometry.
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Risk Factors
| Factor | Details |
|---|---|
| Cigarette smoking | Major risk factor - induces inflammation, mucus overproduction, protease release |
| Age >40 years | Risk increases with age |
| Occupational exposures | Dust, chemicals, fumes |
| Indoor air pollution | Biomass fuel burning |
| Alpha-1 antitrypsin (AAT) deficiency | Most common monogenic cause; SERPINA1 gene mutation, leads to panacinar emphysema |
| Genetic factors | Multiple susceptibility loci beyond AAT |
Alpha-1 Antitrypsin Deficiency: AAT is a serine protease inhibitor (antiprotease) synthesized by the liver. Mutations cause polymerization of AAT in the liver with failure to secrete functional protein. Circulating levels fall to ~15% of normal, predisposing to emphysema and bronchiectasis. Allele frequency in White populations is 4-5%.
- Goldman-Cecil Medicine, p. 895
Pathophysiology
The Protease-Antiprotease Imbalance (Emphysema)
Smoking triggers recruitment of neutrophils and macrophages to the lung. These cells release proteases (including elastase, matrix metalloproteinases) that destroy the elastic support structures of alveolar walls. Normally, AAT neutralizes these enzymes. When the balance tips toward proteases - either from excess inflammation or AAT deficiency - alveolar wall destruction results, enlarging airspaces and reducing elastic recoil.
Mucus Dysfunction and Airway Obstruction (Chronic Bronchitis)
Cigarette smoke causes:
- Mucus overproduction: Surface epithelial mucous metaplasia, submucosal gland expansion, increased MUC5AC (10-fold) and MUC5B (3-fold) in severe COPD
- Ciliary dysfunction: Structural and functional changes; impaired mucociliary clearance
- Reduced airway surface liquid: Via decreased CFTR function and increased ENaC function
- Persistent infection: Particularly Haemophilus influenzae
Airflow Obstruction Mechanisms
By definition, COPD involves obstruction of expiratory airflow in small airways (<2 mm). Multiple mechanisms contribute:
- Airway smooth muscle constriction
- Small airway inflammation, wall thickening, and scarring
- Loss of small airways due to parenchymal destruction
- Dynamic airway collapse from loss of parenchymal tethering (emphysema)
- Decreased driving force from loss of elastic recoil
The result is a prolonged expiratory time and characteristic "coving" of the expiratory flow-volume loop.
Dynamic Hyperinflation
When expiratory time is shortened (increased respiratory rate), tidal volume is incompletely exhaled, leading to air trapping and elevated end-expiratory lung volume. This produces the classic barrel chest and contributes heavily to dyspnea even independent of hypoxemia.
- Goldman-Cecil Medicine, p. 895; Costanzo Physiology 7th Edition
Subtypes of Emphysema
| Type | Description | Association |
|---|---|---|
| Centriacinar (centrilobular) | Destruction begins at respiratory bronchioles, central acinus | Cigarette smoking (most common) |
| Panacinar (panlobular) | Uniform destruction of the entire acinus | Alpha-1 antitrypsin deficiency |
| Paraseptal (distal acinar) | Distal acinus near pleura | Spontaneous pneumothorax in young adults |
Clinical Features
Symptoms
- Progressive dyspnea on exertion (hallmark)
- Chronic productive cough (chronic bronchitis component)
- Wheezing and chest tightness
- Fatigue, weight loss in advanced disease
Signs
- Barrel chest (increased AP diameter) from hyperinflation
- Prolonged expiration, pursed-lip breathing
- Decreased breath sounds, hyperresonance
- Cyanosis ("blue bloater" - chronic bronchitis predominant)
- Pink, dyspneic appearance ("pink puffer" - emphysema predominant) - though most patients overlap
- Cor pulmonale (right heart failure) in advanced disease
Classic ABG Findings
From the Costanzo Physiology clinical case of a 65-year-old long-term smoker:
- PaO2 60 mmHg (low - due to V/Q mismatch)
- PaCO2 variable (low if hyperventilating; elevated in CO2 retainers)
- Elevated A-a gradient
Diagnosis
Spirometry (Gold Standard)
- Post-bronchodilator FEV1/FVC < 0.70 confirms airflow obstruction
- FEV1 is reduced; FVC is normal or near-normal
- The degree of FEV1 reduction determines GOLD grade
GOLD ABE Classification (Current)
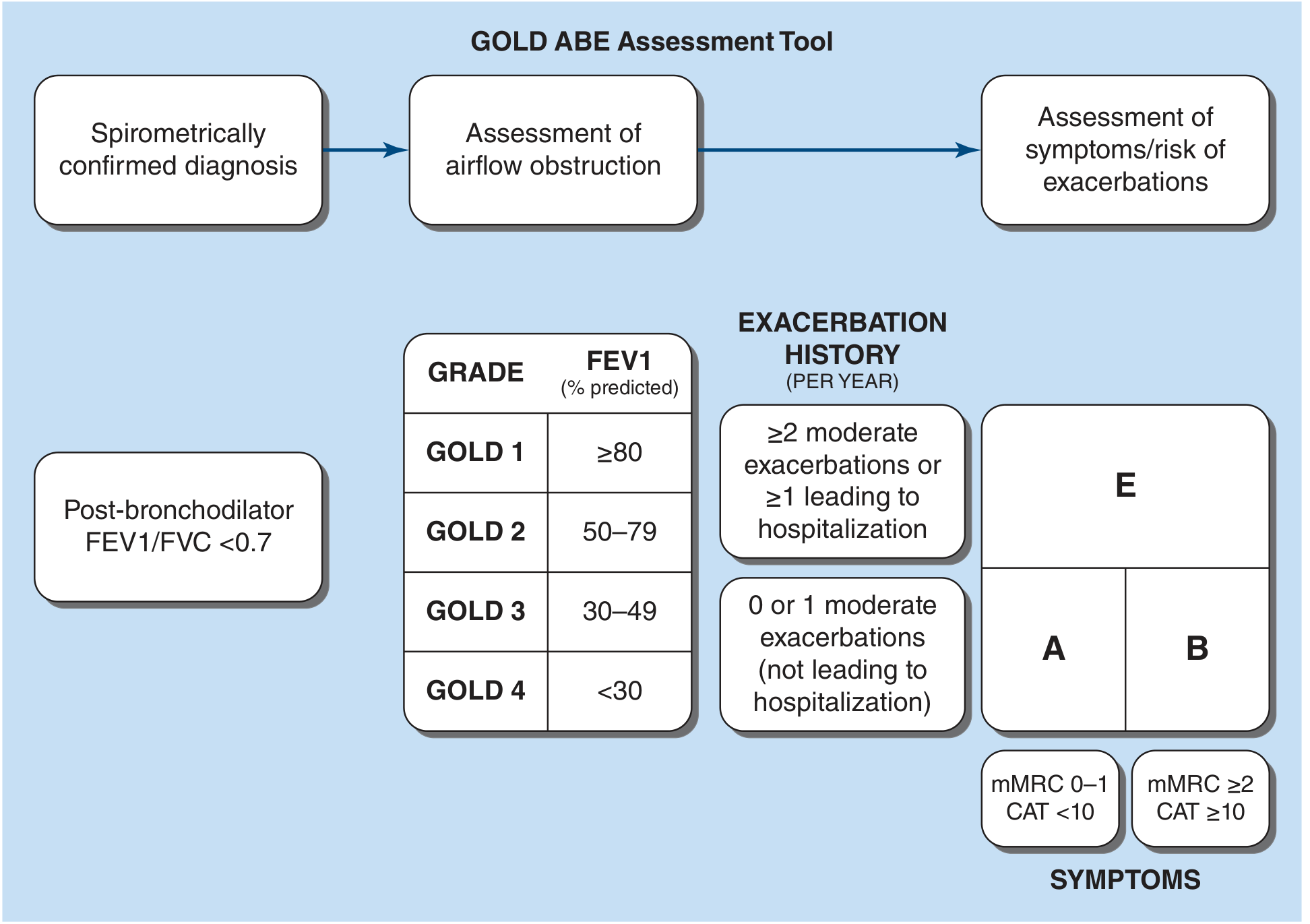
GOLD Grades by FEV1 (% predicted):
| Grade | FEV1 % predicted | Severity |
|---|---|---|
| GOLD 1 | ≥80% | Mild |
| GOLD 2 | 50-79% | Moderate |
| GOLD 3 | 30-49% | Severe |
| GOLD 4 | <30% | Very severe |
GOLD Groups (A, B, E) by symptoms + exacerbation history:
-
Group A: Low symptoms (mMRC 0-1, CAT <10) + 0-1 moderate exacerbations (not hospitalized)
-
Group B: High symptoms (mMRC ≥2, CAT ≥10) + 0-1 moderate exacerbations
-
Group E: ≥2 moderate exacerbations OR ≥1 hospitalization per year
-
Harrison's Principles of Internal Medicine 22E (2025)
Management
Interventions That Improve Survival
- Smoking cessation - most important; restores rate of FEV1 decline toward normal
- Long-term oxygen therapy (LTOT) - for chronically hypoxemic patients (PaO2 ≤55 mmHg, or ≤60 mmHg with cor pulmonale)
- Lung volume reduction surgery (LVRS) - in selected patients with upper-lobe-predominant emphysema
- Triple inhaled therapy (LABA + LAMA + ICS) - reduces mortality in selected patients
- Pulmonary rehabilitation - especially after COPD hospitalization
Pharmacotherapy
Bronchodilators (mainstay of treatment):
| Drug Class | Examples | Role |
|---|---|---|
| Short-acting beta-2 agonists (SABA) | Albuterol (salbutamol) | Acute symptom relief |
| Short-acting muscarinic antagonists (SAMA) | Ipratropium | Acute relief; improves FEV1 |
| Long-acting muscarinic antagonists (LAMA) | Tiotropium, umeclidinium, glycopyrronium, aclidinium | Mainstay for persistent symptoms; reduce exacerbations |
| Long-acting beta-2 agonists (LABA) | Salmeterol, formoterol, indacaterol, olodaterol, vilanterol | Symptom relief; reduce exacerbations |
| LABA + LAMA combinations | Multiple fixed-dose inhalers | Superior to monotherapy |
Inhaled Corticosteroids (ICS):
- Less central than in asthma
- Reserved for patients with severe airflow obstruction, frequent exacerbations, or asthma overlap
- Blood eosinophil count guides ICS use: eosinophils ≥300 cells/µL suggest likely benefit
- ICS are never used as monotherapy in COPD
- Associated with increased risk of bacterial pneumonia
Other agents:
- Roflumilast (PDE4 inhibitor): Improves pulmonary function and reduces exacerbation frequency in severe COPD with chronic bronchitis
- Theophylline: Evidence of limited benefit; a large RCT of low-dose theophylline failed to show reduction in exacerbation frequency
- Smoking cessation pharmacotherapy: Nicotine replacement therapy, bupropion, varenicline
Surgical / Bronchoscopic Interventions
-
LVRS: Thoracoscopic resection of hyperinflated upper-lobe tissue; contraindicated if FEV1 <20% predicted with low exercise capacity or DLCO <20%
-
Bronchoscopic lung volume reduction: One-way endobronchial valves, coils, or stents in patients with heterogeneous emphysema and intact interlobar fissures
-
Lung transplantation: Option for advanced COPD; median survival 5.8 years; ~75% now bilateral; accounts for ~25% of US lung transplants
-
Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Katzung's Pharmacology 16th Edition
Acute Exacerbations of COPD (AECOPD)
Definition: Acute worsening of dyspnea beyond the patient's usual state, plus increased cough and/or change in sputum character.
Key facts:
- Short-term mortality ~10%
- Account for ~60% of direct medical costs of COPD
- 75-80% involve viral or bacterial pathogens (rhinovirus, influenza, H. influenzae, S. pneumoniae, M. catarrhalis)
Management:
-
Short-acting bronchodilators (SABA ± SAMA) - first line
-
Systemic corticosteroids: Recommended due to inflammatory component
-
Antibiotics: Routinely given (unlike asthma) given frequent bacterial involvement; beta-lactams, macrolides, or fluoroquinolones
-
Supplemental oxygen: With careful titration to avoid CO2 retention
-
Noninvasive positive-pressure ventilation (NIPPV/BiPAP): For acute hypercapnic respiratory failure
-
Hospital admission for hypercarbia, acidemia, or significant distress despite bronchodilators
-
Goldman-Cecil Medicine; Katzung's Pharmacology 16th Edition
Complications
| Complication | Mechanism |
|---|---|
| Cor pulmonale | Chronic hypoxemia → pulmonary vasoconstriction → right heart failure |
| Pulmonary hypertension | Chronic hypoxic vascular remodeling |
| Secondary polycythemia | Erythropoietin stimulation from chronic hypoxemia |
| Respiratory failure | Progressive loss of lung function |
| Pneumothorax | Bullae rupture (especially in emphysema) |
| Lung cancer | Shared smoking etiology; COPD itself is an independent risk factor |
Recent Evidence (2024-2026)
A 2025 systematic review and meta-analysis on digital health interventions for COPD (PMID: 40418567) found that digital health tools (apps, telehealth, wearables) can improve outcomes in COPD patients - a growing area for management. A 2024 meta-analysis on AECOPD prognostic risk models (PMID: 39543648) showed that clinical prediction tools can meaningfully stratify mortality risk in acute exacerbations.
Sources: Robbins & Kumar Basic Pathology | Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine | Katzung's Basic and Clinical Pharmacology 16th Edition | Fishman's Pulmonary Diseases and Disorders | Costanzo Physiology 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.