Explain the topic ultrasound in pregnancy for obg
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the textbooks. Let me compile a thorough OBG-oriented explanation.
Ultrasound in Pregnancy — OBG Overview
Source: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Berek & Novak's Gynecology
1. Introduction & Safety
Obstetric ultrasound is the primary imaging modality in pregnancy. It is non-ionizing and has an extensive safety record when used with proper clinical indication. It uses high-frequency sound waves reflected from tissues to generate real-time images. The ALARA ("as low as reasonably achievable") principle applies — output should be minimized while achieving diagnostically adequate images.
2. Types of Obstetric Ultrasound Examinations
Examinations are categorized by clinical indication and level of detail:
| CPT Code | Examination Type | Description |
|---|---|---|
| 76801 | First trimester (< 14 weeks), transabdominal | Routine first-trimester screening |
| 76805 | Standard (≥ 14 weeks) | Midtrimester anatomy scan — fetal size, anatomy, placenta |
| 76811 | Detailed fetal anatomic exam | For high-risk cases; performed once per pregnancy per practice |
| 76815 | Limited | Answers a discrete question (fetal heart activity, placental location, AFI) |
| 76816 | Follow-up | Repeat exams — growth reassessment, organ re-evaluation |
| 76817 | Transvaginal | Any gestational age via TVS |
| 76818/76819 | Biophysical Profile (BPP) | With or without nonstress test |
3. First-Trimester Ultrasound (< 14 Weeks)
Key Objectives
- Confirm intrauterine pregnancy and exclude ectopic
- Establish gestational age — crown-rump length (CRL) is the most accurate biometric parameter in the first trimester
- Determine fetal cardiac activity
- Assess fetal number and chorionicity in multiples (most accurately determined before 14 weeks)
- Nuchal translucency (NT) measurement at 11–13+6 weeks for Down syndrome and other aneuploidies screening
- Detect major structural anomalies (with emerging evidence for late first-trimester detailed scans)
Crown-Rump Length (CRL)
- Most reliable dating method; accurate to ±5–7 days
- Obtained in a true neutral position — fetus neither hyperflexed nor hyperextended
Nuchal Translucency
- The fluid-filled space at the back of the fetal neck
- NT ≥ 3.0 mm is associated with increased risk of trisomy 21, 18, 13, cardiac defects, and other structural anomalies
- Combined with serum free β-hCG and PAPP-A (combined first-trimester screening) for detection rates of ~85–90%
4. Midtrimester Anatomy Scan (18–22 Weeks) — The "Anatomy Scan"
This is the most important routine obstetric ultrasound examination. It serves as a major checkpoint for:
- Confirming/correcting gestational age by comparing obstetric dates with fetal biometry
- Detecting structural anomalies before fetal viability
- Identifying placental abnormalities (previa, accreta spectrum)
- Detecting uterine abnormalities (fibroids, etc.)
Studies show that a scan at 18–20 weeks detects major structural anomalies in approximately 60% of cases in unselected populations (Gagnon et al.).
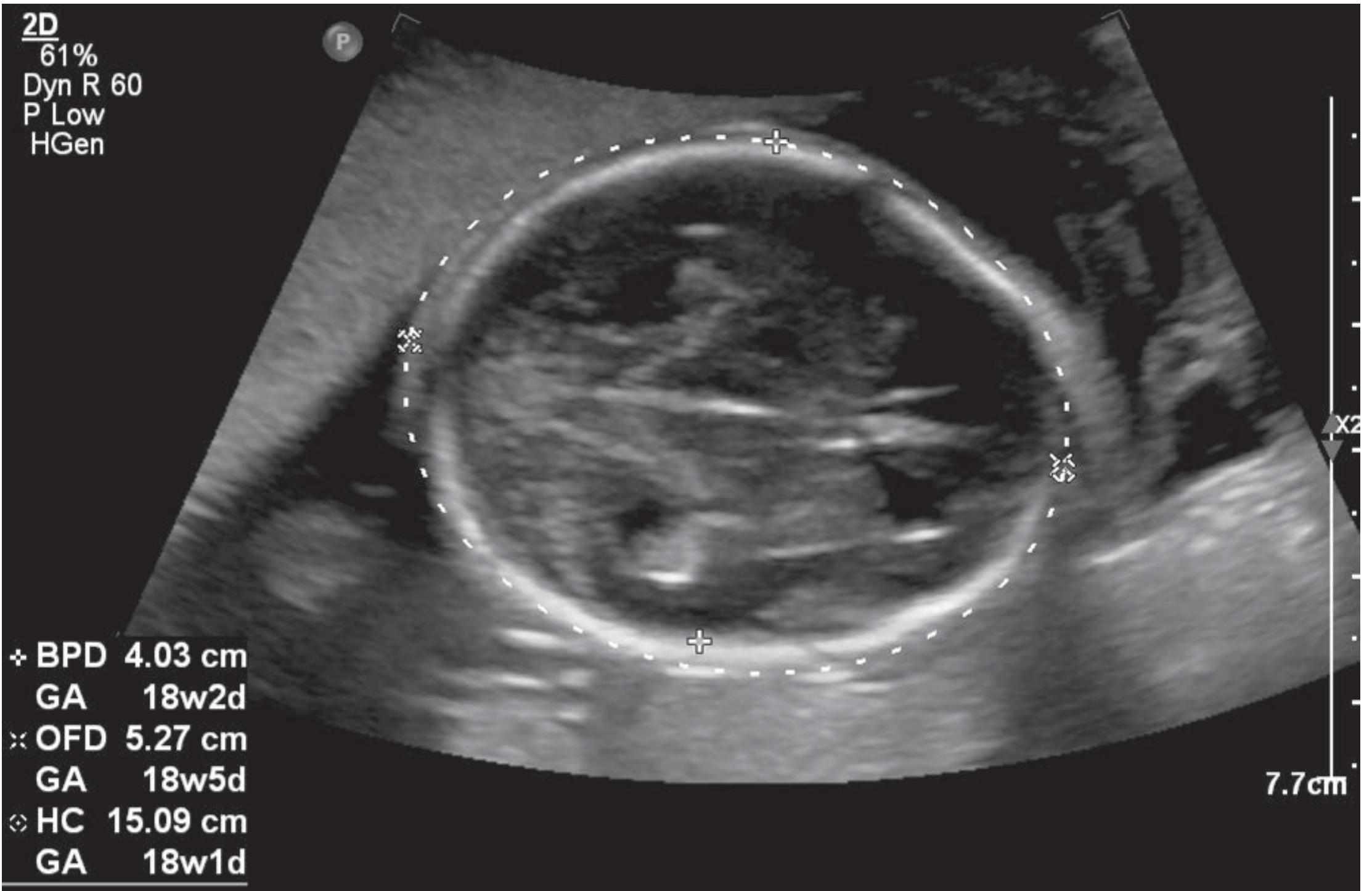
Fetal Biometry (Standard Measurements)
| Measurement | Abbreviation | Plane |
|---|---|---|
| Biparietal diameter | BPD | Axial transthalamic plane |
| Head circumference | HC | Same axial plane |
| Abdominal circumference | AC | Axial plane at stomach/umbilical vein |
| Femur length | FL | Long axis of femur |
These four measurements are used to calculate Estimated Fetal Weight (EFW) and gestational age.
Detailed Fetal Anatomy Checklist (CPT 76805)
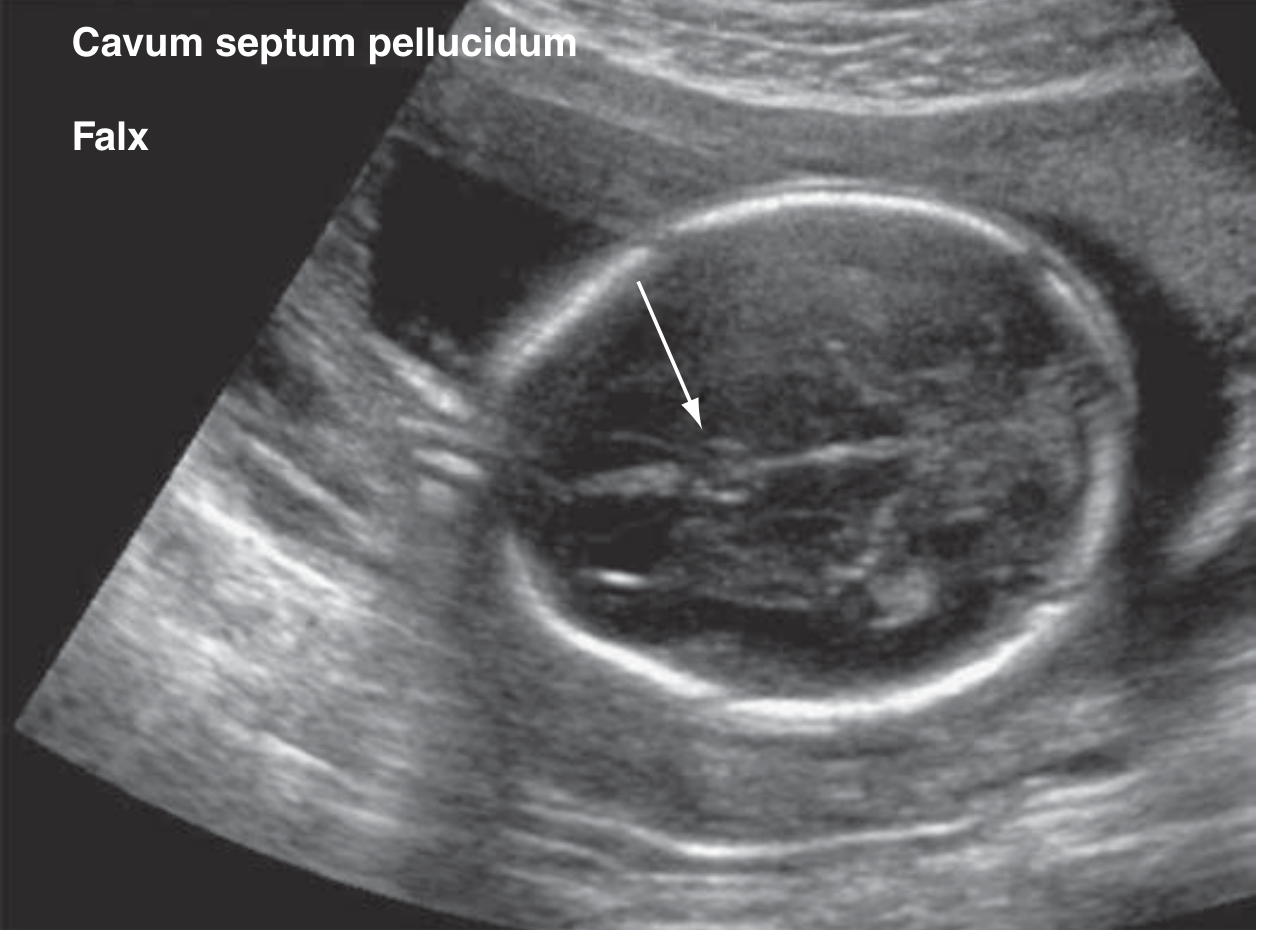
Head & Face
- Cranial bones, falx cerebri, cavum septi pellucidi
- Thalami, lateral ventricles (normal < 10 mm)
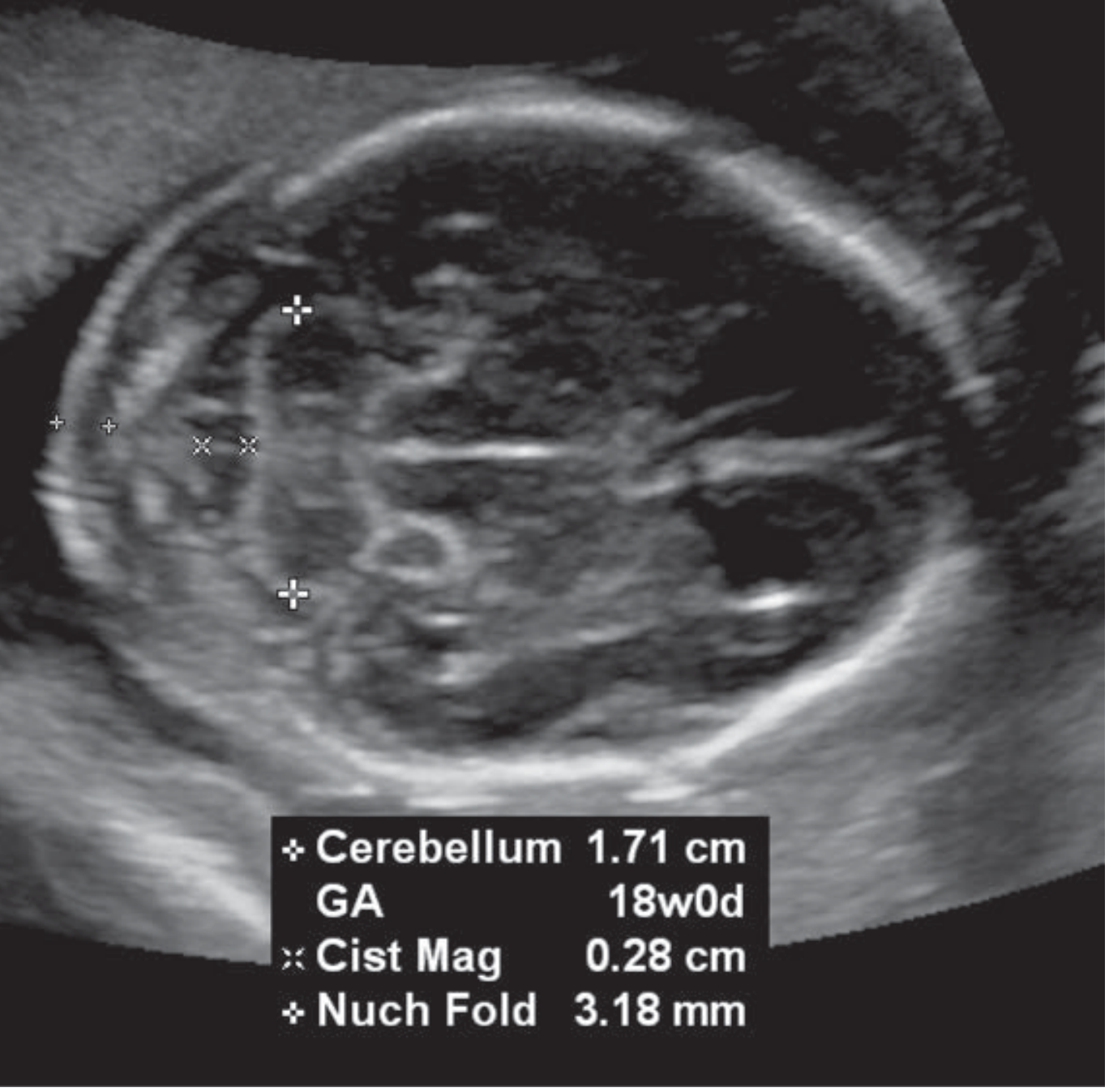
- Cerebellum, cisterna magna
- Orbits, facial profile, nasal bone, upper lip
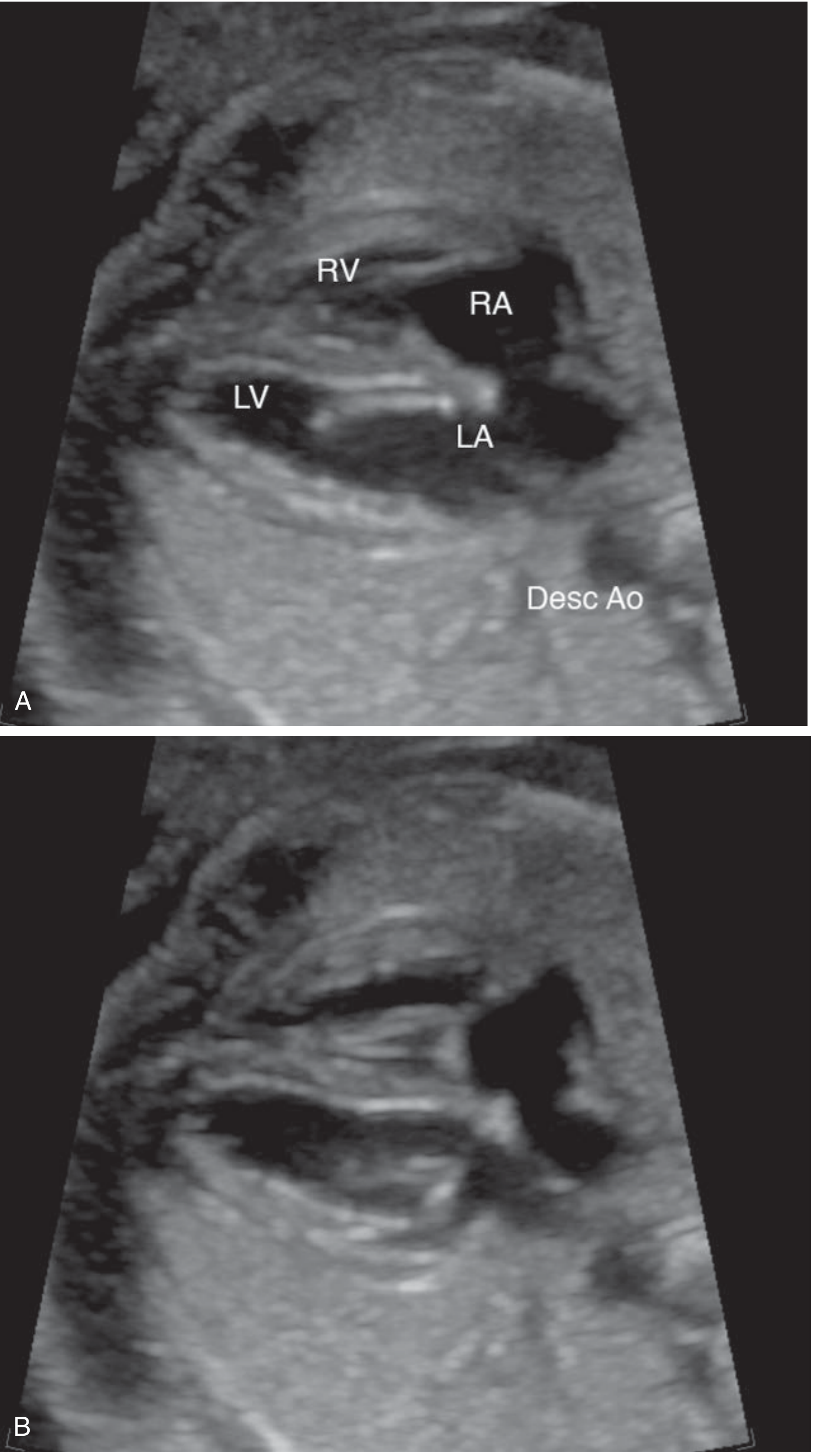
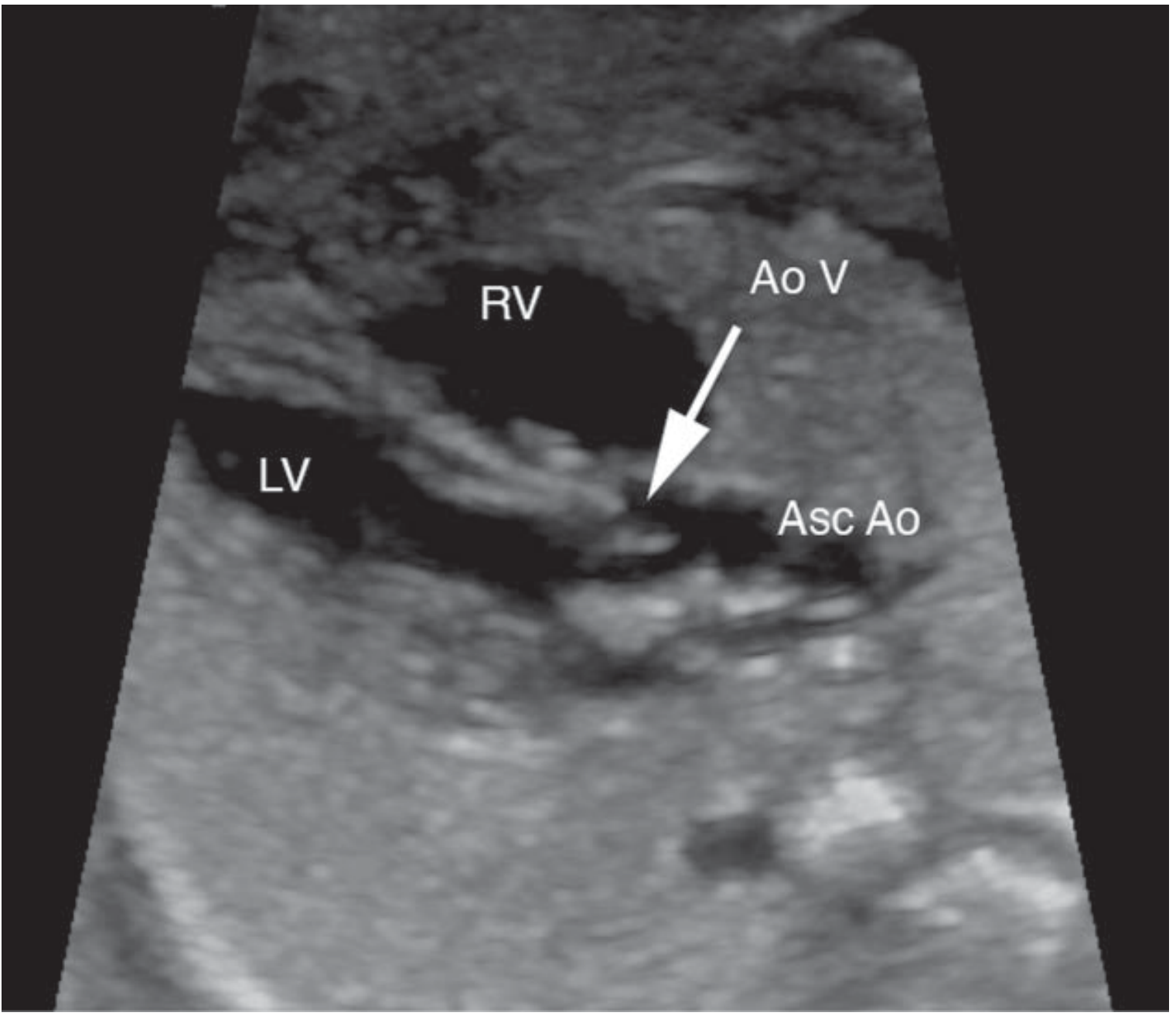
Thorax
- Four-chamber view of the heart
- Cardiac axis (normally ~45° to the left)
- Left and right ventricular outflow tracts
- Lung parenchyma
Abdomen
- Stomach (should be visible and fluid-filled)
- Abdominal umbilical cord insertion
- Kidneys and bladder
- Umbilical arteries (should be two)
Spine & Extremities
- Spine in longitudinal and transverse views
- All four extremities (upper and lower long bones)
- Hand/foot anatomy and posture
- Genitalia

Placenta, Cord & Amniotic Fluid
Placenta:
- Location (note if low-lying or previa)
- Appearance (masses, cysts, lucencies, accessory lobe)
- Umbilical cord insertion site (central/marginal/velamentous)
- Number of umbilical cord vessels (normally 3 — 2 arteries + 1 vein)
Amniotic Fluid Volume:
- Maximum Vertical Pocket (MVP): Normal 2–8 cm
- Amniotic Fluid Index (AFI): Sum of MVPs in four quadrants; normal 5–24 cm
- Oligohydramnios: MVP < 2 cm / AFI < 5 cm
- Polyhydramnios: MVP > 8 cm / AFI > 24 cm
5. Third-Trimester Ultrasound — Growth & Well-being
Fetal Growth Assessment
- Serial biometry every 3–4 weeks in growth-restricted fetuses
- EFW < 10th percentile = small for gestational age (SGA); EFW < 3rd percentile = severely growth-restricted
Biophysical Profile (BPP)
Assesses fetal well-being by scoring five parameters (2 points each, maximum score = 10):
| Parameter | Normal (Score 2) |
|---|---|
| Fetal breathing movements | ≥ 1 episode lasting ≥ 30 seconds in 30 min |
| Gross body movements | ≥ 3 discrete movements in 30 min |
| Fetal tone | ≥ 1 extension/flexion cycle |
| Amniotic fluid volume | MVP ≥ 2 cm |
| Non-stress test (NST) | Reactive (in BPP with NST, CPT 76818) |
Score ≥ 8/10 is reassuring; score ≤ 4/10 warrants delivery or intensive monitoring.
6. Doppler Velocimetry
Doppler ultrasound evaluates blood flow velocity waveforms in fetal and maternal vessels. It is essential for monitoring feto-placental compromise in fetal growth restriction (FGR) and preeclampsia.
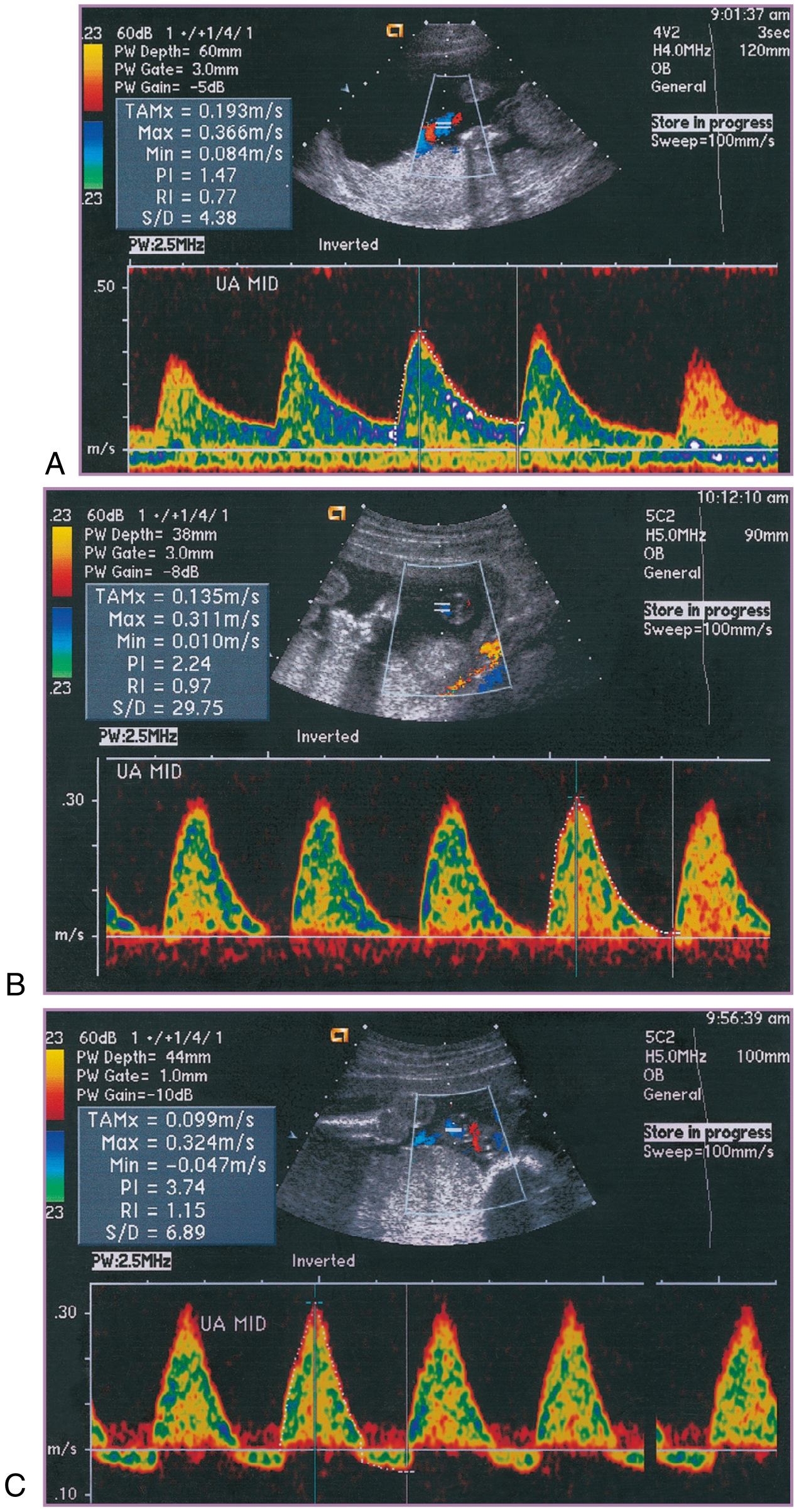
Umbilical Artery (UA) Doppler
- Reflects placental vascular resistance
- Normal: diastolic flow present and progressive throughout pregnancy
- Abnormal patterns (in order of severity):
- Elevated S/D ratio / increased PI, RI — increased resistance
- Absent End-Diastolic Velocity (AEDV) — critical worsening
- Reversed End-Diastolic Velocity (REDV) — imminent fetal compromise; strong indicator for delivery
Middle Cerebral Artery (MCA) Doppler
- Measures MCA Peak Systolic Velocity (PSV)
- Brain-sparing effect: in FGR, MCA resistance decreases (vasodilation) as the fetus preferentially perfuses the brain
- MCA PSV > 1.5 MoM (multiples of the median): hallmark for fetal anaemia (e.g., Rh isoimmunization, hydrops fetalis)
Ductus Venosus (DV) Doppler
- Reflects right heart pressure and venous return
- Absent or reversed a-wave in DV waveform = sign of severe cardiac compromise; indicates imminent fetal acidosis and guides timing of delivery in preterm FGR
7. Cervical Length Assessment
- Transvaginal ultrasound (TVS) is the standard method
- Short cervix (< 25 mm before 24 weeks) predicts preterm birth
- Used to guide decisions on:
- Cervical cerclage
- Progesterone supplementation
- Antenatal corticosteroids
8. Ultrasound Markers for Aneuploidy
First Trimester Markers
| Marker | Association |
|---|---|
| ↑ Nuchal Translucency (≥ 3.0 mm) | Trisomy 21, 18, 13; cardiac defects; Turner syndrome |
| Absent nasal bone | Trisomy 21 |
| Reversed ductus venosus a-wave | Trisomy 21, cardiac defects |
| Tricuspid regurgitation | Trisomy 21 |
Second Trimester "Soft Markers"
| Marker | Main Association |
|---|---|
| Choroid plexus cysts | Trisomy 18 |
| Echogenic intracardiac focus | Trisomy 21 |
| Nuchal fold ≥ 6 mm | Trisomy 21 |
| Short femur/humerus | Trisomy 21 |
| Pyelectasis | Trisomy 21 |
| Echogenic bowel | Trisomy 21, CF, CMV |
9. Special Applications
Multiple Pregnancy
- Chorionicity determination is critical and most accurately assessed at < 14 weeks:
- Dichorionic-diamniotic (DCDA): "Twin peak" (lambda sign) — triangular wedge of placental tissue between membranes
- Monochorionic-diamniotic (MCDA): "T-sign" — membrane inserts at right angle to placenta
- Ultrasound staging of Twin-Twin Transfusion Syndrome (TTTS) using Quintero criteria (based on UA, UV, DV Doppler and amniotic fluid discordance)
- Detection of Selective FGR in monochorionic twins
Placental Abnormalities
- Placenta previa: Placenta covering the internal os — typically confirmed by TVS at 32–36 weeks
- Placenta accreta spectrum: Abnormal placentation suspected on grey-scale and colour Doppler — loss of retroplacental clear space, placental lacunae, bridging vessels to bladder
10. Reporting Requirements
Every obstetric ultrasound report must include:
- Patient identifying information and date
- Indication for the procedure and type of examination
- Gestational age by established dates
- Number of fetuses (and chorionicity if multiples)
- Fetal biometry with predicted gestational age
- Principal findings (normal, abnormal, or poorly visualized)
- Differential diagnosis for abnormalities
- Recommendations for management or follow-up
Summary Table: Ultrasound Schedule in Normal Pregnancy
| Timing | Examination | Key Parameters |
|---|---|---|
| 7–10 weeks | Early pregnancy | Confirm IUP, CRL, cardiac activity, number |
| 11–13+6 weeks | NT scan | NT, nasal bone, CRL, chorionicity |
| 18–22 weeks | Anatomy scan (level II) | Full fetal anatomy, biometry, placenta, AFI |
| 28–32 weeks | Growth scan | Biometry, EFW, AFI, presentation |
| 36+ weeks | Term scan | Presentation, AFI, BPP if indicated |
| Any trimester | Doppler | UA, MCA, DV when FGR or anaemia suspected |
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (9780323828499), pp. 318–335; Berek & Novak's Gynecology (9781496380357)
This is a shared conversation. Sign in to Orris to start your own chat.