Sleep physiology mbbs 1st year
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from Harrison's and Adams & Victor. Let me compile a thorough MBBS 1st year-level answer.
Sleep Physiology - MBBS 1st Year
1. Introduction
Sleep is a naturally recurring, reversible state of reduced consciousness and reduced responsiveness to external stimuli. It is NOT a passive state - the brain remains highly active during sleep, just differently organized. Sleep is a basic circadian rhythm seen in all mammalian, avian, and reptilian species.
Most healthy adults require 7-9 hours per night. Sleep duration varies with age:
- Newborn: 16-20 h/day
- Child: 10-12 h/day
- Adolescent: 9-10 h/day
- Young adult: ~7-7.5 h/day
- Elderly (>70 yrs): ~6 h/day
2. How Sleep is Recorded - Polysomnography (PSG)
Sleep stages are defined by recording three parameters simultaneously:
| Parameter | What it measures |
|---|---|
| EEG (Electroencephalogram) | Brain electrical activity |
| EOG (Electrooculogram) | Eye movements |
| EMG (Electromyogram) | Muscle tone (chin + legs) |
This combined recording is called polysomnography (PSG).
3. Stages of Sleep (AASM Classification)
Sleep has two major types: NREM and REM.
NREM Sleep (Non-Rapid Eye Movement)
Divided into 3 stages (N1, N2, N3):
| Stage | Old name | EEG Pattern | Features |
|---|---|---|---|
| W (Wake) | - | Posterior alpha waves (9-11 Hz) + low-voltage fast activity | Alert, eyes open |
| N1 | Stage 1 | Diffuse theta waves; loss of alpha | Drowsy; slow roving eye movements; light sleep; easily aroused |
| N2 | Stage 2 | Sleep spindles (12-14 Hz, 0.5-2 sec bursts) + K complexes (high-amplitude sharp slow waves, central-parietal) | Light sleep; majority of total sleep |
| N3 | Stages 3 & 4 (Slow Wave Sleep) | High-voltage delta waves (0.5-2 Hz, >75 µV) | Deep sleep; hardest to arouse; sleepwalking/night terrors occur here |
REM Sleep (Rapid Eye Movement)
- EEG: Low amplitude, mixed frequency (similar to N1 / wakefulness - hence called "paradoxical sleep")
- EOG: Rapid conjugate eye movements in bursts
- EMG: Near-complete muscle atonia (active inhibition of motor neurons - protects us from acting out dreams)
- Dreaming is most vivid and consistently recalled in REM
- Brain metabolic activity approaches waking levels
Adams & Victor's Neurology: "Subjects are easily aroused from REM sleep but arousing a person during stage N3 is more difficult; full arousal may take minutes or more, during which time the subject may be slightly disoriented and confused."
4. Architecture of a Normal Night's Sleep (Hypnogram)
- Sleep onset → progresses through N1 → N2 → N3 within 45-60 min
- First REM episode occurs about 90 min after sleep onset
- NREM and REM then alternate in cycles of 60-160 min (the "ultradian cycle")
- N3 (slow-wave sleep) predominates in the first third of the night
- REM episodes get longer toward the end of the night (second half is REM-rich)
- Setting an alarm clock causes selective REM deprivation (as REM is most prominent late in sleep)
Proportions in a healthy young adult:
- N1 + N2 = 50-60%
- N3 (slow wave) = 15-25%
- REM = 20-25%
- REM in infancy = up to 50% (important for brain development)
5. Neural Control of Sleep-Wake Cycles
The Flip-Flop Switch Model
Two opposing systems keep each other in check - like an electrical flip-flop switch - ensuring rapid, stable transitions between waking and sleeping:
Ascending Arousal System (keeps us awake):
- Neurons extend from upper pons → hypothalamus → basal forebrain
- Neurotransmitters used: Norepinephrine, Dopamine, Serotonin, Histamine, Glutamate, Acetylcholine
- Orexin (Hypocretin) neurons in the lateral hypothalamus reinforce and stabilize arousal (loss of orexin neurons → Narcolepsy)
- Some basal forebrain neurons use GABA to inhibit cortical inhibitory interneurons (thereby promoting arousal)
Sleep-Promoting System (turns off wakefulness):
- Ventrolateral Preoptic Nucleus (VLPO) in the hypothalamus - key sleep-promoting site
- Preoptic area and pons neurons use GABA to inhibit the arousal system
- Lateral hypothalamic neurons containing Melanin-Concentrating Hormone (MCH) promote REM sleep
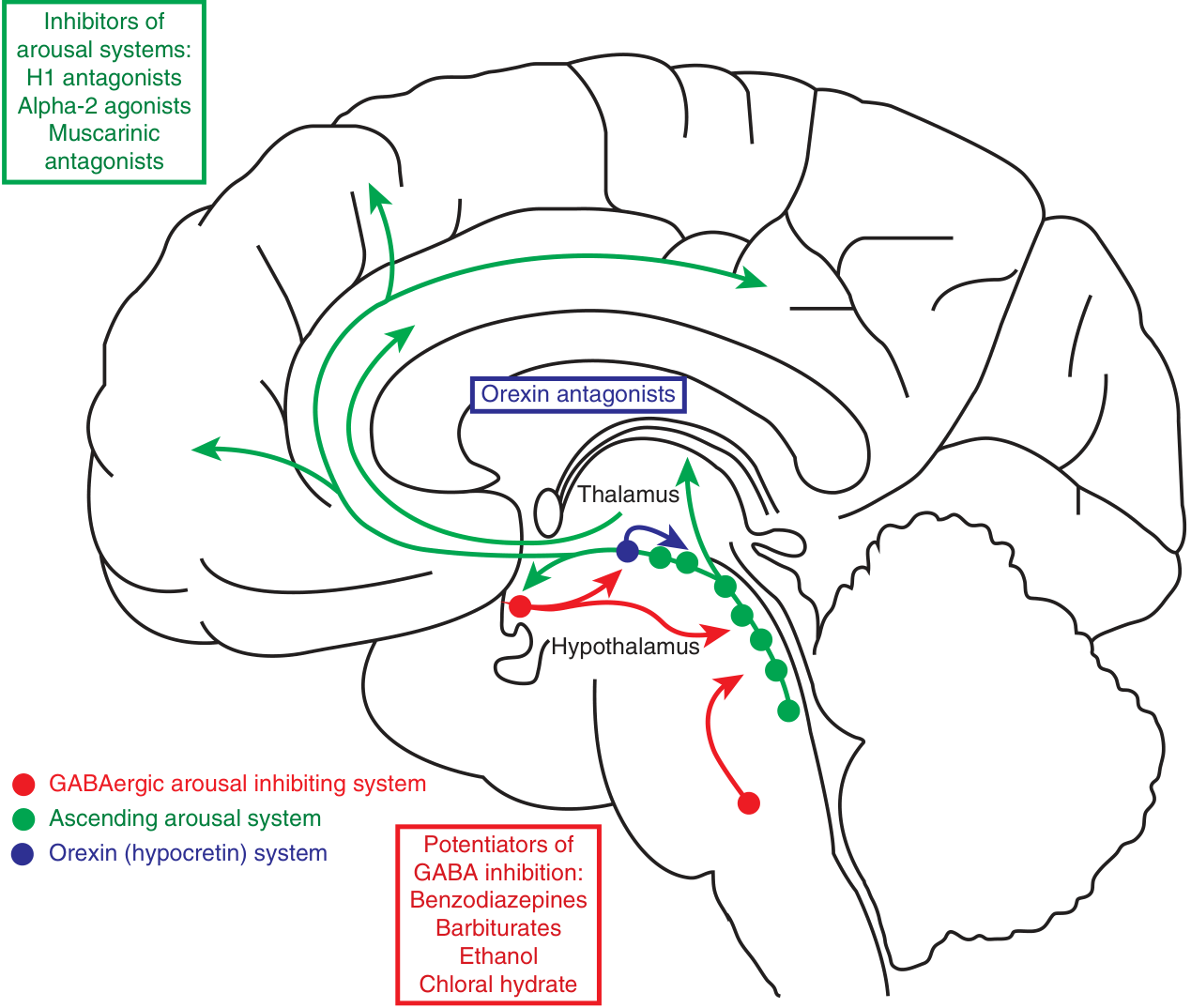
Fig. 33-2 from Harrison's Principles of Internal Medicine: The arousal (green), orexin (blue), and sleep-promoting GABAergic (red) systems
REM Sleep Switch (in brainstem)
- REM-On neurons (upper pons): Use GABA + glutamate; glutamatergic projections cause REM phenomena
- Projections to medulla/spinal cord → activate inhibitory interneurons (GABA + glycine) → hyperpolarize motor neurons → muscle atonia of REM
- Projections to forebrain → produce dreams
- REM-Off neurons (lower midbrain): GABAergic; inhibit REM-On neurons
- Cholinergic input favors REM; norepinephrine + serotonin prevent REM
- (That's why SNRIs and TCAs suppress REM sleep)
6. Homeostatic, Allostatic, and Circadian Regulation
(A) Homeostatic Drive ("Process S")
- The longer you stay awake, the stronger the drive to sleep
- Key mediator: Adenosine - accumulates in the brain during wakefulness
- Acts on A1 receptors → directly inhibits arousal-promoting neurons
- Acts on A2a receptors → activates VLPO sleep-promoting neurons
- Caffeine works by blocking adenosine receptors (A1 and A2a) → blocks sleepiness
- Prostaglandin D2 also accumulates and activates VLPO neurons
- Sleep deprivation → increased N3 (slow-wave) intensity on recovery ("rebound sleep")
(B) Allostatic Drive
- Stress, anxiety, and psychological threats activate the arousal system → insomnia
- Chronic insomnia shows hyperactivation of the ascending arousal system on PET scan
(C) Circadian Rhythm ("Process C")
- Controlled by the Suprachiasmatic Nucleus (SCN) of the anterior hypothalamus
- Intrinsic rhythm of ~25 hours, entrained to 24 hours by light (the most powerful zeitgeber/"time giver")
- SCN → outputs to hypothalamus → impose 24-h rhythms on sleep, temperature, feeding, activity
- Melatonin (from pineal gland) modulates this cyclic activity - rises in darkness, promotes sleep onset
- Destruction of SCN → complete disorganization of sleep-wake cycles
7. Physiological Changes During Sleep
| Parameter | NREM Sleep | REM Sleep |
|---|---|---|
| EEG | Synchronized (slow waves) | Desynchronized (fast, mixed) |
| Eye movements | Slow, roving (N1); absent (N2, N3) | Rapid, conjugate, all directions |
| Muscle tone | Slightly reduced | Near-complete atonia (except diaphragm) |
| Heart rate | Decreased, regular | Irregular, variable (phasic) |
| Blood pressure | Decreased | Fluctuates (phasic) |
| Respiration | Regular, slightly reduced rate | Irregular |
| Temperature | Maintained | Thermoregulation impaired |
| Dreaming | Occurs but less vivid | Vivid, complex, narrative dreams |
| Erection/clitoral tumescence | Absent | Present (useful in diagnosing erectile dysfunction - if present in REM → psychogenic cause) |
| Growth hormone secretion | Peak in N3 (slow-wave sleep) | Minimal |
Key clinical point: REM sleep atonia is mediated by GABA and glycine inhibiting motor neurons. REM Sleep Behavior Disorder (RBD) occurs when this paralysis fails - patients physically act out their dreams and may injure themselves or their bed partner.
8. Effects of Age on Sleep
| Age | Features |
|---|---|
| Neonates | 16-20 h/day; 50% REM (brain development) |
| Children | 10-12 h; consolidation into single night period by age 4-5 |
| Young adults | 7-7.5 h; 20-25% REM; prominent N3 |
| Elderly | ~6 h; N3 may be absent; fragmented sleep; frequent awakenings (VLPO neuron loss); more time awake |
9. Functions of Sleep (Why Do We Sleep?)
- N3 / Slow-wave sleep: Physical restoration, growth hormone secretion, immune function
- REM sleep: Memory consolidation, emotional processing, brain maturation (especially in infancy)
- Overall sleep: Metabolic regulation (glucose, insulin), immune response, cardiovascular health, cognitive function
Consequences of Sleep Deprivation
- Impaired cognition, reaction time, vigilance
- Glucose intolerance → risk of diabetes, metabolic syndrome
- Obesity, immune suppression, atherosclerosis
- Increased risk of cardiovascular disease, Alzheimer's disease, stroke
10. Quick Memory Tricks for Exams
- "BASK in sleep": Brain waves slow down in NREM (B-N1, A-N2 spindles, S-N3 slow wave, K-K complex)
- "REM = Rapid + Relaxed muscles + Real dreams"
- Adenosine = sleep pressure; Caffeine = adenosine blocker = wakefulness
- VLPO = sleep ON; SCN = body clock; Orexin = wake stabilizer
- First 1/3 of night = N3 dominant; Last 1/3 = REM dominant
- Sleep spindles + K complexes = N2 (the most common stage of sleep)
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 253-254 | Adams and Victor's Principles of Neurology, 12th Ed., p. 411
This is a shared conversation. Sign in to Orris to start your own chat.