Skin grafting indications Contraindications Steps And Stages of Grafts accept
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, well-structured answer.
Skin Grafting: Complete Overview
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Sabiston Textbook of Surgery, Fischer's Mastery of Surgery 8th ed, Pfenninger & Fowler's Procedures for Primary Care, Current Surgical Therapy 14e, Rockwood & Green's Fractures in Adults, Bailey & Love's Short Practice of Surgery 28th ed
Definition
A skin graft is tissue moved from one site (donor site) to another (recipient site) without its own blood supply. It is entirely dependent on the recipient bed for revascularization and survival. Grafts are classified based on the layers of skin harvested.
Types of Skin Grafts
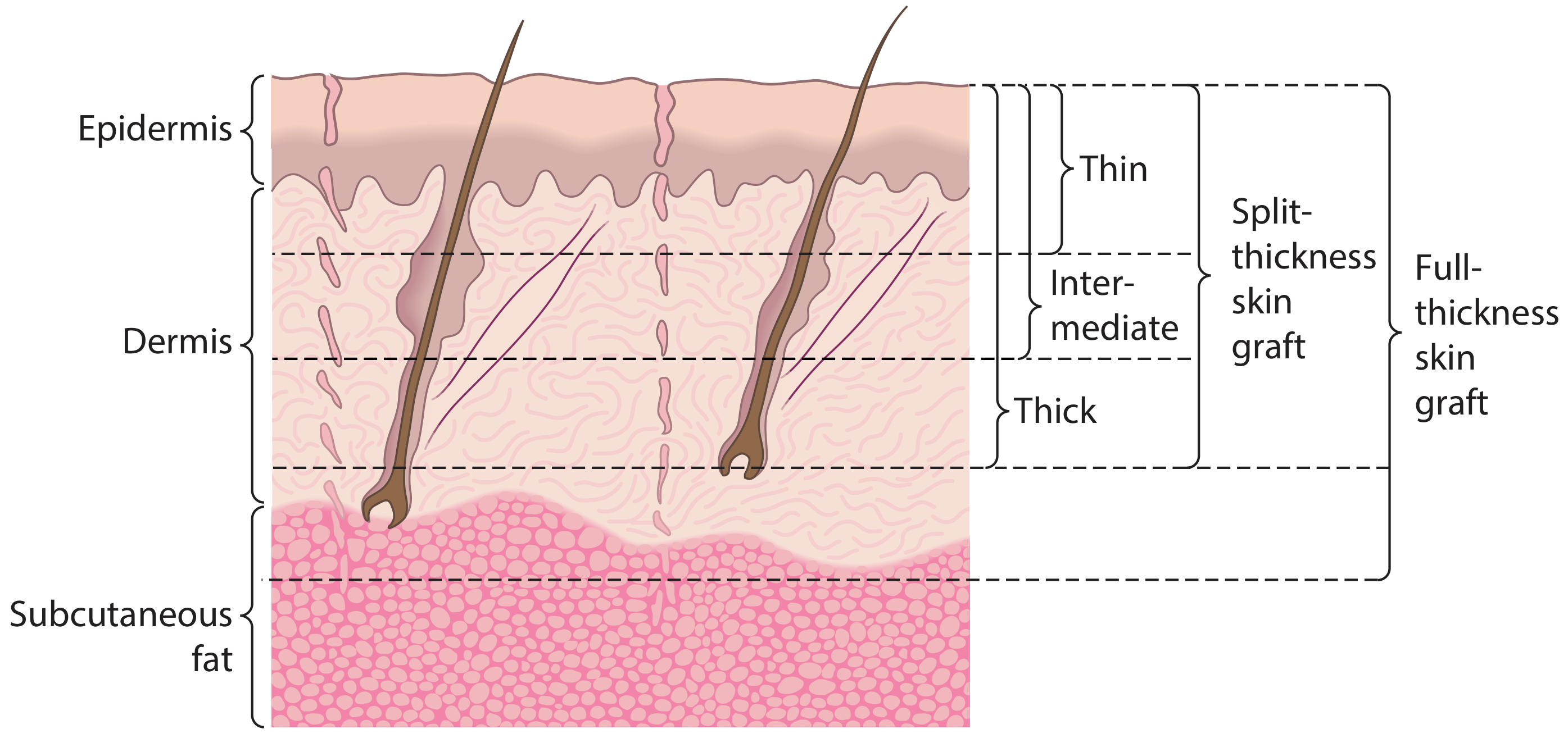
Figure: Skin graft thickness levels - Scott-Brown's Otorhinolaryngology
| Type | Layers Included | Thickness |
|---|---|---|
| Split-thickness (STSG) | Epidermis + part of dermis | Thin (0.005-0.010 in), Medium, Thick (0.015 in) |
| Full-thickness (FTSG) | Epidermis + entire dermis | Determined by donor region |
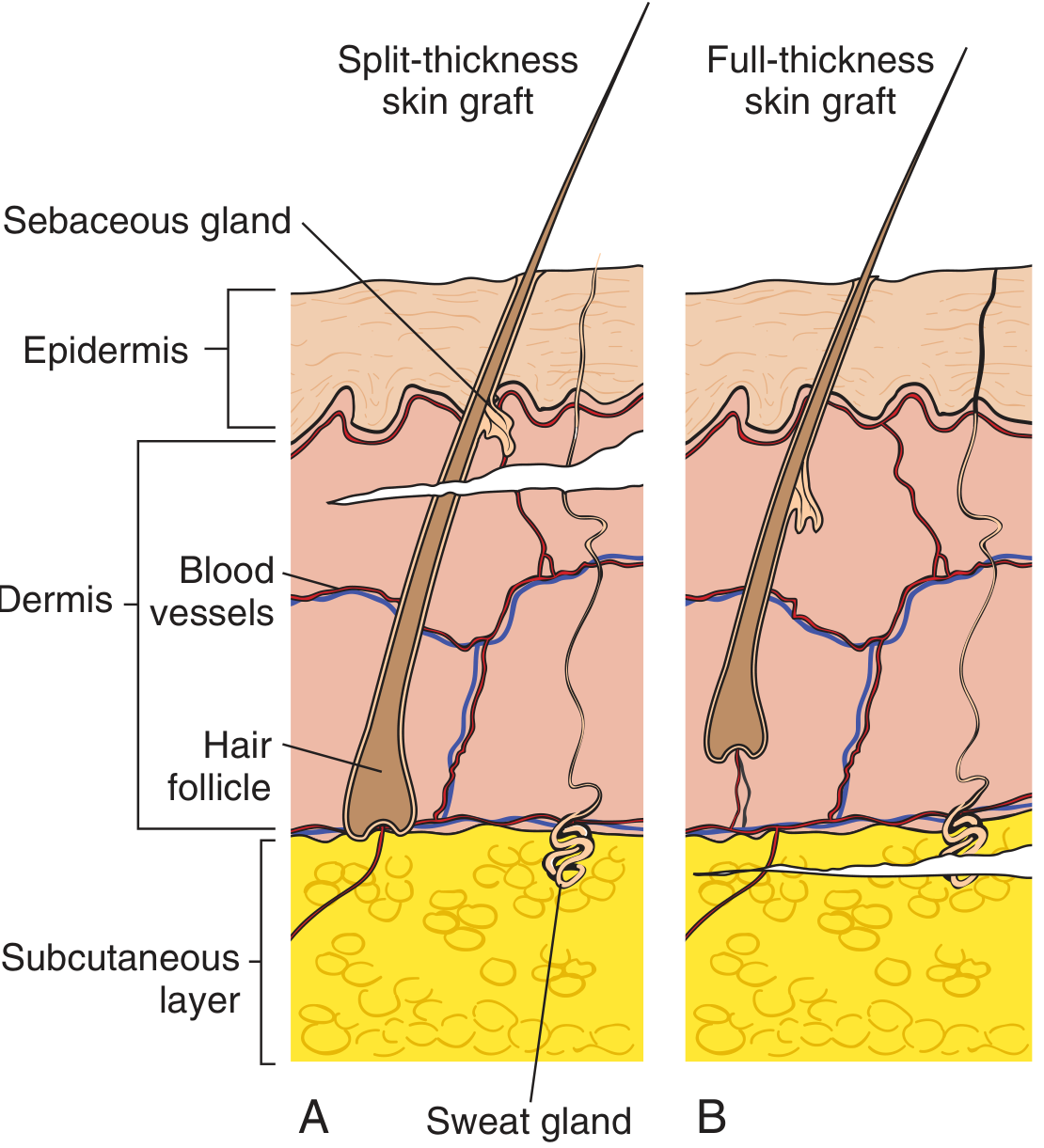
Figure: STSG vs FTSG cross-section anatomy - Pfenninger & Fowler's Procedures for Primary Care
Indications
1. Wound Coverage (Most Common)
- Burns (deep partial-thickness and full-thickness burns) - early excision and grafting reduces infection risk and healing time
- Traumatic wounds with skin loss too large for primary closure or secondary intention healing
- Chronic non-healing ulcers (venous, diabetic, pressure ulcers) after adequate debridement
2. Reconstructive Indications
- Skin defects after tumor excision (e.g., basal cell carcinoma, squamous cell carcinoma, melanoma) - particularly when the defect is too large to close primarily but not large enough to warrant a free flap
- Reconstruction after mastectomy or other cancer resections
- Soft tissue defects over periosteum, fascia, or muscle that cannot be closed primarily
- Orbital exenteration defects (where a prosthesis will be placed)
- Maxillectomy defects (with palatal obturators)
- Flap donor site closure (e.g., radial forearm flap or fibula flap harvest sites)
- Granulating wounds as a delayed second-stage closure after initial healing
3. Specific Clinical Situations
- Patients medically unfit for prolonged anesthesia required for free flap reconstruction
- Pediatric burns - scalp is an excellent donor site
- Areas requiring coverage after contracture release
- Coverage of exposed healthy periosteum or perichondrium (e.g., upper two-thirds of nose using FTSG)
- Patients requiring staged reconstruction where the wound is first granulated, then grafted
Contraindications
Absolute Contraindications (Recipient Site)
- Exposed avascular bone without periosteum - no vascular bed to support graft
- Exposed tendon without paratenon
- Exposed cartilage
- Heavily irradiated tissue (poor vascularity)
- Active infection or heavy bacterial colonization - wounds containing >10⁵ organisms per gram of tissue will not support a graft; specific organisms that destroy fibrin and prevent adherence include:
- Streptococcus pyogenes (beta-hemolytic streptococci are particularly destructive)
- Pseudomonas aeruginosa
- MRSA
Relative Contraindications / Unfavorable Conditions
- Fat as recipient bed - less vascular than muscle/fascia, poor take
- Exposed peritoneum or major blood vessels - risk of compromise if graft fails
- Systemically unfit patients with coagulopathy (high hematoma risk)
- Active malignancy in wound bed - graft will not address underlying disease
Systemic Factors That Impair Graft Take
- Diabetes mellitus
- Smoking
- Prior radiotherapy or chemotherapy to the area
- Malnutrition / poor nutritional status
Steps of Skin Grafting
Pre-operative
- Assess and prepare the recipient site - complete debridement of necrotic tissue, control of infection, and achievement of a viable wound bed (granulation tissue, healthy muscle, or fascia)
- Donor site selection - choose a cosmetically concealed area; options include inner thigh (most common), scalp (excellent for large burns - heals with no alopecia), back, buttock
- Mark both sites - measure the defect, mark the donor site area accordingly
- Patient counseling - donor site will create an additional permanent scar
Intraoperative
A. Harvesting the Graft (STSG)
- Infiltrate donor site subcutaneously with physiologic saline to create a flat harvestable surface
- Apply mineral oil to the skin surface to lubricate
- Assistant holds skin taut with gauze or towel clamp
- Set electric/air-powered dermatome to 0.2-0.3 mm (0.008-0.012 inches) - set between 6/1000 and 12/1000 inch; verify the gap manually with a #15 blade
- Hold dermatome at 45-60 degrees to the skin surface; activate before skin contact
- Advance with consistent, gentle pressure and forward motion across the width of the blade
- After harvest: donor site should show light punctate bleeding (papillary dermis level) - fat lobules must NOT be visible
- Hemostasis at donor site: epinephrine-soaked gauze (1:10,000 to 1:20,000)
B. Processing the Graft
- Pie-crusting: make small perforations with a #15 blade or needle to prevent hematoma collection
- Meshing: pass through a mesh carrier for large defects - ratios of 1:1.5, 1:2, 1:3, 1:6, or 1:9; meshing promotes drainage and allows expansion to cover larger areas; standard of care for large burns
- Avoid meshing on aesthetically important areas (face, hands) as mesh pattern becomes visible scarring
C. Applying the Graft
- Achieve meticulous hemostasis of recipient bed
- Apply graft dermis side down onto the wound bed
- Place under mild tension - attach one edge, pull/stretch toward opposite edge; trim to fit with an ideal 1-2 mm gap from wound edge to graft
- Graft must contact the wound bed completely
- Orient graft seams perpendicular to biodynamic skin tension lines, respecting aesthetic units
- Fix with staples, non-absorbable sutures (Prolene - especially hands and face), thrombin/cyanoacrylate glue; absorbable sutures are avoided as they cause inflammatory granulomas
D. Dressing
- Apply a non-adherent (low-adherent) dressing (e.g., Adaptic, Jelonet) directly on the graft
- Apply a bolster or tie-over dressing, or negative pressure wound therapy (NPWT/VAC) to:
- Eliminate dead space
- Prevent shear forces
- Promote graft-bed contact
- Immobilize the area for 3-7 days (critical phase of revascularization)
Postoperative
- First dressing change at 3-5 days (after initial adherence)
- Monitor for hematoma, seroma, infection
- Ongoing immobilization until graft is secure
- Compression garments for burn scar management after full healing
Stages of Graft Acceptance ("Take")
Once a graft is harvested and placed, it passes through four sequential biological stages to achieve permanent survival:
Stage 1 - Graft Adherence (Immediate)
| Mechanism | Fibrin layer forms between graft undersurface and recipient bed |
|---|
- The graft adheres immediately through a thin fibrin layer
- Within 48 hours, fibrin begins breaking down; adhesion is then maintained by fibroblast proliferation and collagen deposition
- No blood flow to the graft yet; graft appears pale
Stage 2 - Serum Imbibition (0 to 48 hours)
| Mechanism | Passive absorption of plasma nutrients from the recipient bed |
|---|
- The graft survives by absorbing nutrients from plasma leaking out of capillaries in the recipient bed
- The graft gains weight and swells during this phase
- This is entirely passive diffusion - the graft has NO active circulation
- This phase is transient; the graft cannot survive on imbibition indefinitely
Stage 3 - Revascularization (48 hours to 3 weeks)
This occurs through three overlapping mechanisms:
| Mechanism | Description |
|---|---|
| Inosculation | Direct joining of cut vessel ends in the recipient bed with cut vessel ends in the graft - the graft's own vessels reconnect to the bed's vessels |
| Revascularization | Actual ingrowth of new vessels from the recipient bed into the graft, forming new vascular channels |
| Neovascularization | Endothelium of old cut vessels degenerates, leaving basement membrane as a conduit for capillary bud ingrowth |
- Graft begins to appear pink/red as circulation is restored
- This is the most critical phase; shear forces and fluid collections (hematoma/seroma) during this phase = graft failure
- Complete by approximately 3 weeks
Stage 4 - Remodelling (3 weeks to 1 year)
| Mechanism | Maturation and reorganization of collagen; increasing tensile strength |
|---|
- Collagen reorganization, increasing graft strength and durability
- Pigmentation normalizes (partially)
- Sensory recovery occurs (better in FTSG than STSG)
- Secondary contraction occurs (myofibroblast activity in wound bed) - more pronounced in STSG
Summary Table: STSG vs FTSG
| Feature | STSG | FTSG |
|---|---|---|
| Dermis included | Partial | Full |
| Donor site heals by | Re-epithelialization from adnexal remnants | Direct closure (scar) |
| Recipient bed vascularity needed | Less | More |
| Primary contraction | Less | More (due to elastin) |
| Secondary contraction | More | Less |
| Pigmentation | Abnormal, mismatched | Better match |
| Cosmetic result | Poorer | Superior |
| Sensory recovery | Poorer | Better |
| Hair growth | Absent (no follicles) | Present |
| Best use | Large defects, burns | Small cosmetically important areas (face, hands) |
| Max reliable size | Large (can be meshed) | ~2.5 cm without unpredictable take |
Causes of Graft Failure (Summary)
- Hematoma or seroma (most common) - separates graft from bed, blocks revascularization
- Infection (>10⁵ organisms/gram) - destroys fibrin, prevents adherence
- Shear forces - disrupt forming vascular connections
- Poor recipient bed - exposed bone, tendon, irradiated tissue
- Systemic factors - diabetes, smoking, poor nutrition, steroids
This is a shared conversation. Sign in to Orris to start your own chat.