Hand shoulder syndrome
"hand shoulder syndrome" OR "shoulder hand syndrome" reflex sympathetic dystrophy
Hand shoulder syndrome pg Orthopaedics structure answer Introduction 2. History (if relevant) 3. Anatomy 4. Etiology 5. Mechanism (if applicable) 6. Pathology 7. Clinical Features 8. Investigation 9. Radiograph 10. CT 11. MRI 12. Classification 13. Treatment A. Non-operative B. Operative 14. Recent Advances
"shoulder hand syndrome" OR "complex regional pain syndrome" treatment
"complex regional pain syndrome" spinal cord stimulation ketamine
Hand-Shoulder Syndrome (Shoulder-Hand Syndrome / Complex Regional Pain Syndrome Type I)
1. Introduction
- Disproportionate, intractable burning pain involving both the hand and shoulder
- Autonomic dysregulation (vasomotor and sudomotor dysfunction)
- Trophic changes progressing to contracture and osteoporosis
- Campbell's Operative Orthopaedics 15th Ed 2026, p. 3843
- Adams and Victor's Principles of Neurology 12th Ed, p. 1371
2. History
- 1864 - Weir Mitchell first described "causalgia" in Civil War soldiers with peripheral nerve injuries
- 1900 - Paul Sudeck described post-traumatic bone atrophy ("Sudeck's atrophy")
- 1947 - Steinbrocker & Argyros coined "shoulder-hand syndrome" for the hand-shoulder variant
- 1979 - Excellent review by Genant covering stages and importance of early treatment
- 1994 - IASP taxonomy committee replaced RSD/causalgia with CRPS Type I and II
- 2003 - Budapest diagnostic criteria validated by Harden et al., now the gold standard
- 2010s-present - Central sensitization, neuroplasticity, and cortical reorganization recognized as key mechanisms
3. Anatomy
- Sympathetic efferent fibers traveling with the brachial plexus and peripheral nerves (median, ulnar, radial) to the hand
- Somatic afferent nociceptive C-fibers and A-delta fibers
- Stellate ganglion (C7-T1) - key sympathetic relay for the upper limb
- Glenohumeral joint, rotator cuff, shoulder capsule, acromioclavicular and sternoclavicular joints
- Subacromial bursa - commonly involved in trophic changes
- Intrinsic muscles of the hand, finger flexors/extensors
- Metacarpophalangeal and interphalangeal joints
- Skin, subcutaneous tissue, nails, hair follicles - all affected by trophic changes
- Internuncial pool (Stage 2 short-circuiting)
- Ascending spinothalamic tracts
- Descending cortical modulation (thalamic centers in Stage 3)
- Dorsal horn NMDA receptors - central sensitization site
4. Etiology
| Category | Specific Causes |
|---|---|
| Trauma (most common) | Fracture of distal radius (Colles'), crush injury, soft tissue injury (~40%), fracture (~25%) |
| Cardiac | Myocardial infarction (~12%), cardiac surgery |
| Neurological | Stroke (hemiplegia), cervical disc disease, brachial plexus injury |
| Iatrogenic | Post-operative (any UL surgery), IV/arterial cannulation, shoulder surgery |
| Metabolic/Systemic | Diabetes mellitus (diabetic hand-shoulder syndrome), chemical/electrical burns |
| Infective | Postherpetic neuralgia |
| Immobilization | Prolonged cast, splint, or postoperative immobilization |
| Idiopathic | Up to 10-15% - no identifiable cause |
- Female sex (female predominance)
- Smoking
- Emotional/psychological distress at time of onset
- Anxiety and catastrophizing personality traits
5. Mechanism / Pathophysiology
A. Sympathetic Overflow Theory (Classic)
- Peripheral injury causes abnormal reflex arc through the sympathetic nervous system
- Sympathetic overflow leads to vasomotor instability, edema, and pain amplification
B. Catecholamine Hypersensitivity
- Decreased sympathetic outflow to the affected limb paradoxically causes upregulation of adrenergic receptors on nociceptors
- Circulating or locally secreted catecholamines trigger abnormal afferent pain activity
C. Ephaptic Transmission (Short-Circuiting)
- Abnormal direct electrical coupling between efferent sympathetic fibers and somatic afferent pain fibers at the nerve injury site
- Stage 1: Peripheral short-circuiting
- Stage 2: Short-circuiting at the internuncial pool in spinal cord
- Stage 3: Higher thalamic center involvement
D. Central Sensitization (Modern View)
- Sustained nociceptive bombardment sensitizes central sensory structures
- Molecular changes at dorsal horn: NMDA receptor alterations, cyclooxygenase/prostaglandin induction, changes in GABAergic inhibition
- Maladaptive neuroplasticity - cortical reorganization with expansion of pain representation map
- Explains nondermatomal, nonsclerotomal distribution of symptoms
E. Inflammatory Mediators
- Release of pro-inflammatory neuropeptides (substance P, CGRP)
- Mast cell degranulation
- Neurogenic inflammation perpetuates the vicious cycle
6. Pathology
- Early: Soft tissue edema, erythema, warmth
- Late: Shiny, smooth, atrophic skin; thin, brittle nails; hair loss; waxy appearance; flexion contractures
- Fibrosis of joint capsule and periarticular soft tissues (similar to but more severe than disuse atrophy)
- Periarticular demineralization of bone (juxtaarticular osteoporosis)
- Synovial tissue: lymphocytic infiltration and fibrosis in late stages
- Skin: Epidermal thinning, dermal fibrosis, decreased hair follicles and sweat glands
- Progressive periarticular bone resorption and osteopenia
- Medullary bone involvement in later stages
- Changes driven by inflammatory cytokines stimulating osteoclast activity
7. Clinical Features
Symptom Complex (Four Domains - Budapest Criteria)
| Domain | Symptoms | Signs |
|---|---|---|
| Sensory | Hyperesthesia, allodynia, burning/throbbing pain | Hyperalgesia to pinprick, allodynia to light touch |
| Vasomotor | Temperature asymmetry, skin color changes | Temperature difference >1°C, mottling/cyanosis/erythema |
| Sudomotor/Edema | Altered sweating, swelling | Edema, hyperhidrosis or anhidrosis |
| Motor/Trophic | Weakness, stiffness, decreased ROM | Tremor, dystonia, trophic changes in hair/nails/skin |
Three Classical Stages (Bonica / Bradley Classification)
- Severe diffuse burning pain, often described as throbbing
- Pain exceeds what the injury would normally produce
- Localized edema of hand and wrist
- Vasomotor disturbances: skin erythema, warmth, increased sweating
- Limitation of shoulder movement with periarthritis
- Radiograph: early patchy osteoporosis
- Progression of soft tissue edema
- Thickening of skin and articular soft tissues; muscle wasting
- Vasomotor shift: extremity becomes cold, cyanotic
- Skin becomes shiny, smooth, devoid of hair
- Shoulder progressively stiffens ("frozen shoulder")
- Pain remains severe and intractable
- Radiograph: progression of periarticular demineralization
- Irreversible trophic changes: waxy skin, brittle ridged nails, severe muscle atrophy
- Flexion contracture of digits and wrist - "intrinsic minus" hand
- Frozen shoulder (complete loss of glenohumeral motion)
- Extremity is pale, cold, and painful
- Lymphedema
- Radiograph: severe demineralization
- Loss of employment and social relationships
- Depression, suicidal ideation
- Orthostatic hypotension, hypertension
- Unnecessary repeated surgeries

8. Investigations
| Investigation | Finding | Utility |
|---|---|---|
| Plain X-ray | Periarticular osteoporosis, demineralization | Staging, baseline |
| Triple-phase bone scan | Most sensitive early test | Confirmatory |
| Thermography | Skin temperature asymmetry >1°C | Sympathetic dysfunction |
| Autonomic testing | QSART (quantitative sudomotor axon reflex test) | Sympathetic dysfunction |
| MRI | Bone marrow edema, muscle edema, interstitial edema | Differential diagnosis |
| Limb volume measurement | Submersion testing | Edema quantification |
| CBC, ESR, CRP | Normal or mildly elevated | Exclude infection/inflammatory |
| Blood glucose, HbA1c | Exclude diabetic cheiroarthropathy | |
| EMG/NCS | Differentiate CRPS I from CRPS II (nerve injury) |
9. Radiograph (Plain X-ray)
- Early (Stage I): Subtle periarticular osteopenia, patchy "spotty" rarefaction most marked in juxtaarticular regions
- Progressive: Diffuse osteoporosis extending through the hand, wrist, and shoulder
- Late (Stage III): Severe demineralization, cortical thinning, subperiosteal bone resorption
- Pattern: Predominantly juxta-articular, affecting metacarpal heads, carpal bones, distal radius/ulna, proximal humerus
- Subchondral bone lucency (not erosion - distinguishes from RA)
- "Sudeck's atrophy" pattern: Characteristic mottled, "moth-eaten" appearance of bones of the hand
10. CT Scan
- Characterizing fracture patterns that may have precipitated CRPS
- Differentiating from bone tumors when malignancy is suspected
- CT arthrography of shoulder: Evaluating capsular adhesions, labral pathology in frozen shoulder component
- Documenting the extent of periarticular osteoporosis more precisely than plain film
- Not superior to bone scan or MRI for primary diagnosis of CRPS
11. MRI
| Finding | Significance |
|---|---|
| Bone marrow edema (high T2, low T1) | Periarticular and diffuse - reflects hyperemia and inflammatory mediators |
| Soft tissue edema | Periarticular and subcutaneous - diffuse T2 hyperintensity |
| Muscle edema | Interstitial edema on STIR/T2 sequences |
| Synovitis | Enhancement on contrast (Gadolinium) |
| Joint effusion | Glenohumeral or hand joints |
| Skin thickening | Late trophic changes |
- More sensitive than plain X-ray for early changes
- Demonstrates diffuse signal abnormalities distinguishing CRPS from focal lesions (tumor, infection)
- Still not very sensitive or specific for CRPS diagnosis (Campbell's, p. 3845)
- Most useful for differential diagnosis - ruling out AVN, osteomyelitis, neoplasm
- Bone marrow edema pattern seen before radiographic osteoporosis
12. Classification
A. IASP Classification (Current Standard)
| Type | Former Name | Definition |
|---|---|---|
| CRPS Type I | Reflex Sympathetic Dystrophy (RSD) | Same clinical features BUT without evidence of a defined nerve injury |
| CRPS Type II | Causalgia | Same clinical features WITH evidence of a defined peripheral nerve injury |
B. Subtypes by Sympathetic Mediation
- Sympathetically Maintained Pain (SMP): Responds to sympathetic blockade - warm subtype (early), erythematous, hyperhidrotic
- Sympathetically Independent Pain (SIP): No response to sympathetic blockade - cold subtype (late), pale, atrophic
C. Bonica's Staging (Temporal/Clinical)
- Stage 1 (Dysfunction): Acute - 1-3 months
- Stage 2 (Dystrophy): Subacute - 3-7 months
- Stage 3 (Atrophy): Chronic - >7 months
- Stage 4: Advanced - social/systemic consequences
D. Budapest Diagnostic Criteria (2003/2007 - Harden et al.)
- Continued pain disproportionate to any inciting event
- At least one symptom in 3 of 4 categories (sensory, vasomotor, sudomotor/edema, motor/trophic)
- At least one sign at time of diagnosis in 2 or more categories
- No other diagnosis better explains the signs and symptoms
13. Treatment
A. Non-Operative Treatment
1. Physical and Occupational Therapy (First-line)
- Active function-oriented program - most important element
- Graded motor imagery (GMI): mental rehearsal of limb movements before actual use
- Mirror therapy: mirror-assisted movement patterns
- Desensitization techniques
- Edema control: elevation, retrograde massage, compressive gloves
- TENS (Transcutaneous Electrical Nerve Stimulation)
- Hydrotherapy
- Shoulder mobilization to prevent/treat frozen shoulder
- Pediatric patients: high-intensity PT alone shows favorable responses
2. Pharmacological Treatment
| Drug Class | Examples | Mechanism/Role |
|---|---|---|
| NSAIDs | Ibuprofen, naproxen | Anti-inflammatory, analgesic |
| Bisphosphonates | Alendronate, pamidronate, neridronate | Inhibit bone resorption, analgesic; strong evidence |
| Calcitonin | Intranasal or SC | Anti-osteoclastic, analgesic effect via CNS |
| Corticosteroids | Prednisolone | Reduce neurogenic inflammation; useful in early acute stage |
| Tricyclic antidepressants | Amitriptyline, nortriptyline | Central pain modulation, neuropathic pain |
| SSRIs / SNRIs | Duloxetine | Descending pain modulation |
| Anticonvulsants | Gabapentin, pregabalin | Neuropathic pain, reduces central sensitization |
| Alpha-blockers | Prazosin, phenoxybenzamine | Sympathetically mediated pain |
| Calcium channel blockers | Nifedipine, verapamil | Vasomotor symptoms |
| Beta-blockers | Propranolol | Sympathetic modulation |
| Guanethidine | IV regional (Bier block) | Peripheral sympatholytic |
| Ketamine infusion | Sub-anesthetic dose IV | NMDA receptor antagonist; use in refractory cases |
| Vitamin C | 500 mg/day perioperatively | Prophylactic - reduces CRPS after distal radius fracture |
| Free radical scavengers | DMSO topical | Anti-inflammatory |
3. Sympathetic Nerve Blocks (Procedural/Non-Surgical)
- Stellate Ganglion Block (SGB): Most important procedure for upper extremity CRPS/HSS
- Sequential series of blocks combined with physical therapy
- 80-93% success rate reported in published series (Campbell's)
- Can be repeated if successful
- Also serves as a diagnostic test for sympathetically maintained pain
- Intravenous Regional Block (Bier Block): Lidocaine ± guanethidine ± corticosteroid
- Poplawski et al.: best predictor of success = treatment onset <6 months
- Trigger point injections: For associated myofascial pain around shoulder
- Intra-articular shoulder injection: Corticosteroid for frozen shoulder component
4. Psychological Support
- Cognitive behavioral therapy (CBT)
- Pain coping strategies, relaxation techniques
- Address secondary gain issues
- Management of depression and emotional lability
B. Operative Treatment
1. Surgical Sympathectomy
- Indication: CRPS with documented response to sympathetic nerve blocks that is not sustained
- Procedure: Cervicothoracic sympathectomy (C7-T2 ganglia excision)
- Open: posterior approach or anterior supraclavicular approach
- Endoscopic/Video-assisted thoracoscopic sympathectomy (VATS) - modern preferred approach
- Results: Reported improvement in patients who had prior temporary response to sympathetic blockade
- Complications: Horner's syndrome, compensatory hyperhidrosis, pneumothorax (VATS)
2. Spinal Cord Stimulation (SCS) / Dorsal Column Stimulation
- Indication: Refractory CRPS not responding to conservative measures and sympathetic blocks
- Electrodes placed epidurally at C5-C7 for upper extremity HSS
- Mechanism: Gate control theory, inhibition of ascending pain pathways
- Evidence: Provides pain relief and improved function in select patients
- Newer systems: Burst stimulation, high-frequency (10 kHz) stimulation may be superior to conventional tonic SCS
3. Intrathecal Drug Delivery
- Implanted intrathecal pump for opioids, baclofen (for dystonia component), clonidine, or ziconotide
- Reserved for severe refractory cases
- Baclofen particularly useful when CRPS-dystonia syndrome is present
4. Peripheral Nerve Ablation/Neurolysis
- Selective ablation of identified peripheral nerve branches
- Limited evidence; not a primary surgical option
5. Joint Procedures for Sequelae
- Shoulder manipulation under anaesthesia (MUA) or arthroscopic capsular release for fixed frozen shoulder (Stage III)
- Digital joint contracture release - reserved for irreversible flexion contractures
- Note: Surgery should be done with extreme caution as it can worsen CRPS
14. Recent Advances
A. Pathophysiology
- Central sensitization and cortical reorganization: Cortical remapping using fMRI shows altered somatosensory and motor cortex representation - basis for mirror therapy and GMI
- Autoimmune hypothesis: IgM autoantibodies against nervous tissue antigens found in CRPS patients; IVIG trials underway
- Neuro-inflammation: Role of mast cells, TNF-alpha, IL-1, IL-6, and CGRP in perpetuating peripheral sensitization
B. Diagnostic Advances
- Quantitative sensory testing (QST): Systematic detection of thermal and mechanical sensory thresholds
- Infrared thermography: Digital asymmetry mapping for objective temperature measurement
- Skin biopsy: Intraepidermal nerve fiber density (IENFD) assessment to differentiate small fiber neuropathy
C. Treatment Advances
Graded Motor Imagery (GMI)
- Three-step progressive program: Laterality recognition → Motor imagery → Mirror therapy
- Targets cortical reorganization directly
- Evidence 2023 supports GMI as first-line adjunct
Bisphosphonates - Strong Evidence
- Neridronate (IV) has shown best evidence in RCTs for CRPS (Varenna et al.)
- Pamidronate IV and alendronate also used
Ketamine Infusion Protocol
- Sub-anesthetic ketamine (0.1-0.5 mg/kg/hr IV) as NMDA receptor antagonist
- Reference consensus protocol published
- Used for refractory CRPS; evidence remains moderate quality
Stellate Ganglion Block - Meta-analysis Evidence
- 2024 systematic review and meta-analysis (PMID: 38805523) confirmed efficacy of SGB for CRPS with significant pain reduction
Spinal Cord Stimulation Advances
- Burst SCS and High-frequency (10 kHz) SCS superior to conventional tonic stimulation
- Dorsal Root Ganglion (DRG) Stimulation - more targeted stimulation for CRPS; promising results in upper extremity involvement
- Closed-loop SCS systems with real-time feedback being trialed
Low-Level Laser Therapy (LLLT)
- Emerging evidence for pain reduction and improved function in early CRPS
Virtual Reality (VR) / Augmented Reality
- VR-based mirror therapy and body illusions for cortical reorganization
- Early phase trials showing promise
Intravenous Immunoglobulin (IVIG)
- Based on autoimmune hypothesis
- Small RCTs show benefit in refractory CRPS; larger trials needed
Vitamin C Prophylaxis
- Strong evidence for 500 mg/day for 50 days post distal radius fracture reducing CRPS incidence (Zollinger et al.)
Summary Table
| Feature | Details |
|---|---|
| Eponym | Steinbrocker's shoulder-hand syndrome (1947) |
| Modern term | CRPS Type I |
| Pathology | Sympathetic/central sensitization dysregulation |
| Most common trigger | Trauma (fracture, soft tissue injury, post-surgical) |
| Key clinical triad | Pain + autonomic features + trophic changes |
| Best diagnostic test | Triple-phase bone scan (early); Budapest criteria (clinical) |
| Best imaging for differentiation | MRI (bone marrow edema, excludes other diagnoses) |
| Stages | I: Dysfunction → II: Dystrophy → III: Atrophy |
| Key prognostic factor | Treatment within 6 months of onset |
| First-line treatment | Multidisciplinary PT + pharmacotherapy + SGB |
| Surgical option | Cervicothoracic sympathectomy (VATS); SCS |
| Recent advance | DRG stimulation; IVIG; ketamine protocol; GMI |
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 67 (p. 3843-3846)
- Adams and Victor's Principles of Neurology 12th Ed (p. 1365-1375)
- Bradley and Daroff's Neurology in Clinical Practice (p. 551)
- Firestein & Kelley's Textbook of Rheumatology (p. 9091-9132)
- Rheumatology 2-Volume Set, Elsevier 2022 (p. 3584-3607)
- Harrison's Principles of Internal Medicine 22E 2025 (p. 823)
- Grainger & Allison's Diagnostic Radiology (p. 2563)
- Limerick G et al. Curr Pain Headache Rep 2023
- Abd-Elsayed A et al. Ann Med 2024
- Candan B & Gungor S. Diagnostics 2025
- Tian Y et al. Pain Physician 2024 - SGB meta-analysis PMID: 38805523
Provide flow chart and diagram of present
Medical flowchart titled "Hand-Shoulder Syndrome (CRPS Type I) - Pathophysiology & Stages" on white background. Professional medical diagram style with clean boxes and arrows. Show: TOP: "TRIGGERING EVENT" box (trauma/fracture/MI/stroke/post-surgical/idiopathic) with red border Arrow down to: "SYMPATHETIC NERVOUS SYSTEM DYSREGULATION" in orange box Two branches: Left: "Peripheral Sensitization" (C-fiber sensitization, nociceptor upregulation, catecholamine hypersensitivity) Right: "Central Sensitization" (NMDA receptor changes, dorsal horn sensitization, cortical reorganization) Both arrows converge to: "NEUROGENIC INFLAMMATION" (Substance P, CGRP, mast cell activation, IL-1, IL-6, TNF-alpha) Arrow down to THREE STAGE progression shown as horizontal timeline with boxes: STAGE I - DYSFUNCTION (1-3 months): Red box - Burning pain, Edema, Warmth, Erythema, Hyperhidrosis, X-ray: Patchy osteoporosis STAGE II - DYSTROPHY (3-7 months): Orange box - Cold extremity, Shiny skin, Hair loss, Muscle wasting, Frozen shoulder, Progressive demineralization STAGE III - ATROPHY (>7 months): Dark purple box - Waxy skin, Brittle nails, Flexion contracture, Pale cold extremity, Severe osteoporosis, IRREVERSIBLE Arrow pointing up from stages labeled "EARLY TREATMENT = REVERSAL POSSIBLE" Arrow pointing down from Stage III labeled "POOR PROGNOSIS" Bottom note box: "KEY: Treatment within 6 months = best outcome" in green Clean arrows, color-coded stages, medical illustration style, highly readable text, 1200x900 resolution
Medical treatment algorithm flowchart titled "Hand-Shoulder Syndrome - Management Algorithm" on clean white background. Professional clinical flowchart with decision diamonds and process boxes. START (green oval): "Patient presents with disproportionate hand/shoulder pain + autonomic features" Arrow down to DIAMOND: "Budapest Criteria Met? (4 criteria)" - NO branch right → "Consider differential diagnosis: RA, infection, DVT, tumor, fibromyalgia" - YES branch down Arrow down to BOX: "INVESTIGATIONS" (blue): X-ray both sides | Triple-phase bone scan | MRI | EMG/NCS | Thermography | QSART Arrow down to DIAMOND: "Stage Assessment" Three branches: LEFT: "Stage I (Acute <3mo)" CENTER: "Stage II (Dystrophic 3-7mo)" RIGHT: "Stage III (Atrophic >7mo)" From ALL THREE stages → converge to: "MULTIDISCIPLINARY FIRST-LINE TREATMENT" (green box): • Physical Therapy + Occupational Therapy • Graded Motor Imagery + Mirror Therapy • Psychological support + CBT • Vitamin C 500mg/day Below that, parallel box: "PHARMACOTHERAPY" (blue): • NSAIDs / Analgesics • Bisphosphonates (Neridronate/Pamidronate) • Calcitonin • Gabapentin/Pregabalin • TCAs / SSRIs • Corticosteroids (early stage) Arrow down to DIAMOND: "Response to conservative Rx after 3-6 months?" YES → "Continue, taper, maintain PT" (green) NO → Arrow down "INTERVENTIONAL PROCEDURES" (orange box): • Stellate Ganglion Block (serial) • IV Regional Block (Bier block) • Trigger point injections • Ketamine infusion (refractory) DIAMOND: "Sustained response?" YES → Continue (green) NO → Arrow down to "SURGICAL OPTIONS" (red box): • Cervicothoracic Sympathectomy (VATS) • Spinal Cord Stimulation (SCS) • DRG Stimulation • Intrathecal drug delivery • Joint release (sequelae only) Clean professional design, color coded boxes, decision diamonds, readable fonts, 1200x1000 resolution
Medical anatomy and mechanism diagram titled "Hand-Shoulder Syndrome - Anatomical Basis & Mechanism" on white background. Split into two panels side by side. LEFT PANEL - "Anatomical Structures Involved": Draw a simple outline of upper limb from shoulder to hand. Label with arrows: - SHOULDER: Glenohumeral joint, Rotator cuff, Shoulder capsule, Subacromial bursa - NECK/SPINE: Stellate ganglion (C7-T1) shown as star symbol, Brachial plexus - ARM: Sympathetic nerve fibers running alongside brachial artery - WRIST & HAND: Median/Ulnar/Radial nerves, Intrinsic muscles, MCP/IP joints, Skin/nails/hair - SPINAL CORD inset: dorsal horn, internuncial pool, spinothalamic tract RIGHT PANEL - "Vicious Cycle of CRPS" shown as circular diagram with arrows going clockwise: 1. "INJURY / TRIGGER" (top, red) → 2. "Nociceptor Activation" → 3. "Sympathetic Overflow" → 4. "Catecholamine Release + Hypersensitivity" → 5. "Neurogenic Inflammation (SP, CGRP, mast cells)" → 6. "Vasomotor + Sudomotor Dysfunction" → 7. "Tissue Hypoxia + Edema" → 8. "Central Sensitization (NMDA, dorsal horn)" → back to "AMPLIFIED PAIN" in center of circle (red bold text) Breaking the cycle labeled with green arrow: "SYMPATHETIC BLOCK / TREATMENT interrupts here" Color scheme: blue for anatomy, red/orange for pain pathway, green for treatment arrows. Professional medical illustration, clear labels, 1200x900
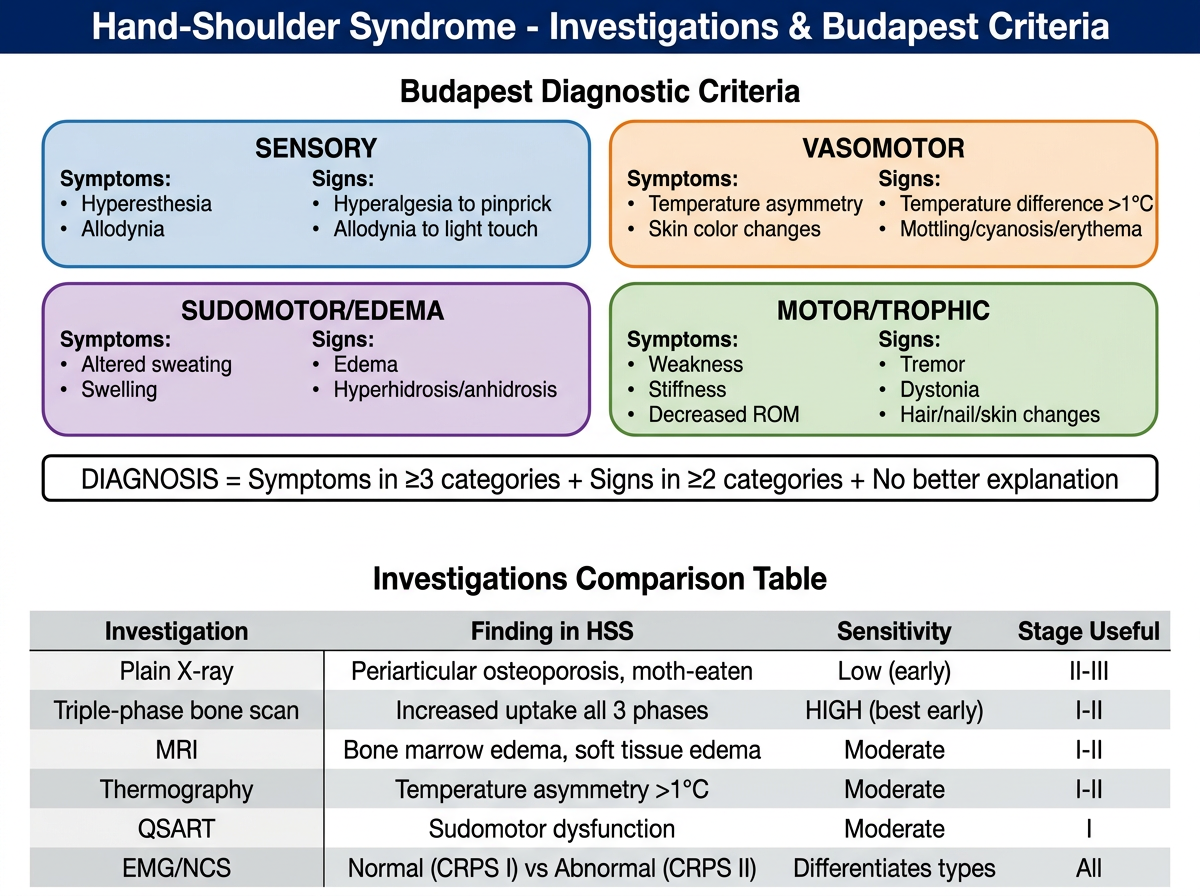
Medical investigation and classification summary diagram for "Hand-Shoulder Syndrome - Investigations & Budapest Criteria" on clean white background. Two sections: TOP HALF - "Budapest Diagnostic Criteria" shown as a 2x2 grid of colored boxes: Box 1 (SENSORY - blue): Symptoms: Hyperesthesia, Allodynia | Signs: Hyperalgesia to pinprick, Allodynia to light touch Box 2 (VASOMOTOR - orange): Symptoms: Temperature asymmetry, Skin color changes | Signs: Temperature difference >1°C, Mottling/cyanosis/erythema Box 3 (SUDOMOTOR/EDEMA - purple): Symptoms: Altered sweating, Swelling | Signs: Edema, Hyperhidrosis/anhidrosis Box 4 (MOTOR/TROPHIC - green): Symptoms: Weakness, Stiffness, Decreased ROM | Signs: Tremor, Dystonia, Hair/nail/skin changes Below the grid, rule box: "DIAGNOSIS = Symptoms in ≥3 categories + Signs in ≥2 categories + No better explanation" BOTTOM HALF - "Investigations Comparison Table" as a clean table: Column headers: Investigation | Finding in HSS | Sensitivity | Stage Useful Row 1: Plain X-ray | Periarticular osteoporosis, moth-eaten | Low (early) | II-III Row 2: Triple-phase bone scan | Increased uptake all 3 phases | HIGH (best early) | I-II Row 3: MRI | Bone marrow edema, soft tissue edema | Moderate | I-II Row 4: Thermography | Temperature asymmetry >1°C | Moderate | I-II Row 5: QSART | Sudomotor dysfunction | Moderate | I Row 6: EMG/NCS | Normal (CRPS I) vs Abnormal (CRPS II) | Differentiates types | All Color coded rows alternating light grey/white, bold headers, professional medical table style, 1200x900 resolution
Diagram 1 - Pathophysiology & Three-Stage Progression
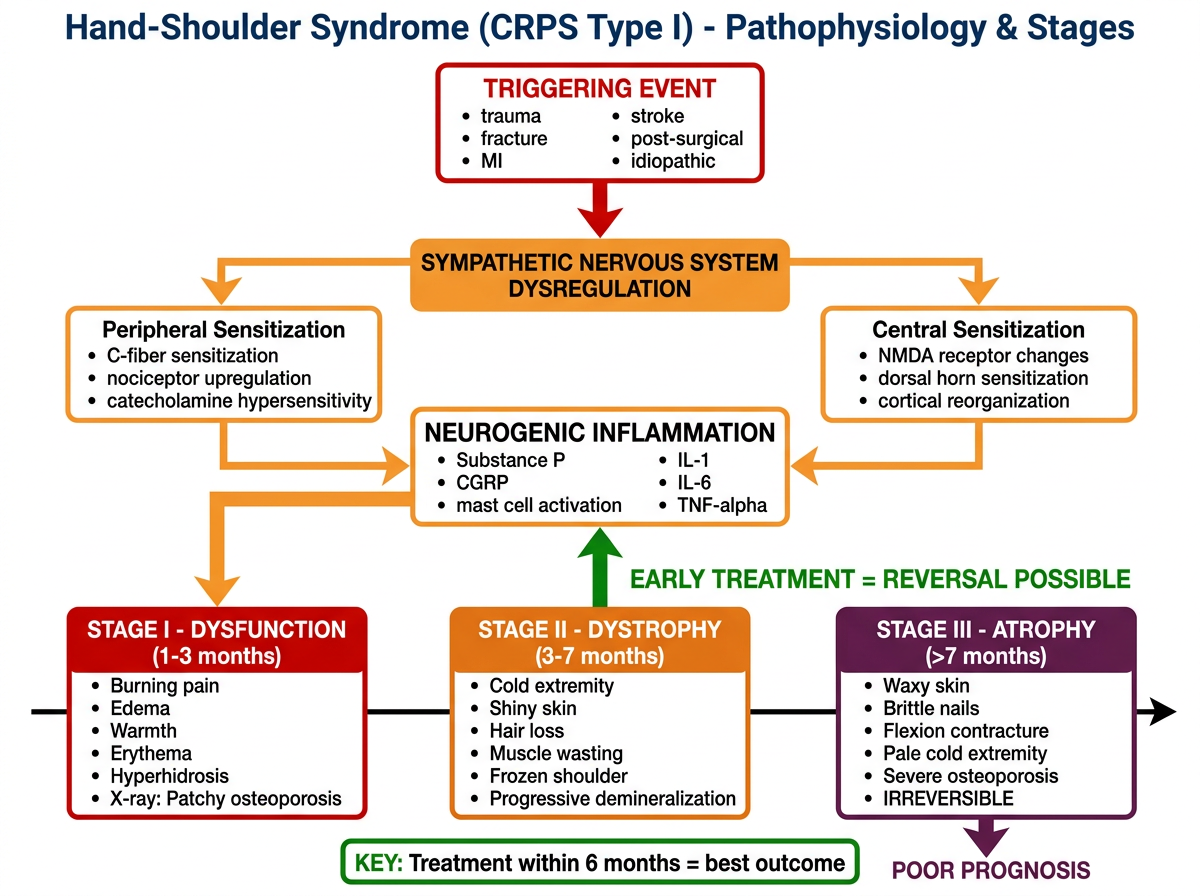
Diagram 2 - Management Algorithm (Complete Treatment Flowchart)
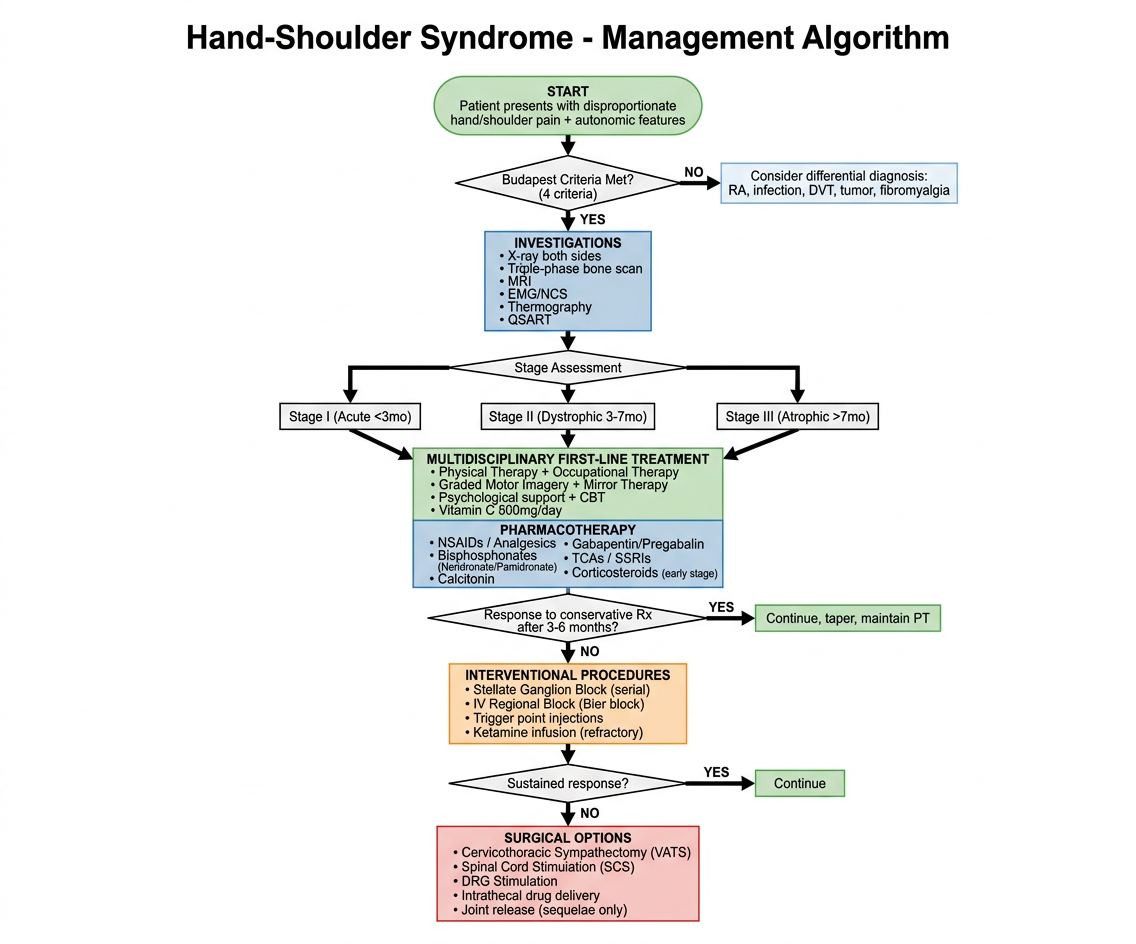
Diagram 3 - Anatomical Basis & Vicious Cycle Mechanism
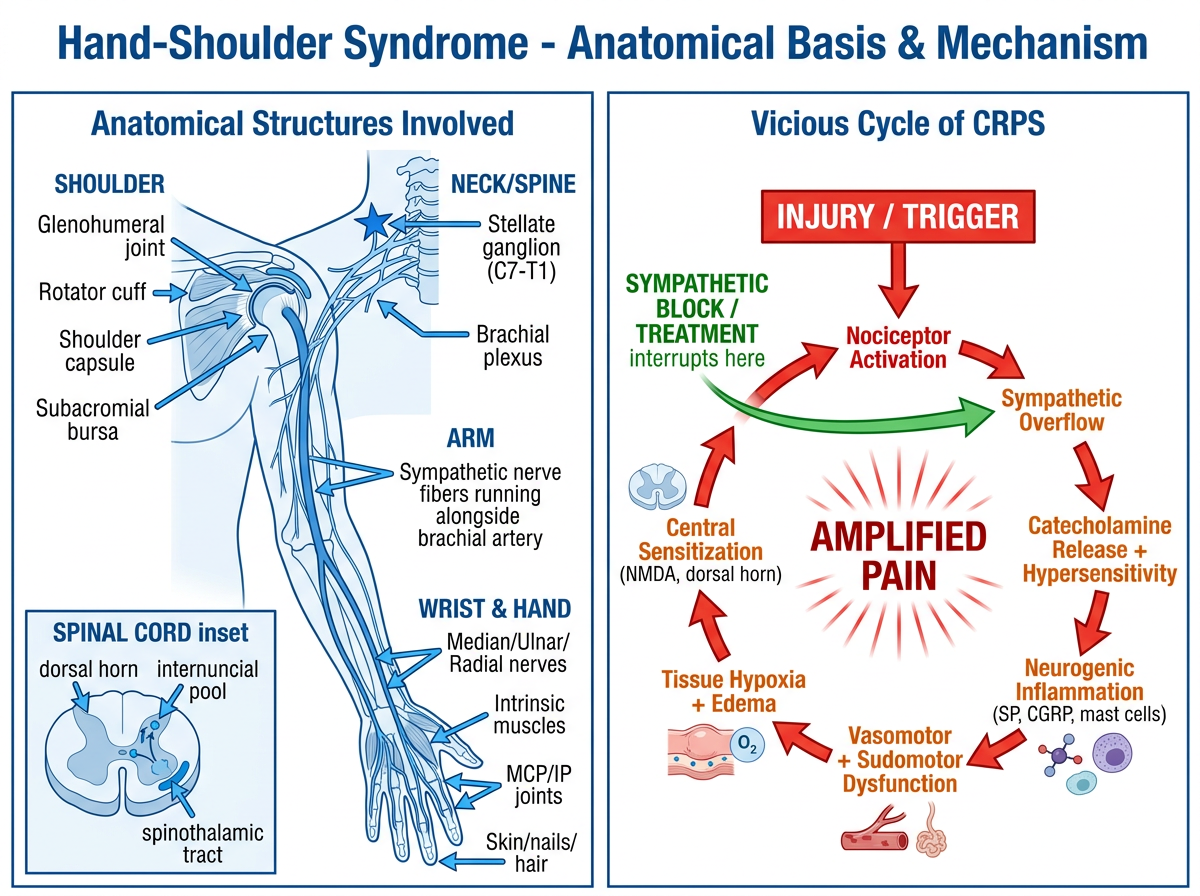
Diagram 4 - Budapest Criteria & Investigations Summary
| Diagnosis | Budapest criteria: symptoms ≥3 domains + signs ≥2 domains |
| Best early investigation | Triple-phase bone scan |
| Critical intervention window | <6 months from onset |
| First-line Rx | PT + Mirror therapy + Bisphosphonates + Stellate Ganglion Block |
| Surgical escalation | VATS sympathectomy → SCS → DRG stimulation |
| Break the cycle | Sympathetic block interrupts the vicious cycle at the autonomic overflow step |