Addiomiq crisis
Reading File
Finding Sources
Searching PubMed
"adrenal crisis" AND management
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of Addisonian Crisis (Acute Adrenal Insufficiency):
Addisonian Crisis (Acute Adrenal Insufficiency)
Definition
An Addisonian crisis is a life-threatening medical emergency caused by critically insufficient cortisol levels. It typically occurs in patients with pre-existing adrenal insufficiency who are exposed to an acute physiological stressor, or from sudden, complete destruction of adrenal function. - Tintinalli's Emergency Medicine, p. 230; Sabiston Textbook of Surgery
Causes & Precipitants
-
Underlying primary adrenal insufficiency (Addison's disease) unmasked by stress
-
Secondary/tertiary adrenal insufficiency (pituitary/hypothalamic disease)
-
Waterhouse-Friderichsen syndrome - bilateral adrenal hemorrhage from severe sepsis (classically meningococcal)
-
Sudden cessation of chronic glucocorticoid therapy
-
Acute stressors in patients with marginal adrenal reserve:
- Infection (most common; especially GI infections)
- Surgery or trauma
- Extreme physical activity
- Acute burns
-
Hypercoagulable states causing adrenal infarction
-
Bailey and Love's Surgery 28e; Tintinalli's Emergency Medicine
Clinical Features
Symptoms are non-specific, making diagnosis challenging. Classic features include:
| Feature | Details |
|---|---|
| Hypotension | Severe, refractory to vasopressors - hallmark sign |
| Abdominal pain | Severe; mimics acute abdomen (commonly misdiagnosed as surgical emergency) |
| GI symptoms | Nausea, vomiting, diarrhea |
| Fever | Common; may suggest underlying infection as precipitant |
| CNS changes | Confusion, disorientation, lethargy, coma |
| Hypoglycemia | Due to cortisol deficiency |
| Electrolyte disturbance | Hyponatremia + hyperkalemia (primary); variable in secondary |
Primary vs. Secondary: Key Differences
| Feature | Primary (Addison's) | Secondary (Pituitary) |
|---|---|---|
| Volume depletion | Marked | Less severe |
| Serum K+ | Hyperkalemia | Hypokalemia |
| Skin pigmentation | Present (high ACTH) | Absent |
| Aldosterone | Deficient | Present |
| ACTH | High | Low/normal |
- Tintinalli's Emergency Medicine, Table 230-3
Diagnosis
Do not delay treatment while awaiting results.
Initial labs:
- Serum cortisol, plasma ACTH
- Electrolytes (Na+, K+, Ca2+), glucose, CBC
- Plasma renin, aldosterone
- ECG (potassium-related changes)
Key thresholds:
- Morning serum cortisol >18 mcg/dL - effectively rules out adrenal insufficiency
- Morning serum cortisol <15 mcg/dL (or salivary <5.8 ng/mL) - adrenal insufficiency possible
Confirmatory test - ACTH Stimulation (Synacthen/Cosyntropin Test):
- Give 250 mcg cosyntropin IV
- Measure cortisol at baseline and 30-60 min post
- Post-cortisol <18 mcg/dL = strongly suggestive of adrenal insufficiency
- Note: If steroids must be given urgently before the test, use dexamethasone (no cross-reactivity with cortisol assays)
Algorithm:
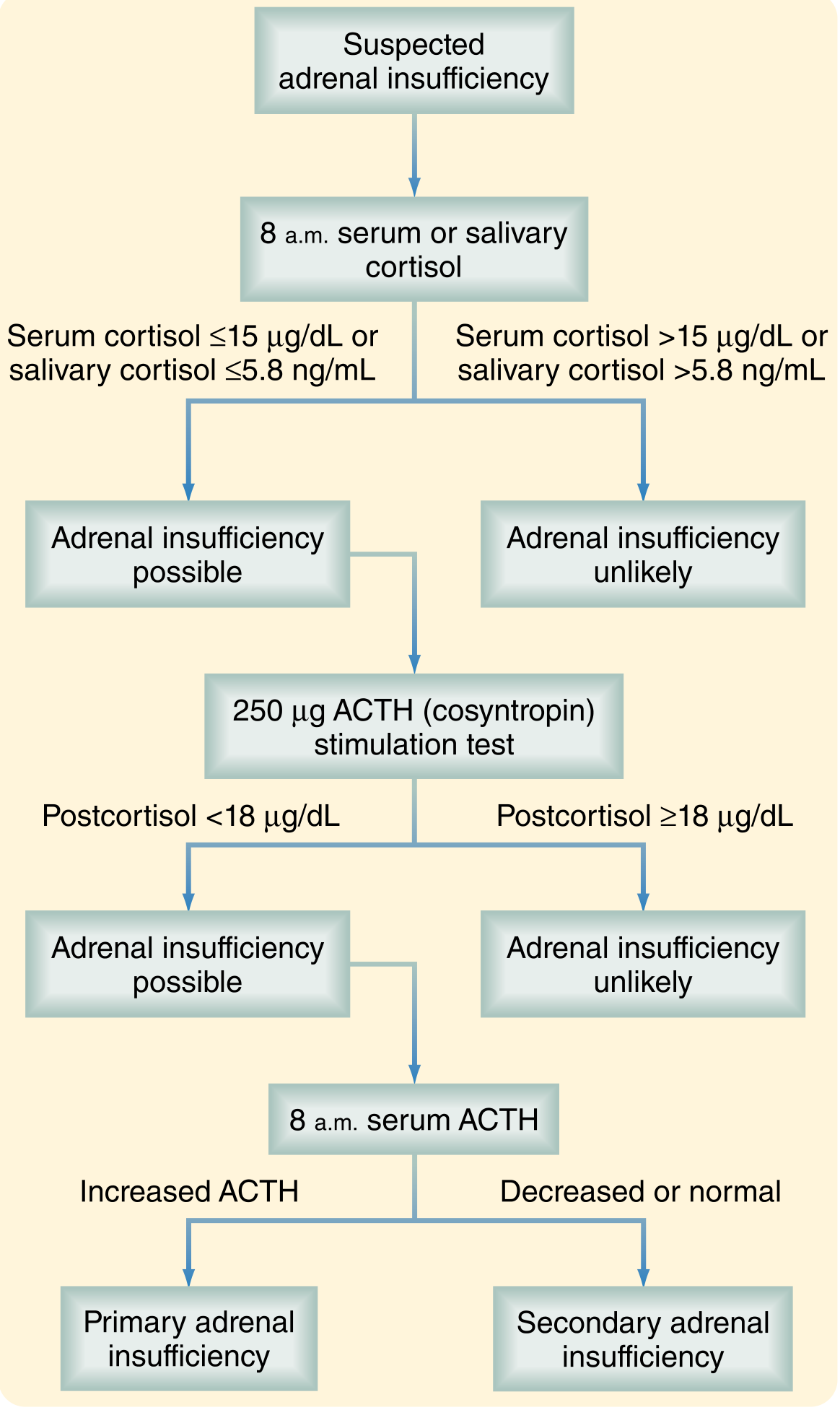
- Sabiston Textbook of Surgery, Fig. 75.7
Treatment (Emergency Protocol)
Treatment must start IMMEDIATELY - do not wait for lab results. - Bailey and Love's Surgery 28e
1. IV Fluids
- Normal saline (0.9%): 2-3 L in the first 6 hours
- Use D5/NS (dextrose-saline) if hypoglycemic
2. Steroids (Drug of Choice: Hydrocortisone)
- Hydrocortisone 100 mg IV bolus (first-line - provides both glucocorticoid AND mineralocorticoid effects)
- Followed by 50 mg IV q6h (or 200 mg/24h infusion)
- If no IV access: 100 mg IM
- Alternative: Dexamethasone 4 mg IV (preferred if ACTH stimulation test is planned - no cortisol cross-reactivity); must add fludrocortisone 100 mcg/day as dexamethasone has no mineralocorticoid activity
3. Supportive Care
- Airway, breathing, circulation
- Correct electrolytes (Na+, K+, Ca2+)
- Treat underlying precipitant (antibiotics for infection)
4. Vasopressors (if needed)
- Only after steroid therapy, in patients unresponsive to fluids
- Norepinephrine, dopamine, or phenylephrine
5. Mineralocorticoid Replacement (NOT urgent initially)
-
Fludrocortisone effects take days to manifest; saline infusion covers early needs
-
Begin once patient is stabilized and tolerating oral medications
-
Tintinalli's Emergency Medicine, Table 230-4; Bailey and Love's Surgery 28e; Sabiston Textbook of Surgery
Prevention / Patient Education
Patients with known chronic adrenal insufficiency must:
-
Take lifelong glucocorticoid replacement (hydrocortisone 15-25 mg/day PO in 2-3 divided doses)
-
Double the dose during illness or stress ("sick day rules")
-
Take fludrocortisone 0.05-0.2 mg each morning (for primary insufficiency)
-
Carry a steroid emergency card and injectable hydrocortisone for self-injection
-
Bailey and Love's Surgery 28e
Recent Evidence Note
A 2025 systematic review and meta-analysis (PMID: 40966723) confirmed increased all-cause mortality in primary adrenal insufficiency, underscoring the importance of early recognition and aggressive treatment of adrenal crisis.
This is a shared conversation. Sign in to Orris to start your own chat.