Cvs Physiological changes in pregnancy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive, authoritative data from three major textbooks. Let me compile the full answer.
CVS Physiological Changes in Pregnancy
Pregnancy imposes dramatic, well-coordinated cardiovascular adaptations beginning as early as 5-6 weeks of gestation. These are driven primarily by hormonal changes (progesterone, estrogen, relaxin), placental vasodilation, and increased metabolic demand.
1. Blood Volume
| Parameter | Change |
|---|---|
| Total blood volume | +35% (1000-1500 mL at term; ~90 mL/kg) |
| Plasma volume | +40-55% (begins early, peaks at ~24-28 weeks) |
| Red blood cell mass | +45% |
- The disproportionate rise in plasma volume over RBC mass produces physiological (dilutional) anemia of pregnancy
- Hemoglobin usually remains >11 g/dL
- Reduced blood viscosity is a beneficial adaptation
- Morgan & Mikhail's Clinical Anesthesiology, p. 1575
2. Cardiac Output (CO)
The most important CVS change. CO rises 30-50% above pre-pregnancy baseline.
- Begins rising from 5 weeks after the last menstrual period
- Peaks at 28-34 weeks of gestation
- Begins to decline in late third trimester but does NOT return to pre-pregnancy values until 2-4 weeks postpartum
Mechanism by trimester:
- 1st & 2nd trimester: Rise primarily due to increased stroke volume (+30-40%), which peaks at 28-31 weeks
- 3rd trimester: Rise primarily due to increased heart rate (+10-15 bpm / ~20%)
- Twin pregnancies add a further 10-15% increase in CO
| Parameter | Change |
|---|---|
| Cardiac output | +40% at term |
| Stroke volume | +30% |
| Heart rate | +20% (~10-15 bpm above baseline) |
- Fuster and Hurst's The Heart, 15th Ed, p. 2209; Braunwald's Heart Disease, p. 1062
3. Blood Pressure
| Parameter | Change |
|---|---|
| Systolic BP | -5% (5-10 mmHg below baseline) |
| Diastolic BP | -15% (more pronounced fall) |
- Fall begins at 6-8 weeks, nadirs in the second trimester, then gradually rises back toward (but not above) pre-pregnancy values in the third trimester
- Driven by progesterone-mediated vasodilation, prostacyclin, and nitric oxide
- Fuster and Hurst's The Heart, p. 2209
4. Systemic Vascular Resistance (SVR) and Pulmonary Vascular Resistance (PVR)
| Parameter | Change |
|---|---|
| SVR | -15 to -50% |
| PVR | -30% |
- SVR falls early in pregnancy due to:
- Maturation of the uteroplacental low-resistance circulation
- Progesterone and estrogen effects
- Local vasodilators: prostacyclin and nitric oxide
- SVR nadirs at the end of the second trimester, then rises slightly in the third trimester
- Central venous pressure (CVP), pulmonary artery pressure (PAP), and pulmonary capillary wedge pressure (PCWP) remain unchanged
- Morgan & Mikhail, p. 1575; Fuster & Hurst, p. 2209
5. Cardiac Chambers and Structure
- Cardiac chambers enlarge - all four chambers dilate
- Myocardial hypertrophy is often seen on echocardiography
- Diaphragm elevation by the gravid uterus shifts the heart leftward and upward
- Gives the appearance of cardiomegaly on plain chest X-ray
- Produces left-axis deviation on ECG
6. ECG and Chest X-Ray Changes in Normal Pregnancy
ECG:
- Sinus tachycardia
- Premature atrial or ventricular complexes
- Left QRS axis deviation
- Inferior Q waves
- T wave flattening or inversion
- ST depression
- Increased R/S ratio in right precordial leads
Chest X-Ray:
-
Apparent cardiomegaly
-
Straightening of the left upper cardiac border
-
Horizontal positioning of the heart
-
Increased pulmonary vascular markings
-
Small pleural effusions (especially postpartum)
-
Braunwald's Heart Disease, p. 1062
7. Cardiac Examination Findings in Normal Pregnancy
These are NORMAL and must be distinguished from pathology:
- Collapsing (water-hammer) arterial pulses
- Prominent jugular venous pulsations (without elevated JVP)
- Laterally displaced apical impulse
- Palpable right ventricle or pulmonary trunk
- Soft, short ejection systolic murmur (grade I-II) at the pulmonary area or left sternal border - due to increased flow
- Exaggerated splitting of S1
- Third heart sound (S3) - may be audible (physiological)
- Small, asymptomatic pericardial effusion in some women
- Braunwald's Heart Disease, p. 1062; Morgan & Mikhail, p. 1576
8. Hemodynamics During Labor and Delivery
CO increases dramatically at this stage:
| Stage | CO Increase (vs. prelabor) |
|---|---|
| Early labor | +15 to 25% |
| Active labor | +50% |
| Immediately postpartum | +60 to 80% |
Mechanisms: catecholamine surge, autotransfusion from uterine contractions (300-500 mL blood shifted into circulation with each contraction), relief of IVC compression, and pain.
- Fuster & Hurst, p. 2209; Braunwald's Heart Disease, p. 1062
9. Aortocaval Compression (Supine Hypotension Syndrome)
- From week 20 onward, the enlarging uterus compresses the inferior vena cava when supine, reducing venous return and CO
- About 5% of women at term develop frank supine hypotension syndrome: hypotension, pallor, sweating, nausea/vomiting
- The aorta is also compressed, reducing uteroplacental perfusion
- Management: Left lateral tilt (>15° wedge under right hip)
- Uterine contraction reduces IVC compression but worsens aortic compression
- Chronic partial IVC obstruction causes lower limb edema, venous stasis, and dilated epidural veins
- Morgan & Mikhail, p. 1576
10. Postpartum Changes
- Heart rate falls ~14% within 48 hours of delivery
- Cardiac output does not fully normalize until 2 weeks postpartum
- Complete resolution of all hemodynamic changes may take up to 6 months
- The first week postpartum is a critical period - fluid mobilization can precipitate heart failure in susceptible women (cardiomyopathy, severe outflow obstruction)
Summary Table (Maximum Changes at Term)
| Parameter | Change |
|---|---|
| Plasma volume | +55% |
| Blood volume | +35% |
| Cardiac output | +40% |
| Stroke volume | +30% |
| Heart rate | +20% |
| Systolic BP | -5% |
| Diastolic BP | -15% |
| SVR | -15 to -50% |
| PVR | -30% |
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e, p. 1572-1576; Fuster and Hurst's The Heart 15th Ed, p. 2209; Braunwald's Heart Disease, p. 1062
Heart block in pregnancy and anesthetic management
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
heart block in pregnancy anesthetic management complete AV block pacemaker labor delivery
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11973396
Finding Sources
I now have comprehensive information from authoritative textbooks and current clinical literature. Let me compile a thorough answer.
Heart Block in Pregnancy and Anesthetic Management
Part 1: Types of Heart Block Relevant to Pregnancy
Heart block in pregnancy falls into two distinct categories:
A. Maternal Heart Block - AV conduction disease in the pregnant woman herself
B. Congenital Heart Block (Fetal/Neonatal) - passively acquired by the fetus from maternal antibodies
Part 2: Maternal Heart Block in Pregnancy
Epidemiology and Causes
Sinus node dysfunction and atrioventricular (AV) block occur rarely in pregnancy in the absence of structural heart disease.
Causes include:
-
Congenital (most common cause of complete heart block in young women)
-
Autoimmune (SLE, anti-Ro/SSA antibodies)
-
Lyme disease
-
Cardiomyopathy / myocarditis
-
Valvular disease
-
Post-surgical (prior cardiac surgery)
-
Toxins, drugs
-
Fuster and Hurst's The Heart, 15th Ed, p. 2221
Why Pregnancy Is Particularly Challenging in Heart Block
Recall from CVS physiology: pregnancy requires a progressive rise in cardiac output of 30-50%. In early/mid pregnancy this is achieved by increased stroke volume, but in the third trimester, the rise in cardiac output depends predominantly on heart rate increase (10-15 bpm).
In complete heart block, the ventricular rate is fixed (typically 35-55 bpm from a junctional/ventricular escape rhythm). The patient cannot augment heart rate in response to:
- Increased metabolic demand of pregnancy
- Labor contractions (catecholamine surge)
- Hemorrhage
- Anesthetic-induced vasodilation
This inability to increase heart rate to compensate for the above means acute hemodynamic decompensation is a real risk, particularly during the third trimester and labor.
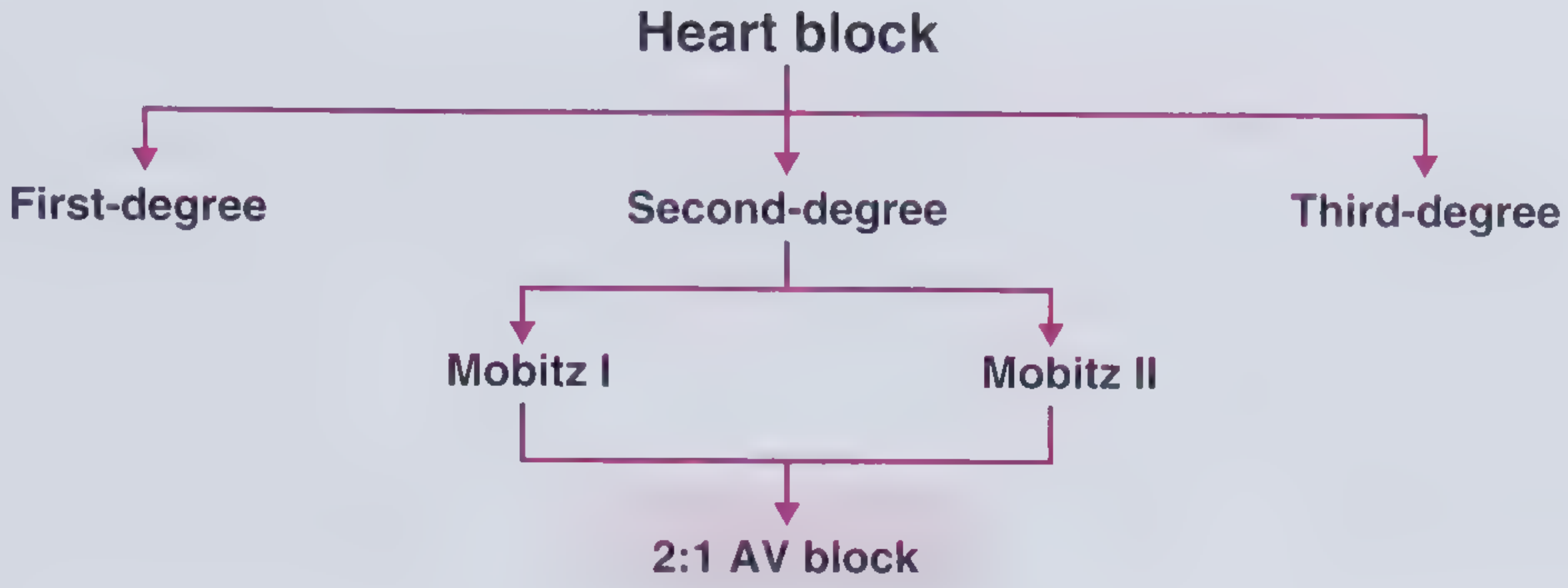
Classification and Management by Degree
First-Degree AV Block (PR > 200 ms)
- Generally well tolerated in pregnancy
- No specific intervention required
- Monitor for progression
Second-Degree AV Block
- Mobitz I (Wenckebach): usually benign; monitor
- Mobitz II: higher risk of progression to complete block; cardiology consultation; consider pacemaker if symptomatic
Complete (Third-Degree) AV Block
This is the most clinically significant:
| Scenario | Management |
|---|---|
| Asymptomatic, pre-existing complete heart block | Can be managed expectantly; generally does NOT require prophylactic temporary pacing during labor/delivery even with Valsalva |
| Asymptomatic pre-pregnancy → develops symptoms during pregnancy | Requires permanent pacemaker |
| Symptomatic at any point | Permanent pacemaker placement |
| Emergency | Transcutaneous pacing until transvenous pacing is possible |
- Fuster and Hurst's The Heart, 15th Ed, p. 2221
Pacemaker Implantation During Pregnancy:
- Can be placed safely during pregnancy
- Use echocardiographic guidance to minimize or eliminate radiation exposure to the fetus
- If fluoroscopy is required, lead shielding of the uterus is mandatory
Unknown Role of Rate Programming:
- Whether pacemaker settings should be increased during pregnancy to augment cardiac output remains under investigation
- Prophylactic pacing of asymptomatic women provides no benefit
- Fuster and Hurst, p. 2221
Part 3: Anesthetic Management of Heart Block in Pregnancy
This is a high-stakes scenario requiring multidisciplinary planning (obstetrics, cardiology, electrophysiology, anesthesiology, neonatology).
Pre-Anesthetic Assessment
- Cardiology/electrophysiology review - degree of block, hemodynamic stability, pacemaker status
- Echocardiography - assess cardiac function, rule out structural disease
- Holter monitor - document heart rate range (typically 37-53 bpm in complete heart block)
- Electrolytes - K⁺ > 4.0 mEq/L, Mg²⁺ > 2.0 mg/dL (hypokalemia and hypomagnesemia worsen conduction)
- Assess pacemaker function if already implanted
- Discuss pacing strategy - transcutaneous pads, temporary transvenous, or permanent pacemaker
Monitoring (Intraoperative)
- Continuous ECG
- Invasive arterial line (radial artery) - for beat-to-beat BP and HR monitoring
- Large-bore IV access (minimum two 16G cannulas)
- Transcutaneous pacing pads applied prophylactically - even in asymptomatic patients during cesarean delivery
- Consider pulmonary artery catheter in severe disease
Choice of Anesthesia
Neuraxial Anesthesia (Regional) - Preferred
Both epidural and spinal have been used successfully:
Epidural (preferred for labor and elective LSCS):
- Allows slow, titrated onset - avoids sudden sympathectomy and hypotension
- Slow incremental dosing: e.g., 0.5% bupivacaine + 2% lidocaine in 5 mL increments to T4 level
- Labor analgesia: 0.2% ropivacaine at 10 mL/hr via epidural infusion pump
- Avoids catecholamine surges of pain that could destabilize hemodynamics
- Atropine 0.2 mg given prophylactically to prevent bradycardia during block establishment
Spinal (acceptable for emergency LSCS):
- Used with low-dose local anesthetic (e.g., levobupivacaine) to minimize sympathectomy
- Co-loading with IV fluids preferred over pre-loading (reduces risk of fluid overload in a patient with fixed heart rate who cannot compensate for volume shifts)
- Transcutaneous pacing on standby
Key principle: Hypotension in heart block cannot be corrected by the normal compensatory tachycardia - treatment relies on vasopressors (phenylephrine, norepinephrine) and fluid management.
General Anesthesia - Reserved for:
- Failed regional / emergency where there is no time for regional
- Patient refusal
- Coagulopathy
Risks of GA in heart block:
- Laryngoscopy/intubation can precipitate bradycardia (vagal response)
- Volatile agents can depress the escape rhythm further
- Atropine and ephedrine should be drawn up and ready
- Temporary pacing must be available
Vasopressor Choice
| Vasopressor | Comment |
|---|---|
| Phenylephrine | Preferred - pure alpha agonist, corrects hypotension without causing tachycardia (which the patient can't achieve anyway) |
| Ephedrine | Mixed alpha/beta - use if bradycardia is also a concern |
| Norepinephrine | Acceptable alternative |
| Atropine | For acute bradycardia; limited efficacy in complete block (AV node bypassed) |
| Isoprenaline (isoproterenol) | Can accelerate the ventricular escape rhythm - useful temporizing measure |
| Epinephrine | For cardiac arrest/severe decompensation |
Labor Management
- Vaginal delivery is possible in asymptomatic, hemodynamically stable women with complete heart block
- Shorten the second stage with instrumental delivery (forceps/vacuum) to avoid prolonged Valsalva-induced decreased venous return
- Continuous fetal monitoring mandatory
- Uterine contractions cause autotransfusion of 300-500 mL per contraction - this increases preload but also triggers catecholamine surges
- Have temporary transcutaneous pacing immediately available throughout labor
Mode of Delivery
- Vaginal delivery is feasible in stable patients
- Elective (planned) cesarean section often preferred in symptomatic or hemodynamically compromised patients to allow controlled, optimized conditions
Postpartum
- Cardiac output increases 60-80% in the immediate postpartum period (autotransfusion from uterine involution)
- First week postpartum: fluid mobilization can cause acute volume overload in patients with fixed-rate hearts
- Cardiology and electrophysiology follow-up for all patients
- Patients who were asymptomatic during pregnancy may develop symptoms postpartum requiring permanent pacemaker
- Example: one case report patient developed exertional dyspnea 2 months postpartum and required pacemaker implantation
Part 4: Congenital Heart Block (Fetal/Neonatal) - Due to Maternal Antibodies
Mechanism
Mothers with anti-Ro/SSA and/or anti-La/SSB antibodies (seen in SLE, Sjögren's syndrome, and other CTDs) transfer these IgG antibodies across the placenta. These antibodies target the fetal cardiac conduction system, causing inflammation and fibrosis of the AV node.
Risk
| Scenario | Risk of CCHB |
|---|---|
| Anti-Ro/SSA positive mother, no prior history | ~2% |
| Prior child with complete heart block | 15-20% recurrence |
Screening
- Fetal echocardiography from 16-26 weeks in antibody-positive mothers
- Weekly echos from 16-26 weeks if prior child with NLE/heart block
- Detect early first- or second-degree block before progression to complete block
Treatment
| Intervention | Evidence |
|---|---|
| Fluorinated glucocorticoids (dexamethasone, betamethasone) | Considered for 1st/2nd degree block or cardiac inflammation; unproven for isolated CCHB |
| IVIG | Not proven effective |
| Hydroxychloroquine (HCQ) | PATCH study: >50% reduction in recurrence of CCHB - recommend for secondary prevention; consider for primary prevention |
| Plasmapheresis | Used in severe cases; efficacy unproven |
-
Isolated CCHB once established: no medical therapy proven beneficial
-
Severe forms: myocarditis, hydrops fetalis
-
Most neonates with CCHB require permanent pacemaker after birth
-
Creasy & Resnik's Maternal-Fetal Medicine, p. 2468-2470; Fuster and Hurst, p. 2220
Summary: Key Points for Anesthesia in Maternal Complete Heart Block
| Principle | Detail |
|---|---|
| Fixed heart rate | Cannot compensate for hypotension with tachycardia |
| Preferred anesthesia | Epidural (slow titration) for labor and LSCS |
| Pre-op prep | Arterial line, 2 large-bore IVs, transcutaneous pacing pads |
| Fluid strategy | Co-loading (not aggressive pre-loading) to avoid overload |
| Vasopressor | Phenylephrine first-line |
| Pacing | Transcutaneous on standby; transvenous if symptomatic/unstable |
| Labor | Shorten second stage; continuous CTG |
| Postpartum | Vigilance for decompensation during fluid mobilization; cardiology follow-up |
Sources: Fuster and Hurst's The Heart 15th Ed, p. 2221; Creasy & Resnik's Maternal-Fetal Medicine; PMC case report: Anesthetic Considerations for Cesarean Delivery in CHB; Sundararaman et al., J Clin Anesth 2016
1 &3
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Here is the detailed answer covering Part 1 (Types of Heart Block) and Part 3 (Anesthetic Management):
Part 1: Types of Heart Block - Full Classification
Anatomy of the AV Conduction System
The AV node is supplied by the AV nodal artery, which arises from the:
- Right coronary artery in 80-90% of patients
- Left circumflex in 10%
- Both in 10%
The bundle of His and bundle branches have dual blood supply from:
- Septal perforators of the left anterior descending (LAD) artery (LBB and proximal RBB)
- Branches of the posterior descending artery
Critical point: The AV node is heavily innervated by both sympathetic and parasympathetic nerves. However, the bundle of His and distal conduction system are NOT influenced by autonomic tone - this is why atropine works for nodal block but NOT for infranodal (Mobitz II/complete) block.
- Harrison's Principles of Internal Medicine 22E, p. 1969
First-Degree AV Block
Definition: Prolonged PR interval >200 ms (0.20 sec) with ALL atrial impulses conducted to the ventricles. Every P wave is followed by a QRS - there are no dropped beats. The term "block" is a misnomer; it is delayed conduction, not true block.
Site of delay: Usually within the AV node (occasionally in atria, His bundle, or Purkinje system)
ECG:
- PR interval >200 ms, constant
- 1:1 P:QRS ratio
- No dropped beats
Symptoms:
- Generally asymptomatic
- Severe cases (PR >300 ms): dyspnea and light-headedness that worsen with exercise due to loss of AV synchrony
Causes:
- Idiopathic fibrosis (Lenègre's disease, Lev's disease)
- Medications: beta-blockers, digoxin, calcium channel blockers, amiodarone
- Enhanced vagal tone (athletes)
- Electrolyte disturbances (hypokalemia)
- Inferior myocardial ischemia/infarction
- Endocarditis, myocarditis
- Lyme disease
- Muscular dystrophies (myotonic dystrophy)
- Infiltrative disease (amyloidosis)
Prognosis: Generally benign. Slight increased risk of progression to AF and other conduction abnormalities.
Treatment: Usually none required. Symptomatic cases: address reversible causes; pacemaker rarely needed.
In pregnancy: Well tolerated. Monitor for progression.
- Frameworks for Internal Medicine, p. 47; Miller's Anesthesia 10e, p. 12222
Second-Degree AV Block
Intermittent failure of conduction - some P waves are NOT followed by a QRS (dropped beats).
Type 1: Mobitz I (Wenckebach)
ECG pattern:
- Progressive lengthening of the PR interval before a suddenly dropped QRS
- After the dropped beat, the PR interval resets to its shortest value
- RR intervals progressively shorten before the dropped beat (grouped beating)
- The greatest PR discrepancy is between the last conducted beat before the dropped beat and the first beat after
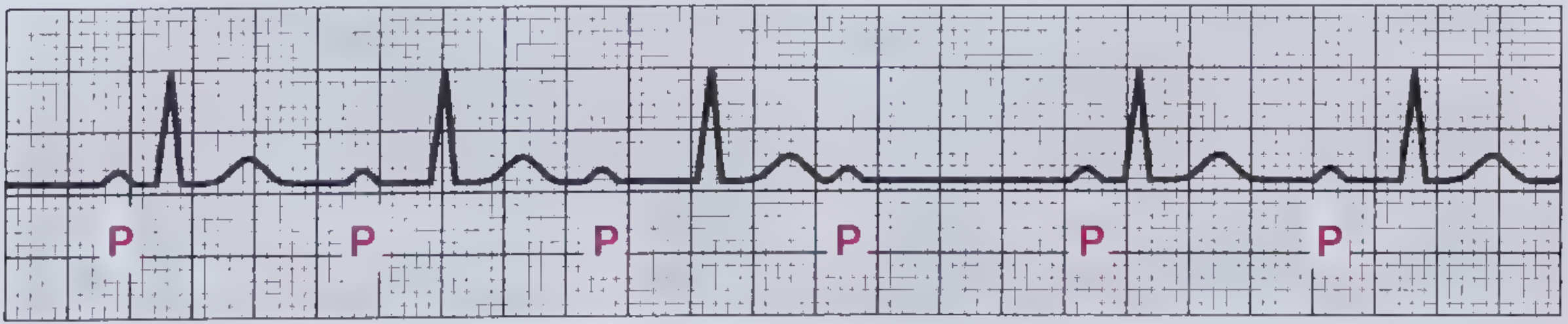
Site of block: AV node (nodal)
Associated MI territory: Right coronary artery - inferior MI (ST elevation in II, III, aVF)
Symptoms: Usually asymptomatic. May cause mild palpitations/light-headedness.
Prognosis: Hemodynamically stable. Does NOT typically warrant pacing in the absence of symptoms.
Treatment: Address reversible causes. No pacing required if asymptomatic and hemodynamically stable.
In pregnancy: Monitor; generally does not worsen or require intervention.
Type 2: Mobitz II
ECG pattern:
- Fixed PR interval (no progressive prolongation)
- Sudden, unexpected dropped QRS - without any warning prolongation of PR
- QRS is often wide (bundle branch block pattern) reflecting infranodal disease
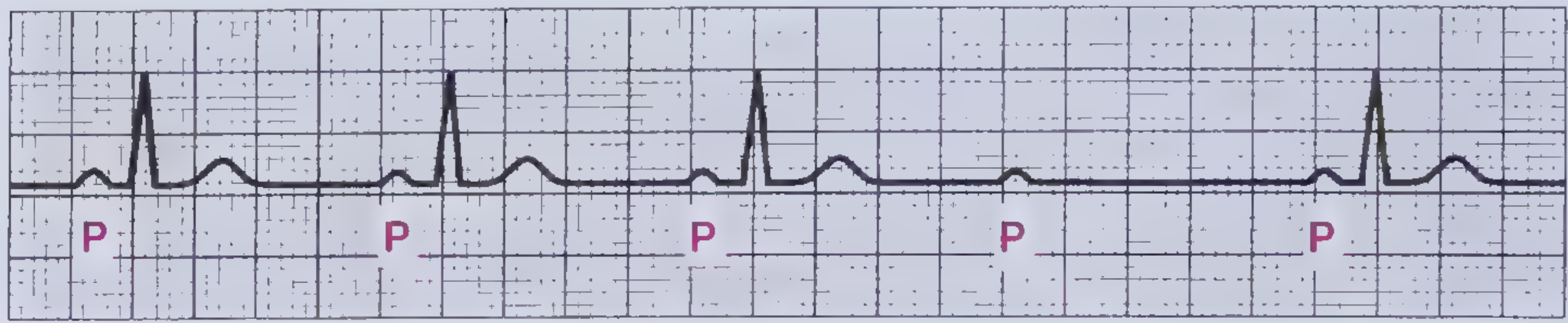
Site of block: Below the AV node - within the His-Purkinje system or bundle branches (infranodal)
Associated MI territory: Left anterior descending (LAD) artery - anterior MI (ST elevation in V1-V4)
Symptoms: Frequently symptomatic - dyspnea, palpitations, light-headedness, syncope.
Prognosis: Serious. High rate of progression to complete (third-degree) heart block. Associated with increased mortality. Risk of sudden death.
Treatment: Permanent pacemaker is almost always required even in asymptomatic patients due to unstable nature and risk of sudden death. If acutely symptomatic/unstable: dopamine infusion or temporary pacing as a bridge.
In pregnancy: High risk - refer for permanent pacemaker. Temporary pacing standby during labor.
Special Case: 2:1 AV Block
- Alternating conducted and non-conducted beats (every other P wave is dropped)
- Cannot be classified as Mobitz I or Mobitz II on ECG alone (can't assess PR trend with only one conducted beat between drops)
- Clues favoring infranodal (Mobitz II) block: PR <160 ms, wide QRS
- Clues favoring nodal (Mobitz I) block: narrow QRS, PR >160 ms, responds to atropine
- Infranodal 2:1 block: permanent pacemaker required
Third-Degree (Complete) Heart Block
Definition: Complete AV dissociation - NO atrial impulses reach the ventricles. The atria and ventricles beat independently.
ECG:
- P waves at their own rate (atrial rate > ventricular rate)
- QRS complexes at their own (slower) rate from an escape rhythm
- P waves bear NO fixed relationship to QRS complexes
- P waves may fall within, before, or after QRS complexes randomly
ECG on previous answer showed: P waves at regular rate, wide QRS escape rhythm at slow rate, complete dissociation.
Site of block and escape rhythm:
| Level of Block | QRS Width | Escape Rate | Stability |
|---|---|---|---|
| AV node / proximal His | Narrow QRS | 40-60 bpm (junctional) | More stable |
| Bundle of His / bundle branches | Wide QRS | 20-40 bpm (ventricular/idioventricular) | Less stable, unreliable |
Narrow QRS escape = block is in the AV node or proximal His; rhythm is faster and more stable
Wide QRS escape = block is in the distal His or bundle branches; slower and unreliable - higher risk of asystole
Causes:
- Congenital (most common cause in young women presenting in pregnancy)
- Fibrosis/sclerosis of conduction system (Lenègre's, Lev's disease)
- Inferior or anterior MI
- Post-cardiac surgery
- Autoimmune (SLE, anti-Ro/SSA antibodies)
- Lyme disease, endocarditis, myocarditis
- Infiltrative (sarcoidosis, amyloidosis, hemochromatosis)
- Drugs (digoxin toxicity, beta-blockers, CCBs)
Symptoms: Syncope (Stokes-Adams attacks), severe dyspnea, heart failure, presyncope, fatigue. Ventricular rate typically 35-55 bpm.
Treatment: Permanent pacemaker in virtually all symptomatic patients. In pregnancy: echoguided implantation to minimize fetal radiation exposure.
- Harrison's 22E, p. 1969; Miller's Anesthesia 10e, p. 12222-12224; Frameworks for Internal Medicine, p. 47-49
Part 3: Anesthetic Management of Heart Block in Pregnancy - Deep Dive
Core Physiological Problem
In complete heart block, the ventricular rate is fixed by the escape pacemaker. Pregnancy normally requires a progressive heart rate increase (especially in the 3rd trimester) to augment cardiac output. In heart block:
- No compensatory tachycardia is possible
- Any fall in BP (from blood loss, regional anesthesia, aortocaval compression) cannot be corrected by reflex tachycardia
- Any increase in demand (labor contractions, pain, bleeding) cannot be met by rate increase
- The only compensatory mechanism available is increased stroke volume via increased preload - and this too is limited
Pre-Anesthetic Preparation
Investigations:
- 12-lead ECG + Holter monitor (document escape rate range, e.g., 37-53 bpm)
- Echocardiography: LV/RV function, wall motion, structural disease
- Electrolytes: K⁺ >4.0 mEq/L, Mg²⁺ >2.0 mg/dL - normalize before any procedure (electrolyte abnormalities impair pacing capture)
- Blood group and cross-match (hemorrhage tolerated poorly)
- Pacemaker check if device already in situ
MDT Planning:
- Obstetrics + Cardiology + Electrophysiology + Anesthesiology + Neonatology
- Determine pacing strategy BEFORE labor starts:
- Transcutaneous pacing pads (all patients)
- Temporary transvenous pacing (symptomatic/hemodynamically unstable)
- Permanent pacemaker (if not already placed and patient is symptomatic)
Pacing Strategy
| Patient Status | Pacing Approach |
|---|---|
| Asymptomatic, hemodynamically stable | Transcutaneous pads on standby; expectant management; no prophylactic pacing needed |
| Symptomatic (syncope, dyspnea, hemodynamic compromise) | Permanent pacemaker before or during pregnancy (echoguided) |
| Emergency labor/LSCS without pacemaker | Transcutaneous pacing immediately; convert to transvenous as soon as possible |
| Pacemaker in situ | Check settings; consider rate programming adjustment |
Why atropine is INEFFECTIVE in Mobitz II and complete heart block:
- Atropine reverses parasympathetic (vagal) effects on the AV node
- In Mobitz II and complete heart block, the block is infranodal (His-Purkinje system) - which has NO vagal innervation
- Atropine cannot accelerate an idioventricular or infranodal escape rhythm
- May even worsen the situation by increasing the atrial rate while the ventricular rate stays fixed
"Atropine is not the preferred drug of choice for type II second-degree or third-degree AV block...these bradyrhythmias should be treated with transcutaneous pacing or β-adrenergic agonists as temporizing measures while the patient is prepared for transvenous pacing." - Miller's Anesthesia 10e, p. 12223
Drug Management of Bradycardia
| Drug | Dose | Mechanism | Role in Heart Block |
|---|---|---|---|
| Atropine | 1 mg IV q3-5 min; max 3 mg (avoid <0.5 mg - paradoxical bradycardia) | Antimuscarinic - blocks vagal tone on AV node | Only for nodal (Mobitz I, sinus bradycardia). NOT effective for Mobitz II or CHB |
| Dopamine | 2-20 mcg/kg/min IV | Alpha + beta adrenergic; rate + inotropy at lower doses, vasoconstriction at >10 mcg/kg/min | Second-line for bradycardia unresponsive to atropine |
| Epinephrine | 2-10 mcg/min infusion | Alpha + beta | Severe bradycardia/cardiac arrest |
| Isoproterenol (Isoprenaline) | 2-10 mcg/min IV infusion | Pure beta-1 and beta-2 agonist | Accelerates ventricular escape rhythm; useful temporizing measure in complete heart block while awaiting pacing; causes vasodilation |
| Phenylephrine | 50-100 mcg IV boluses | Pure alpha-1 | Treats hypotension without increasing heart rate - first choice for neuraxial anesthesia-induced hypotension |
| Ephedrine | 5-10 mg IV | Alpha + beta | Treats hypotension + raises heart rate; use if bradycardia co-exists |
Anesthetic Technique
For Labor Analgesia
Epidural - strongly preferred:
- Slow, titrated sympathectomy avoids sudden hemodynamic swings
- 0.2% ropivacaine at 10 mL/hr (or equivalent low-dose bupivacaine regimen)
- Maintains maternal comfort, blunts catecholamine surges of labor pain
- Epidural catheter can be used for subsequent cesarean if needed
For Cesarean Section (Elective)
Epidural (top-up of labor epidural) - preferred:
- Incremental boluses: e.g., 0.5% bupivacaine + 2% lidocaine in 5 mL increments
- Target T4 sensory block
- Slow titration gives cardiovascular stability
- Prophylactic atropine 0.2 mg IV before block establishment (to blunt any vagal response)
Spinal - acceptable (especially for emergency):
- Use low-dose hyperbaric bupivacaine (levobupivacaine 0.5% is preferred in some case series)
- Co-loading with IV crystalloid preferred over pre-loading:
- Pre-loading before spinal can cause volume overload in a fixed-rate heart (cannot increase rate to offload excess preload)
- Co-loading (infusing during block establishment) is more physiological
- Phenylephrine infusion to treat sympathectomy-induced hypotension
For Emergency Cesarean / Failed Regional
General Anesthesia:
- Higher risk - use only when regional is contraindicated or failed
- Rapid Sequence Induction (RSI) - aspiration prophylaxis mandatory in pregnancy
- Laryngoscopy can trigger vagal bradycardia - have atropine ready (though limited efficacy in CHB)
- Volatile agents depress the escape rhythm; use lowest effective concentration
- Avoid hypoxia, hypercarbia, acidosis - all worsen conduction disease and impair pacing capture
- Avoid drugs that depress conduction (high-dose propofol, suxamethonium vagal response, neostigmine - though neostigmine's effect is usually blocked by atropine given concomitantly)
Intraoperative Monitoring
| Monitor | Rationale |
|---|---|
| Continuous ECG | Detect rhythm changes, pacing capture failure |
| Invasive arterial line (radial artery, 20G) | Beat-to-beat BP + waveform; HR cannot be reliably detected from pulse in CHB |
| 2x Large-bore IV access (minimum 16G) | Rapid drug administration and volume resuscitation |
| Transcutaneous pacing pads | Immediately available pacing - mandatory in all CHB patients |
| SpO₂ | Oxygenation |
| Foley catheter | Fluid balance |
| Consider CVP line | Volume status in high-risk cases |
Labor Management
- Vaginal delivery is feasible in hemodynamically stable, asymptomatic patients
- Shorten the second stage with instrumental delivery (forceps or vacuum):
- Prolonged pushing + Valsalva → increased intrathoracic pressure → decreased venous return → decreased preload → CO falls → cannot compensate with tachycardia
- Left lateral tilt at all times to prevent aortocaval compression
- Continuous CTG monitoring
- Avoid oxytocin boluses (causes hypotension) - use slow infusion
Postpartum Vigilance
- The immediate postpartum period is hemodynamically the most volatile:
- Autotransfusion from uterine involution: 300-500 mL added to circulation per contraction
- CO rises 60-80% above prelabor values immediately postpartum
- Fluid mobilization over days 1-7 postpartum
- A patient with a fixed, slow escape rate who was compensated during pregnancy may decompensate postpartum
- Cardiology + electrophysiology follow-up mandatory
- Symptoms developing postpartum (exertional dyspnea, presyncope) warrant pacemaker implantation
Summary: Anesthetic Checklist for Heart Block in Pregnancy
PRE-OP
✓ MDT meeting: OB + Cardiology + EP + Anaesthesia + Neonatology
✓ Echo + Holter + electrolytes (K+ >4, Mg2+ >2)
✓ Permanent pacemaker if symptomatic
✓ Transcutaneous pacing pads available in all CHB patients
✓ Arterial line + 2x large-bore IV
ANALGESIA FOR LABOR
✓ Early epidural (low-dose, titrated)
✓ Left lateral tilt
FOR LSCS
✓ Epidural preferred (slow top-up) or low-dose spinal with co-loading
✓ Phenylephrine for hypotension
✓ Atropine drawn up (limited use in CHB - for vagal reactions only)
✓ Isoproterenol/dopamine available for escape rhythm support
GENERAL ANAESTHESIA (last resort)
✓ RSI + aspiration prophylaxis
✓ Avoid deep volatile anaesthesia
✓ Transcutaneous/transvenous pacing immediately available
POSTPARTUM
✓ Monitor Day 1-7 for fluid overload/decompensation
✓ Cardiology follow-up at 2 months
Sources: Miller's Anesthesia 10e, p. 12222-12224; Fuster and Hurst's The Heart 15th Ed, p. 2221; Frameworks for Internal Medicine, p. 47-49; Harrison's Principles 22E, p. 1969; PMC case - Anesthetic Considerations for Cesarean Delivery in CHB
Define stroke volume
Stroke volume (SV) is the volume of blood ejected by one ventricle per single contraction (heartbeat). Normal value is approximately 60-100 mL at rest.
Formula:
SV = End-Diastolic Volume (EDV) - End-Systolic Volume (ESV)
- EDV = volume in the ventricle after filling (preload) ~120-130 mL
- ESV = volume remaining after ejection ~50-60 mL
- SV = ~70 mL at rest
Ejection Fraction (EF) = SV/EDV × 100 = ~55-70% (normal)
Three determinants of SV:
| Determinant | Definition | Effect on SV |
|---|---|---|
| Preload | Ventricular filling pressure / stretch before contraction (EDV) | ↑ Preload → ↑ SV (Frank-Starling law) |
| Afterload | Resistance the ventricle must overcome to eject blood (SVR/wall stress) | ↑ Afterload → ↓ SV |
| Contractility | Intrinsic force of myocardial contraction (inotropy), independent of pre/afterload | ↑ Contractility → ↑ SV |
Relation to Cardiac Output:
CO = SV × Heart Rate
So if SV = 70 mL and HR = 72 bpm → CO = ~5 L/min (normal resting output).
In pregnancy: SV increases by ~30%, peaking at 28-31 weeks, primarily driven by increased preload from expanded plasma volume.
Physiological changes in pregnancy
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data across all organ systems. Here is the complete answer:
Physiological Changes in Pregnancy - All Systems
Pregnancy induces widespread adaptive changes in virtually every organ system, beginning as early as 5-6 weeks of gestation and driven primarily by progesterone, estrogen, relaxin, and human placental lactogen (hPL).
Master Summary Table
| System | Parameter | Change |
|---|---|---|
| Neurological | MAC (volatile anaesthetics) | -40% |
| Respiratory | O₂ consumption | +20 to 50% |
| Minute ventilation | +50% | |
| Tidal volume | +40% | |
| Respiratory rate | +15% | |
| FRC | -20% | |
| Airway resistance | -35% | |
| PaO₂ | +10% | |
| PaCO₂ | -15% (28-32 mmHg) | |
| HCO₃⁻ | -15% (compensatory) | |
| Cardiovascular | Plasma volume | +55% |
| Blood volume | +35% | |
| Cardiac output | +40% | |
| Stroke volume | +30% | |
| Heart rate | +20% | |
| Systolic BP | -5% | |
| Diastolic BP | -15% | |
| SVR | -15 to -50% | |
| PVR | -30% | |
| Hematological | Hemoglobin | -20% |
| Platelets | -10% | |
| Clotting factors | +30 to 250% | |
| Renal | GFR | +50% |
Morgan & Mikhail's Clinical Anesthesiology 7e, p. 1572
1. Neurological / CNS Changes
MAC reduction (-40%):
- MAC (minimum alveolar concentration) for ALL volatile anesthetic agents falls progressively, reaching -40% at term
- Returns to normal by day 3 after delivery
- Mechanism: progesterone (rises 20x by term) has sedating properties at pharmacological doses; β-endorphin surge during labor also contributes
Local anesthetic sensitivity:
- Enhanced sensitivity to local anesthetics - neural blockade occurs at reduced concentrations (up to 30% less)
- Termed MLAC (minimum local analgesic concentration) in obstetric anesthesia
- Mechanisms:
- Hormonally mediated increased nerve sensitivity
- IVC compression by gravid uterus → engorged epidural venous plexus → decreased CSF volume + decreased epidural space volume → enhanced cephalad spread of local anesthetic
Epidural space changes:
- Epidural veins engorged → increased epidural blood volume
- Epidural pressure becomes positive (normally negative) in parturients
- Increased risk of unintentional intravascular injection during epidural placement
- Decreased potential volume of epidural space
2. Respiratory Changes
Volumes and ventilation:
| Parameter | Change | Direction |
|---|---|---|
| Minute ventilation | +50% | ↑ |
| Tidal volume | +40% | ↑ (primary driver of ↑MV) |
| Respiratory rate | +15% | ↑ slight |
| Inspiratory reserve volume | ↑ | ↑ |
| FRC | -20% | ↓ |
| Expiratory reserve volume | ↓ | ↓ (major contributor to ↓FRC) |
| Vital capacity | Minimally affected | ~ |
| Closing capacity | Minimally affected | ~ |
| Physiological dead space | ↓ | ↓ |
| Airway resistance | -35% | ↓ (progesterone-mediated bronchodilation) |
Blood gases:
- PaCO₂: falls to 28-32 mmHg (normal: 40 mmHg) - respiratory alkalosis
- Compensated by renal excretion of HCO₃⁻ (falls to ~18-22 mEq/L) → mild compensated respiratory alkalosis
- PaO₂: slightly elevated (+10%) from hyperventilation
- 2,3-DPG increases → P50 rises from 27 to 30 mmHg → rightward shift of O₂-dissociation curve → enhanced O₂ delivery to fetal tissues
Mechanical changes:
- Third trimester: uterus elevates the diaphragm
- Compensated by increased anteroposterior diameter of chest
- Diaphragmatic motion is NOT restricted
- Pulmonary vasodilation prevents pulmonary pressures from rising
Airway:
- Mucosal engorgement of upper airway → friable, edematous mucosa
- Predisposes to trauma, bleeding, and obstruction during laryngoscopy
- Smaller endotracheal tube (6-6.5 mm) required
- Risk of difficult/failed intubation is higher
Key clinical implication:
- Decreased FRC + increased O₂ consumption = rapid desaturation during apnea
- Preoxygenation before GA induction is mandatory
- Closing volume may exceed FRC in supine position at term → atelectasis and hypoxemia
3. Cardiovascular Changes
(Covered in detail previously - summary here)
Volume:
- Plasma volume +55%, RBC mass +45% → dilutional anemia (physiological)
- Blood volume +35% (~1000-1500 mL extra) at term; total ~90 mL/kg
- Hemoglobin usually stays >11 g/dL
Hemodynamics:
- CO +40% at term (begins from 5 weeks; peaks 28-34 weeks)
- 1st/2nd trimester: ↑stroke volume (+30%)
- 3rd trimester: ↑heart rate (+20%, ~10-15 bpm) becomes the primary driver
- SVR and PVR fall (prostacyclin, NO, progesterone)
- BP: systolic -5%, diastolic -15%; nadir in 2nd trimester, rises back in 3rd
- CVP, PAP, PCWP remain unchanged
Structural:
- All 4 cardiac chambers dilate + myocardial hypertrophy
- Heart displaced upward-left by elevated diaphragm
- S3 and soft ejection systolic murmur are normal findings
Labor/delivery surge:
- CO rises a further 60-80% immediately postpartum
Aortocaval compression (from week 20):
- Gravid uterus compresses IVC in supine → ↓ venous return → ↓CO
- 5% develop frank supine hypotension syndrome
- Management: left lateral tilt >15°
4. Renal Changes
| Parameter | Change |
|---|---|
| Renal plasma flow | +75% |
| GFR | +40-50% |
| Serum creatinine | ↓ (to as low as 0.5 mg/dL) |
| BUN | ↓ (to as low as 9 mg/dL) |
| Plasma osmolality | ↓ by 8-10 mOsm/kg |
Tubular changes:
- Decreased renal tubular threshold for glucose and amino acids
- Glycosuria (1-10 g/day) is common and does NOT indicate diabetes
- Mild proteinuria (<300 mg/day) is normal (>300 mg/day = pathological - suspect preeclampsia)
Clinical implication: Normal serum creatinine in pregnancy is ~0.5 mg/dL. A value of 1.0 mg/dL (normal in non-pregnant) may represent significant renal impairment in a pregnant patient.
5. Gastrointestinal Changes
| Feature | Change | Clinical Significance |
|---|---|---|
| Gastric motility | ↓ (reduced) | Delayed gastric emptying |
| Lower oesophageal sphincter (LOS) | ↓ tone (progesterone effect) | Gastroesophageal reflux |
| Stomach position | Displaced upward and anteriorly by uterus | LOS incompetence |
| Gastric acidity | Unchanged | - |
| Gastric volume | Unchanged | - |
Key risk: Aspiration
- Combination of reduced LOS tone + delayed gastric emptying + stomach displacement = high risk of regurgitation and pulmonary aspiration (Mendelson's syndrome)
- This is why:
- Antacid prophylaxis (sodium citrate/H₂ antagonist/PPI) is given before GA
- RSI (rapid sequence induction) is mandatory for GA in pregnancy
- Opioids and anticholinergics worsen LOS incompetence and delay gastric emptying
6. Hepatic Changes
| Parameter | Change |
|---|---|
| Hepatic blood flow | Unchanged |
| Serum transaminases (AST/ALT) | Minor elevation in 3rd trimester |
| Alkaline phosphatase (ALP) | ↑ (from placental secretion - NOT liver disease) |
| Serum albumin | ↓ mild (dilutional, expanded plasma volume) |
| Colloid oncotic pressure | ↓ reduced |
| Pseudocholinesterase (plasma ChE) | -25 to 30% at term |
| Fibrinogen | ↑ (see hematological section) |
Pseudocholinesterase reduction:
- Activity falls 25-30% at term; doesn't normalise until 6 weeks postpartum
- Rarely prolongs suxamethonium (succinylcholine) effect significantly in normal cases
- Metabolism of ester local anesthetics (chloroprocaine, procaine) is NOT appreciably altered
Gallbladder:
- Progesterone inhibits cholecystokinin release → incomplete gallbladder emptying
- Combined with altered bile acid composition → predisposition to cholesterol gallstone formation
7. Hematological Changes
Red cell line:
- Plasma volume +55% > RBC mass +45% → physiological dilutional anemia
- Hb typically >11 g/dL
- Iron and folate requirements increase due to fetal utilization → iron-deficiency and folate-deficiency anemia if supplements not taken
White cells:
- Leukocytosis up to 21,000/μL in third trimester (especially during labor) - this is normal
Platelets:
- -10% decrease in platelet count (gestational thrombocytopenia - usually >100,000/μL)
Coagulation - HYPERCOAGULABLE STATE:
| Factor | Change |
|---|---|
| Fibrinogen | ↑ markedly (+200-300 mg/dL above baseline) |
| Factor VII | ↑ |
| Factor VIII | ↑ |
| Factor IX | ↑ |
| Factor X | ↑ |
| Factor XII | ↑ |
| Factor XI | ↓ (only factor that decreases) |
| Protein S | ↓ (acquired resistance to anticoagulation) |
| PAI-1 and PAI-2 | ↑ (reduced fibrinolysis) |
- Overall: procoagulant shift = protective against hemorrhage at delivery
- Risk: predisposition to DVT, pulmonary embolism (3-5x increased risk vs non-pregnant)
- Late 3rd trimester: accelerated fibrinolysis
8. Metabolic Changes
Carbohydrate metabolism:
- Diabetogenic state - insulin resistance increases progressively
- Insulin levels rise throughout pregnancy
- Human placental lactogen (hPL) is the key anti-insulin hormone
- Altered glucose metabolism favors fetal glucose supply
- Blood glucose and amino acid levels are lower in mother (preferential transfer to fetus)
- Free fatty acids, ketones, and triglycerides are higher (maternal fat stores mobilized)
- This resembles a "starvation-like" state in the mother, while the fetus is well nourished
Thyroid:
- Basal metabolic rate increases
- Total T3/T4 elevated (due to increased thyroxine-binding globulin from estrogen)
- Free T3/T4 remain normal
- Mild goitre may develop from iodine demand
Weight gain:
- Average: 11-13 kg total
- Fetus ~3.5 kg
- Placenta ~0.7 kg
- Amniotic fluid ~0.8 kg
- Uterus ~1 kg
- Breasts ~0.4 kg
- Blood volume ~1.5 kg
- Extracellular fluid ~1.5 kg
- Fat stores ~2-3 kg
9. Summary: Key Anesthetic Implications
| Change | Implication |
|---|---|
| MAC -40% | ↓ volatile agent dose required |
| ↑ airway edema, engorgement | Smaller ETT (6-6.5 mm), gentle laryngoscopy |
| ↓ FRC + ↑ O₂ consumption | Mandatory preoxygenation before GA |
| Local anesthetic sensitivity ↑ | Reduce epidural/spinal doses by ~30% |
| Engorged epidural veins | Risk of intravascular injection; positive epidural pressure |
| Aspiration risk | RSI mandatory; antacid prophylaxis |
| ↓ Pseudocholinesterase | Monitor suxamethonium duration |
| Hypercoagulable | DVT prophylaxis; epidural catheter removal timing |
| Aortocaval compression | Left lateral tilt at all times from week 20 |
| Dilutional anemia | Hb <11 g/dL is pathological; >11 is physiological |
Source: Morgan & Mikhail's Clinical Anesthesiology 7e, pp. 1572-1578
Create a single pdf of the all the answers provided above
Reading File
Running Command
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && echo "workspace ready"
Writing File
~/pregnancy_notes.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.pdfbase import pdfmetrics
from reportlab.pdfbase.ttfonts import TTFont
OUTPUT = "/tmp/workspace/Pregnancy_Physiology_Notes.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2.5*cm, bottomMargin=2.5*cm,
title="Physiological Changes in Pregnancy - Complete Notes",
author="Orris Medical AI"
)
styles = getSampleStyleSheet()
# Custom styles
H1 = ParagraphStyle('H1', parent=styles['Heading1'],
fontSize=18, textColor=colors.HexColor('#1a3a5c'),
spaceAfter=10, spaceBefore=20, leading=22, fontName='Helvetica-Bold')
H2 = ParagraphStyle('H2', parent=styles['Heading2'],
fontSize=14, textColor=colors.HexColor('#2e6da4'),
spaceAfter=6, spaceBefore=14, leading=18, fontName='Helvetica-Bold')
H3 = ParagraphStyle('H3', parent=styles['Heading3'],
fontSize=12, textColor=colors.HexColor('#1a5276'),
spaceAfter=4, spaceBefore=10, leading=15, fontName='Helvetica-Bold')
H4 = ParagraphStyle('H4', parent=styles['Heading4'],
fontSize=11, textColor=colors.HexColor('#154360'),
spaceAfter=3, spaceBefore=8, leading=14, fontName='Helvetica-BoldOblique')
BODY = ParagraphStyle('Body', parent=styles['Normal'],
fontSize=10, leading=14, spaceAfter=5, fontName='Helvetica',
textColor=colors.HexColor('#2c2c2c'))
BULLET = ParagraphStyle('Bullet', parent=BODY,
leftIndent=14, bulletIndent=0, spaceAfter=3,
bulletFontName='Helvetica')
NOTE = ParagraphStyle('Note', parent=BODY,
fontSize=9, textColor=colors.HexColor('#555555'),
leftIndent=10, italic=True, fontName='Helvetica-Oblique')
SOURCE = ParagraphStyle('Source', parent=BODY,
fontSize=8.5, textColor=colors.HexColor('#666666'),
fontName='Helvetica-Oblique', spaceAfter=8)
COVER_TITLE = ParagraphStyle('CoverTitle',
fontSize=26, textColor=colors.HexColor('#1a3a5c'),
alignment=TA_CENTER, fontName='Helvetica-Bold', leading=32, spaceAfter=10)
COVER_SUB = ParagraphStyle('CoverSub',
fontSize=13, textColor=colors.HexColor('#2e6da4'),
alignment=TA_CENTER, fontName='Helvetica', leading=18, spaceAfter=6)
COVER_NOTE = ParagraphStyle('CoverNote',
fontSize=10, textColor=colors.HexColor('#555555'),
alignment=TA_CENTER, fontName='Helvetica-Oblique', leading=14)
# Table style helper
def make_table_style(header_color='#2e6da4'):
return TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor(header_color)),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 9),
('ALIGN', (0,0), (-1,-1), 'LEFT'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('FONTNAME', (0,1), (-1,-1), 'Helvetica'),
('FONTSIZE', (0,1), (-1,-1), 9),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.HexColor('#f0f4f8'), colors.white]),
('GRID', (0,0), (-1,-1), 0.4, colors.HexColor('#b0c4d8')),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
])
def hr():
return HRFlowable(width="100%", thickness=0.8, color=colors.HexColor('#2e6da4'), spaceAfter=8, spaceBefore=4)
def b(text):
return f"<b>{text}</b>"
def source(text):
return Paragraph(f"<i>Source: {text}</i>", SOURCE)
story = []
# ─────────────────── COVER PAGE ───────────────────
story.append(Spacer(1, 3*cm))
story.append(Paragraph("Physiological Changes in Pregnancy", COVER_TITLE))
story.append(Paragraph("Cardiovascular System, Heart Block & Anesthetic Management", COVER_SUB))
story.append(Spacer(1, 0.5*cm))
story.append(HRFlowable(width="60%", thickness=2, color=colors.HexColor('#2e6da4'), hAlign='CENTER'))
story.append(Spacer(1, 0.5*cm))
story.append(Paragraph("Complete Clinical Notes", COVER_SUB))
story.append(Spacer(1, 3*cm))
toc_data = [
["Topic", "Page"],
["1. CVS Physiological Changes in Pregnancy", "2"],
["2. Heart Block in Pregnancy & Anesthetic Management", "5"],
["3. Types of Heart Block (Classification)", "8"],
["4. Anesthetic Management of Heart Block - Deep Dive", "11"],
["5. Stroke Volume - Definition", "14"],
["6. Physiological Changes in Pregnancy - All Systems", "15"],
]
toc_table = Table(toc_data, colWidths=[13*cm, 2*cm])
toc_table.setStyle(make_table_style('#1a3a5c'))
story.append(toc_table)
story.append(Spacer(1, 1*cm))
story.append(Paragraph("Sources: Braunwald's Heart Disease | Fuster & Hurst's The Heart 15e | Morgan & Mikhail's Clinical Anesthesiology 7e | Harrison's Principles of Internal Medicine 22e | Miller's Anesthesia 10e | Frameworks for Internal Medicine | Creasy & Resnik's Maternal-Fetal Medicine", COVER_NOTE))
story.append(PageBreak())
# ─────────────────── TOPIC 1: CVS CHANGES ───────────────────
story.append(Paragraph("1. CVS Physiological Changes in Pregnancy", H1))
story.append(hr())
story.append(Paragraph("Pregnancy imposes dramatic, well-coordinated cardiovascular adaptations beginning as early as 5-6 weeks of gestation. Driven by hormonal changes (progesterone, estrogen, relaxin), placental vasodilation, and increased metabolic demand.", BODY))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph("1.1 Blood Volume", H2))
bv_data = [
["Parameter", "Change"],
["Total blood volume", "+35% (~1000-1500 mL at term; 90 mL/kg)"],
["Plasma volume", "+40-55% (peaks at 24-28 weeks)"],
["Red blood cell mass", "+45%"],
["Result", "Physiological dilutional anaemia of pregnancy"],
["Haemoglobin", "Usually remains >11 g/dL"],
]
t = Table(bv_data, colWidths=[7*cm, 8*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph("The disproportionate rise in plasma volume over RBC mass produces physiological dilutional anaemia. Reduced blood viscosity is a beneficial adaptation.", BODY))
story.append(Paragraph("1.2 Cardiac Output (CO)", H2))
story.append(Paragraph("The most important CVS change. CO rises 30-50% above pre-pregnancy baseline.", BODY))
co_data = [
["Parameter", "Change"],
["Cardiac output", "+40% at term"],
["Onset", "From 5 weeks after LMP"],
["Peak", "28-34 weeks gestation"],
["Stroke volume", "+30% (peaks 28-31 weeks)"],
["Heart rate", "+20% (~10-15 bpm above baseline)"],
["Twin pregnancy", "Additional +10-15% CO"],
]
t = Table(co_data, colWidths=[7*cm, 8*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph("<b>Mechanism by trimester:</b> 1st & 2nd trimester: rise primarily due to increased stroke volume (+30-40%). 3rd trimester: rise primarily due to increased heart rate (+10-15 bpm). CO begins to decline in late 3rd trimester but does NOT return to pre-pregnancy values until 2-4 weeks postpartum.", BODY))
story.append(Paragraph("1.3 Blood Pressure", H2))
bp_data = [
["Parameter", "Change"],
["Systolic BP", "-5% (5-10 mmHg below baseline)"],
["Diastolic BP", "-15% (more pronounced fall)"],
["Onset", "6-8 weeks; nadir in 2nd trimester"],
["3rd trimester", "Gradually rises back to baseline"],
]
t = Table(bp_data, colWidths=[7*cm, 8*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("Driven by progesterone-mediated vasodilation, prostacyclin, and nitric oxide.", BODY))
story.append(Paragraph("1.4 Vascular Resistance", H2))
vr_data = [
["Parameter", "Change"],
["SVR (Systemic Vascular Resistance)", "-15 to -50%"],
["PVR (Pulmonary Vascular Resistance)", "-30%"],
["CVP / PAP / PCWP", "Unchanged"],
]
t = Table(vr_data, colWidths=[7*cm, 8*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("1.5 Cardiac Structure & Examination", H2))
for item in [
"All four cardiac chambers dilate; myocardial hypertrophy on echo",
"Diaphragm elevation → heart shifts left and upward → apparent cardiomegaly on CXR",
"Left axis deviation and T wave changes on ECG",
"Normal findings: Grade I-II ejection systolic murmur (flow murmur), exaggerated S1 splitting, audible S3, collapsing arterial pulses, laterally displaced apex",
"Small pericardial effusion in some (asymptomatic, normal)",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("1.6 Hemodynamics During Labour & Delivery", H2))
labour_data = [
["Stage", "CO Increase vs. Prelabour"],
["Early labour", "+15 to 25%"],
["Active labour", "+50%"],
["Immediately postpartum", "+60 to 80%"],
]
t = Table(labour_data, colWidths=[7*cm, 8*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("Mechanisms: catecholamine surge, autotransfusion from uterine contractions (300-500 mL per contraction), relief of IVC compression, pain.", BODY))
story.append(Paragraph("1.7 Aortocaval Compression (from week 20)", H2))
for item in [
"Gravid uterus compresses IVC in supine position → ↓ venous return → ↓ CO",
"~5% of women at term develop supine hypotension syndrome (pallor, sweating, nausea, hypotension)",
"Aorta also compressed → ↓ uteroplacental perfusion",
"Management: Left lateral tilt >15° (wedge under right hip)",
"Chronic partial IVC obstruction → lower limb oedema, DVT risk, dilated epidural veins",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("1.8 Postpartum Resolution", H2))
for item in [
"Heart rate falls ~14% within 48 hours of delivery",
"CO normalises by 2 weeks postpartum",
"Complete haemodynamic resolution may take up to 6 months",
"First week postpartum: fluid mobilisation can precipitate heart failure in susceptible women",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(source("Braunwald's Heart Disease p.1062; Fuster & Hurst's The Heart 15e p.2209; Morgan & Mikhail's Clinical Anesthesiology 7e p.1572-1576"))
story.append(PageBreak())
# ─────────────────── TOPIC 2: HEART BLOCK IN PREGNANCY ───────────────────
story.append(Paragraph("2. Heart Block in Pregnancy & Anesthetic Management", H1))
story.append(hr())
story.append(Paragraph("2.1 Overview", H2))
story.append(Paragraph("Heart block in pregnancy falls into two categories:", BODY))
story.append(Paragraph("• <b>Maternal Heart Block</b> - AV conduction disease in the pregnant woman", BULLET))
story.append(Paragraph("• <b>Congenital Heart Block (Fetal/Neonatal)</b> - passively acquired by fetus from maternal anti-Ro/SSA antibodies", BULLET))
story.append(Paragraph("2.2 Why Pregnancy Is Challenging in Heart Block", H2))
story.append(Paragraph("Pregnancy requires a progressive rise in CO of 30-50%. In the 3rd trimester, CO augmentation depends predominantly on heart rate increase. In complete heart block, ventricular rate is fixed (35-55 bpm). The patient CANNOT augment heart rate in response to:", BODY))
for item in [
"Increased metabolic demand of pregnancy",
"Labour contractions (catecholamine surge)",
"Haemorrhage",
"Anaesthetic-induced vasodilation",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("2.3 Management by Degree", H2))
mgmt_data = [
["Degree", "Features", "Management in Pregnancy"],
["1st degree", "PR >200 ms, all beats conducted", "Monitor for progression; no intervention"],
["2nd degree Mobitz I", "Progressive PR lengthening, dropped beats", "Usually benign; monitor"],
["2nd degree Mobitz II", "Fixed PR, sudden dropped beats, infranodal", "High risk - permanent pacemaker; TCP on standby"],
["3rd degree (CHB)", "Complete AV dissociation, escape rhythm", "See detailed management below"],
]
t = Table(mgmt_data, colWidths=[3*cm, 5.5*cm, 6.5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("2.4 Complete Heart Block - Specific Management", H2))
chb_data = [
["Scenario", "Management"],
["Asymptomatic, pre-existing CHB", "Expectant management; NO prophylactic temporary pacing needed even with Valsalva"],
["Asymptomatic → develops symptoms during pregnancy", "Permanent pacemaker required"],
["Symptomatic at any point", "Permanent pacemaker"],
["Emergency", "Transcutaneous pacing until transvenous pacing possible"],
["Pacemaker implantation during pregnancy", "Echocardiographic guidance to minimise fetal radiation"],
]
t = Table(chb_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("Note: Whether pacemaker settings should be increased during pregnancy to augment CO remains under investigation. Prophylactic pacing of asymptomatic women provides no benefit.", NOTE))
story.append(Paragraph("2.5 Congenital Heart Block (Neonatal Lupus)", H2))
story.append(Paragraph("Mothers with anti-Ro/SSA and/or anti-La/SSB antibodies (SLE, Sjögren's) transfer these IgG antibodies across the placenta → inflammation and fibrosis of fetal AV node.", BODY))
cchb_data = [
["Scenario", "Risk of CCHB"],
["Anti-Ro/SSA positive, no prior history", "~2%"],
["Prior child with complete heart block", "15-20% recurrence"],
]
t = Table(cchb_data, colWidths=[9*cm, 6*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph("<b>Prevention:</b> Hydroxychloroquine (HCQ) - PATCH study showed >50% reduction in CCHB recurrence. Fetal echo screening 16-26 weeks. Most neonates with CCHB require permanent pacemaker after birth.", BODY))
story.append(source("Fuster & Hurst's The Heart 15e p.2221; Creasy & Resnik's Maternal-Fetal Medicine p.2468-2470"))
story.append(PageBreak())
# ─────────────────── TOPIC 3: TYPES OF HEART BLOCK ───────────────────
story.append(Paragraph("3. Types of Heart Block - Full Classification", H1))
story.append(hr())
story.append(Paragraph("3.1 Anatomy of the AV Conduction System", H2))
for item in [
"AV nodal artery: from RCA in 80-90%, left circumflex in 10%, both in 10%",
"Bundle of His and bundle branches: dual supply from LAD septal perforators (LBB, proximal RBB) and posterior descending artery",
"AV node: richly innervated by sympathetic AND parasympathetic nerves",
"Bundle of His and distal conduction system: NOT influenced by autonomic tone → why atropine fails in Mobitz II / CHB",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("3.2 First-Degree AV Block", H2))
fd_data = [
["Feature", "Detail"],
["Definition", "PR interval >200 ms; ALL beats conducted; no dropped beats"],
["Site of delay", "Usually AV node (can be atria, His bundle, or Purkinje)"],
["ECG", "Prolonged fixed PR; 1:1 P:QRS ratio"],
["Symptoms", "Usually none; severe (PR >300 ms): dyspnoea, light-headedness on exertion"],
["Causes", "Beta-blockers, digoxin, CCBs, inferior MI, Lyme disease, myocarditis, amyloidosis, athletes (vagal)"],
["Prognosis", "Benign; slight increased risk of AF and conduction progression"],
["Treatment", "Usually none; address reversible causes"],
["In pregnancy", "Well tolerated; monitor for progression"],
]
t = Table(fd_data, colWidths=[4*cm, 11*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("3.3 Second-Degree AV Block - Mobitz I (Wenckebach)", H2))
m1_data = [
["Feature", "Detail"],
["ECG pattern", "Progressive PR prolongation before a suddenly dropped QRS; PR resets after dropped beat; RR shortens before drop"],
["Site of block", "AV node (nodal)"],
["Associated MI", "Right coronary artery territory - inferior MI (ST elevation II, III, aVF)"],
["Symptoms", "Usually asymptomatic; mild palpitations/light-headedness"],
["Prognosis", "Haemodynamically stable; does NOT require pacing if asymptomatic"],
["Treatment", "Address reversible causes; pacing rarely needed"],
["In pregnancy", "Monitor; generally does not require intervention"],
]
t = Table(m1_data, colWidths=[4*cm, 11*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("3.4 Second-Degree AV Block - Mobitz II", H2))
m2_data = [
["Feature", "Detail"],
["ECG pattern", "Fixed PR interval; sudden unexpected dropped QRS with NO preceding PR prolongation; QRS often WIDE"],
["Site of block", "Below AV node - His-Purkinje system or bundle branches (infranodal)"],
["Associated MI", "LAD territory - anterior MI (ST elevation V1-V4)"],
["Symptoms", "Frequently symptomatic: dyspnoea, syncope, presyncope"],
["Prognosis", "Serious - high rate of progression to CHB; risk of sudden death"],
["Treatment", "Permanent pacemaker virtually always required (even if asymptomatic)"],
["In pregnancy", "High risk - permanent pacemaker; TCP standby during labour"],
]
t = Table(m2_data, colWidths=[4*cm, 11*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("3.5 Special Case: 2:1 AV Block", H2))
story.append(Paragraph("Alternating conducted and non-conducted beats. Cannot distinguish Mobitz I vs II on ECG alone.", BODY))
twone_data = [
["Feature", "Suggests Nodal (Mobitz I)", "Suggests Infranodal (Mobitz II)"],
["QRS width", "Narrow", "Wide"],
["PR interval", ">160 ms", "<160 ms"],
["Response to atropine", "Improves", "No improvement"],
["Response to exercise", "Conduction improves", "Conduction worsens"],
["Prognosis/treatment", "Often benign", "Permanent pacemaker required"],
]
t = Table(twone_data, colWidths=[4*cm, 5.5*cm, 5.5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("3.6 Third-Degree (Complete) Heart Block", H2))
chb_data2 = [
["Feature", "Detail"],
["Definition", "Complete AV dissociation - NO atrial impulse reaches the ventricles"],
["ECG", "P waves at regular atrial rate; QRS complexes at slower escape rate; NO fixed P-QRS relationship"],
["Escape rhythm - narrow QRS", "Block in AV node/proximal His; 40-60 bpm junctional; more stable and reliable"],
["Escape rhythm - wide QRS", "Block in distal His/bundle branches; 20-40 bpm idioventricular; slow, unreliable, risk of asystole"],
["Symptoms", "Stokes-Adams attacks (syncope), severe dyspnoea, heart failure, presyncope; ventricular rate 35-55 bpm"],
["Causes", "Congenital (most common in young women), fibrosis (Lenègre/Lev), inferior/anterior MI, post-cardiac surgery, SLE/anti-Ro, Lyme disease, sarcoidosis, amyloidosis, drug toxicity (digoxin, beta-blockers)"],
["Treatment", "Permanent pacemaker in virtually all symptomatic patients; echoguided in pregnancy"],
]
t = Table(chb_data2, colWidths=[4.5*cm, 10.5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(source("Harrison's Principles of Internal Medicine 22e p.1969; Frameworks for Internal Medicine p.47-49; Miller's Anesthesia 10e p.12222"))
story.append(PageBreak())
# ─────────────────── TOPIC 4: ANAESTHETIC MANAGEMENT DEEP DIVE ───────────────────
story.append(Paragraph("4. Anesthetic Management of Heart Block in Pregnancy - Deep Dive", H1))
story.append(hr())
story.append(Paragraph("4.1 Core Physiological Problem", H2))
story.append(Paragraph("In complete heart block, ventricular rate is fixed by the escape pacemaker. No compensatory tachycardia is possible. Any fall in BP or increase in demand cannot be corrected by reflex tachycardia. The only compensatory mechanism is increased stroke volume (preload-dependent) - and this too is limited.", BODY))
story.append(Paragraph("4.2 Pre-Anaesthetic Preparation", H2))
pre_data = [
["Assessment", "Detail"],
["ECG + Holter monitor", "Document escape rate range (typically 37-53 bpm in CHB)"],
["Echocardiography", "LV/RV function, wall motion, structural disease"],
["Electrolytes", "K⁺ >4.0 mEq/L, Mg²⁺ >2.0 mg/dL (normalise before any procedure)"],
["Blood group & cross-match", "Haemorrhage tolerated poorly with fixed heart rate"],
["Pacemaker check", "Verify settings and function if device in situ"],
["MDT planning", "OB + Cardiology + EP + Anaesthesia + Neonatology"],
]
t = Table(pre_data, colWidths=[5*cm, 10*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("4.3 Pacing Strategy", H2))
pac_data = [
["Patient Status", "Pacing Approach"],
["Asymptomatic, haemodynamically stable", "Transcutaneous pads on standby; NO prophylactic pacing needed"],
["Symptomatic (syncope, dyspnoea, haemodynamic compromise)", "Permanent pacemaker before or during pregnancy (echoguided)"],
["Emergency labour/LSCS without pacemaker", "Transcutaneous pacing immediately; convert to transvenous ASAP"],
["Pacemaker in situ", "Check settings; consider rate programming adjustment"],
]
t = Table(pac_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("Why atropine is INEFFECTIVE in Mobitz II and CHB: Atropine reverses vagal effects on the AV node only. In infranodal block (Mobitz II, CHB), there is NO vagal innervation below the AV node. Atropine cannot accelerate an idioventricular escape rhythm and may worsen the situation.", NOTE))
story.append(Paragraph("4.4 Drug Management of Bradycardia", H2))
drug_data = [
["Drug", "Dose", "Mechanism", "Role in Heart Block"],
["Atropine", "1 mg IV q3-5 min; max 3 mg\n(avoid <0.5 mg)", "Antimuscarinic - blocks vagal tone on AV node", "Only for NODAL block (Mobitz I, sinus brady). NOT effective for Mobitz II or CHB"],
["Dopamine", "2-20 mcg/kg/min IV", "Alpha + beta adrenergic; rate/inotropy at low dose, vasoconstriction >10 mcg/kg/min", "2nd line for bradycardia unresponsive to atropine"],
["Epinephrine", "2-10 mcg/min IV infusion", "Alpha + beta", "Severe bradycardia/cardiac arrest"],
["Isoproterenol", "2-10 mcg/min IV infusion", "Pure beta-1 and beta-2 agonist", "Accelerates ventricular escape rhythm; useful temporising in CHB while awaiting pacing; causes vasodilation"],
["Phenylephrine", "50-100 mcg IV boluses", "Pure alpha-1", "Treats hypotension WITHOUT increasing HR - 1st choice for neuraxial-induced hypotension"],
["Ephedrine", "5-10 mg IV", "Alpha + beta", "Treats hypotension + raises HR; use if bradycardia co-exists"],
]
t = Table(drug_data, colWidths=[2.8*cm, 3*cm, 4*cm, 5.2*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("4.5 Anaesthetic Technique", H2))
story.append(Paragraph("<b>For Labour Analgesia - Epidural (strongly preferred):</b>", H4))
for item in [
"Slow, titrated sympathectomy avoids sudden haemodynamic swings",
"0.2% ropivacaine at 10 mL/hr (or equivalent low-dose bupivacaine)",
"Blunts catecholamine surges of labour pain",
"Epidural catheter can be used for subsequent caesarean if needed",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("<b>For Elective LSCS - Epidural top-up (preferred):</b>", H4))
for item in [
"Incremental boluses: e.g., 0.5% bupivacaine + 2% lidocaine in 5 mL increments to T4 level",
"Prophylactic atropine 0.2 mg IV before block establishment",
"Arterial line (radial artery, 20G) for beat-to-beat monitoring",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("<b>For Emergency LSCS - Spinal (acceptable):</b>", H4))
for item in [
"Low-dose hyperbaric bupivacaine/levobupivacaine",
"CO-LOADING preferred over pre-loading (pre-loading risks fluid overload in fixed-rate heart)",
"Phenylephrine infusion to treat sympathectomy-induced hypotension",
"Transcutaneous pacing pads applied before spinal",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("<b>General Anaesthesia (last resort only):</b>", H4))
for item in [
"RSI mandatory (aspiration risk) + antacid prophylaxis",
"Laryngoscopy can trigger vagal bradycardia - have vasopressors drawn up",
"Volatile agents depress escape rhythm - use lowest effective concentration",
"Avoid hypoxia, hypercarbia, acidosis - all worsen conduction and impair pacing capture",
"Transcutaneous/transvenous pacing immediately available",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("4.6 Intraoperative Monitoring", H2))
mon_data = [
["Monitor", "Rationale"],
["Continuous ECG", "Detect rhythm changes, pacing capture failure"],
["Invasive arterial line (radial 20G)", "Beat-to-beat BP; HR unreliable from pulse in CHB"],
["2x Large-bore IV access (min 16G)", "Rapid drug administration and volume resuscitation"],
["Transcutaneous pacing pads", "Mandatory in all CHB patients - immediate pacing capability"],
["SpO₂", "Oxygenation monitoring"],
["Foley catheter", "Fluid balance"],
]
t = Table(mon_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("4.7 Labour & Postpartum Management", H2))
for item in [
"Vaginal delivery is feasible in haemodynamically stable, asymptomatic patients",
"Shorten second stage with instrumental delivery (forceps/vacuum) - avoid prolonged Valsalva",
"Left lateral tilt at all times to prevent aortocaval compression",
"Continuous CTG monitoring; avoid oxytocin boluses (use slow infusion)",
"Immediate postpartum: CO rises 60-80%; fluid mobilisation days 1-7 - risk of decompensation",
"Cardiology + EP follow-up mandatory; asymptomatic patients may need pacemaker postpartum",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(source("Miller's Anesthesia 10e p.12222-12224; Fuster & Hurst's The Heart 15e p.2221; PMC11973396 (Anesthetic Considerations for Cesarean Delivery in CHB)"))
story.append(PageBreak())
# ─────────────────── TOPIC 5: STROKE VOLUME ───────────────────
story.append(Paragraph("5. Stroke Volume - Definition", H1))
story.append(hr())
story.append(Paragraph("Stroke volume (SV) is the volume of blood ejected by one ventricle per single contraction (heartbeat). Normal value is approximately 60-100 mL at rest.", BODY))
story.append(Paragraph("5.1 Formula", H2))
story.append(Paragraph("<b>SV = End-Diastolic Volume (EDV) − End-Systolic Volume (ESV)</b>", H3))
sv_data = [
["Variable", "Value", "Definition"],
["EDV (End-Diastolic Volume)", "~120-130 mL", "Volume in ventricle after filling (preload)"],
["ESV (End-Systolic Volume)", "~50-60 mL", "Volume remaining after ejection"],
["SV (Stroke Volume)", "~70 mL", "EDV minus ESV"],
["EF (Ejection Fraction)", "55-70%", "SV ÷ EDV × 100 (normal ≥55%)"],
]
t = Table(sv_data, colWidths=[5*cm, 3.5*cm, 6.5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("5.2 Cardiac Output Relationship", H2))
story.append(Paragraph("<b>CO = SV × Heart Rate</b> (e.g., 70 mL × 72 bpm = ~5 L/min)", H3))
story.append(Paragraph("5.3 Three Determinants of Stroke Volume", H2))
det_data = [
["Determinant", "Definition", "Effect on SV"],
["Preload", "Ventricular filling pressure/stretch before contraction (EDV)", "↑ Preload → ↑ SV (Frank-Starling law)"],
["Afterload", "Resistance ventricle must overcome to eject blood (SVR/wall stress)", "↑ Afterload → ↓ SV"],
["Contractility", "Intrinsic force of myocardial contraction (inotropy), independent of pre/afterload", "↑ Contractility → ↑ SV"],
]
t = Table(det_data, colWidths=[3.5*cm, 5.5*cm, 6*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("5.4 In Pregnancy", H2))
story.append(Paragraph("SV increases by ~30%, peaking at 28-31 weeks, primarily driven by increased preload from expanded plasma volume (+55%). In the 3rd trimester, heart rate becomes the dominant mechanism for further CO augmentation.", BODY))
story.append(PageBreak())
# ─────────────────── TOPIC 6: ALL SYSTEM CHANGES ───────────────────
story.append(Paragraph("6. Physiological Changes in Pregnancy - All Systems", H1))
story.append(hr())
story.append(Paragraph("6.1 Master Summary Table", H2))
master_data = [
["System", "Parameter", "Change"],
["Neurological", "MAC (volatile anaesthetics)", "-40%"],
["Respiratory", "O₂ consumption", "+20 to 50%"],
["", "Minute ventilation", "+50%"],
["", "Tidal volume", "+40%"],
["", "Respiratory rate", "+15%"],
["", "FRC", "-20%"],
["", "Airway resistance", "-35%"],
["", "PaO₂", "+10%"],
["", "PaCO₂", "-15% (28-32 mmHg)"],
["", "HCO₃⁻", "-15% (compensatory)"],
["Cardiovascular", "Plasma volume", "+55%"],
["", "Blood volume", "+35%"],
["", "Cardiac output", "+40%"],
["", "Stroke volume", "+30%"],
["", "Heart rate", "+20%"],
["", "Systolic BP", "-5%"],
["", "Diastolic BP", "-15%"],
["", "SVR", "-15 to -50%"],
["", "PVR", "-30%"],
["Hematological", "Haemoglobin", "-20%"],
["", "Platelets", "-10%"],
["", "Clotting factors", "+30 to 250%"],
["Renal", "GFR", "+50%"],
["", "Serum creatinine", "↓ to 0.5 mg/dL"],
["", "BUN", "↓ to 9 mg/dL"],
]
t = Table(master_data, colWidths=[4*cm, 6*cm, 5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("6.2 Neurological / CNS Changes", H2))
for item in [
"MAC falls -40% at term for ALL volatile agents; returns to normal by day 3 postdelivery",
"Mechanism: progesterone (rises 20× by term) is sedating; β-endorphin surge during labour",
"Enhanced sensitivity to local anaesthetics - neural blockade at reduced concentrations (up to 30% less)",
"IVC compression → engorged epidural venous plexus → ↓CSF volume, ↓epidural space volume → enhanced cephalad spread",
"Epidural pressure becomes POSITIVE (normally negative) in parturients",
"Increased risk of unintentional intravascular injection during epidural placement",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("6.3 Respiratory Changes", H2))
resp_data = [
["Parameter", "Change", "Clinical Significance"],
["Minute ventilation", "+50%", "Hyperventilation state; driven mainly by progesterone"],
["Tidal volume", "+40%", "Primary driver of increased MV"],
["FRC", "-20%", "Rapid O₂ desaturation during apnea; mandatory preoxygenation"],
["PaCO₂", "-15% (28-32 mmHg)", "Respiratory alkalosis; compensated by ↓HCO₃⁻"],
["HCO₃⁻", "-15%", "Compensatory metabolic acidosis; normal pH ~7.44"],
["PaO₂", "+10%", "Slight improvement from hyperventilation"],
["Airway resistance", "-35%", "Progesterone-mediated bronchodilation"],
["2,3-DPG", "↑", "P50 rises 27→30 mmHg; rightward O₂-dissociation curve shift → enhanced O₂ delivery to fetus"],
["Airway mucosa", "Engorged, oedematous, friable", "Risk of bleeding/trauma; use 6-6.5 mm ETT; difficult airway risk"],
]
t = Table(resp_data, colWidths=[4*cm, 4*cm, 7*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("Key: Decreased FRC + increased O₂ consumption = rapid desaturation during apnea. Preoxygenation before GA is MANDATORY.", NOTE))
story.append(Paragraph("6.4 Renal Changes", H2))
ren_data = [
["Parameter", "Change"],
["Renal plasma flow", "+75%"],
["GFR", "+40-50%"],
["Serum creatinine", "↓ to 0.5 mg/dL (normal non-pregnant value = pathological in pregnancy)"],
["BUN", "↓ to 9 mg/dL"],
["Plasma osmolality", "↓ by 8-10 mOsm/kg"],
["Glycosuria (1-10 g/day)", "Common, normal (↓ tubular threshold)"],
["Proteinuria (<300 mg/day)", "Normal (>300 mg/day = pathological - suspect preeclampsia)"],
]
t = Table(ren_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("6.5 Gastrointestinal Changes", H2))
gi_data = [
["Feature", "Change", "Clinical Significance"],
["Gastric motility", "↓ Reduced", "Delayed gastric emptying"],
["Lower oesophageal sphincter", "↓ Tone (progesterone)", "Gastro-oesophageal reflux"],
["Stomach position", "Displaced upward/anteriorly by uterus", "LOS incompetence; aspiration risk"],
["Gastric acidity", "Unchanged", "-"],
["Gastric volume", "Unchanged", "-"],
]
t = Table(gi_data, colWidths=[4*cm, 4*cm, 7*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("→ RSI mandatory for GA in pregnancy; antacid prophylaxis (sodium citrate/H₂ antagonist/PPI) essential", NOTE))
story.append(Paragraph("6.6 Hepatic Changes", H2))
hep_data = [
["Parameter", "Change"],
["Hepatic blood flow", "Unchanged"],
["ALT/AST", "Minor elevation in 3rd trimester"],
["Alkaline phosphatase", "↑ (from placental secretion - NOT liver disease)"],
["Serum albumin", "↓ mild (dilutional)"],
["Colloid oncotic pressure", "↓ Reduced"],
["Pseudocholinesterase activity", "-25 to 30% at term; normalises by 6 weeks postpartum"],
["Gallbladder", "Incomplete emptying (progesterone inhibits CCK); risk of cholesterol gallstones"],
]
t = Table(hep_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("6.7 Hematological Changes", H2))
haem_data = [
["Parameter", "Change"],
["RBC mass", "+45%"],
["Plasma volume", "+55%"],
["Result", "Physiological dilutional anaemia (Hb >11 g/dL = normal)"],
["WBC (leukocytes)", "↑ Up to 21,000/μL in 3rd trimester - NORMAL"],
["Platelets", "-10% (gestational thrombocytopenia; usually >100,000/μL)"],
["Fibrinogen", "↑ markedly (+200-300 mg/dL)"],
["Factors VII, VIII, IX, X, XII", "All ↑"],
["Factor XI", "↓ (only coagulation factor that decreases)"],
["Protein S", "↓ (acquired resistance to anticoagulation)"],
["PAI-1 and PAI-2", "↑ (reduced fibrinolysis)"],
["Overall coagulation", "HYPERCOAGULABLE STATE → DVT/PE risk ×3-5"],
]
t = Table(haem_data, colWidths=[6*cm, 9*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Paragraph("6.8 Metabolic Changes", H2))
for item in [
"Diabetogenic state: insulin resistance increases progressively; insulin levels rise throughout",
"Human placental lactogen (hPL) is the key anti-insulin hormone",
"Maternal blood glucose and amino acids: LOWER (preferential transfer to fetus)",
"Maternal free fatty acids, ketones, triglycerides: HIGHER (maternal fat stores mobilised)",
"Resembles 'starvation' in the mother while fetus is well nourished",
"Thyroid: total T3/T4 elevated (increased TBG from oestrogen); free T3/T4 remain NORMAL",
"Basal metabolic rate: increased",
]:
story.append(Paragraph(f"• {item}", BULLET))
story.append(Paragraph("6.9 Key Anaesthetic Implications Summary", H2))
anaes_imp = [
["Change", "Anaesthetic Implication"],
["MAC -40%", "↓ Volatile agent dose required"],
["↑ Airway oedema/engorgement", "Smaller ETT (6-6.5 mm); gentle laryngoscopy; higher difficult airway risk"],
["↓ FRC + ↑ O₂ consumption", "Mandatory preoxygenation before GA; rapid desaturation"],
["Local anaesthetic sensitivity ↑", "Reduce epidural/spinal doses ~30%"],
["Engorged epidural veins", "Risk of intravascular injection; positive epidural pressure"],
["Aspiration risk", "RSI mandatory; antacid prophylaxis (Na citrate + ranitidine/PPI)"],
["↓ Pseudocholinesterase -25-30%", "Monitor suxamethonium duration"],
["Hypercoagulable", "DVT prophylaxis; timing of epidural catheter removal"],
["Aortocaval compression (>20 wks)", "Left lateral tilt at ALL times; avoid supine position"],
["Physiological anaemia", "Hb <11 g/dL pathological; Hb >11 g/dL physiological"],
]
t = Table(anaes_imp, colWidths=[5.5*cm, 9.5*cm])
t.setStyle(make_table_style())
story.append(t)
story.append(Spacer(1, 0.5*cm))
story.append(source("Morgan & Mikhail's Clinical Anesthesiology 7e pp.1572-1578; Braunwald's Heart Disease p.1062; Fuster & Hurst's The Heart 15e p.2209; Harrison's Principles of Internal Medicine 22e; Miller's Anesthesia 10e"))
story.append(Spacer(1, 1*cm))
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor('#1a3a5c')))
story.append(Spacer(1, 0.3*cm))
story.append(Paragraph("Generated by Orris Medical AI | Sources: Authoritative Medical Textbooks & Peer-Reviewed Literature | For educational use only", COVER_NOTE))
# Build PDF
doc.build(story)
print("PDF created successfully:", OUTPUT)
Running Command
cd /tmp/workspace && python pregnancy_notes.py 2>&1
Running Command
ls -lh /tmp/workspace/Pregnancy_Physiology_Notes.pdf
Your PDF is ready. It is a fully formatted, colour-coded document covering all six topics from this session:
Pregnancy Physiology Notes
PDF Document · PDF
Contents of the PDF:
| # | Topic |
|---|---|
| 1 | CVS Physiological Changes in Pregnancy |
| 2 | Heart Block in Pregnancy & Anesthetic Management |
| 3 | Types of Heart Block - Full Classification |
| 4 | Anesthetic Management - Deep Dive (pacing, drugs, techniques, monitoring) |
| 5 | Stroke Volume - Definition |
| 6 | Physiological Changes in Pregnancy - All Systems |
Features: formatted tables with colour-coded headers, bullet points, section headings, cover page with table of contents, and source citations throughout.
This is a shared conversation. Sign in to Orris to start your own chat.