Extended trochanteric osteotomy in orthopaedics 10 marks pg answer with flow chart and images
extended trochanteric osteotomy orthopedics technique indications complications
https://www.wheelessonline.com/orthopaedics/extended-trochan…
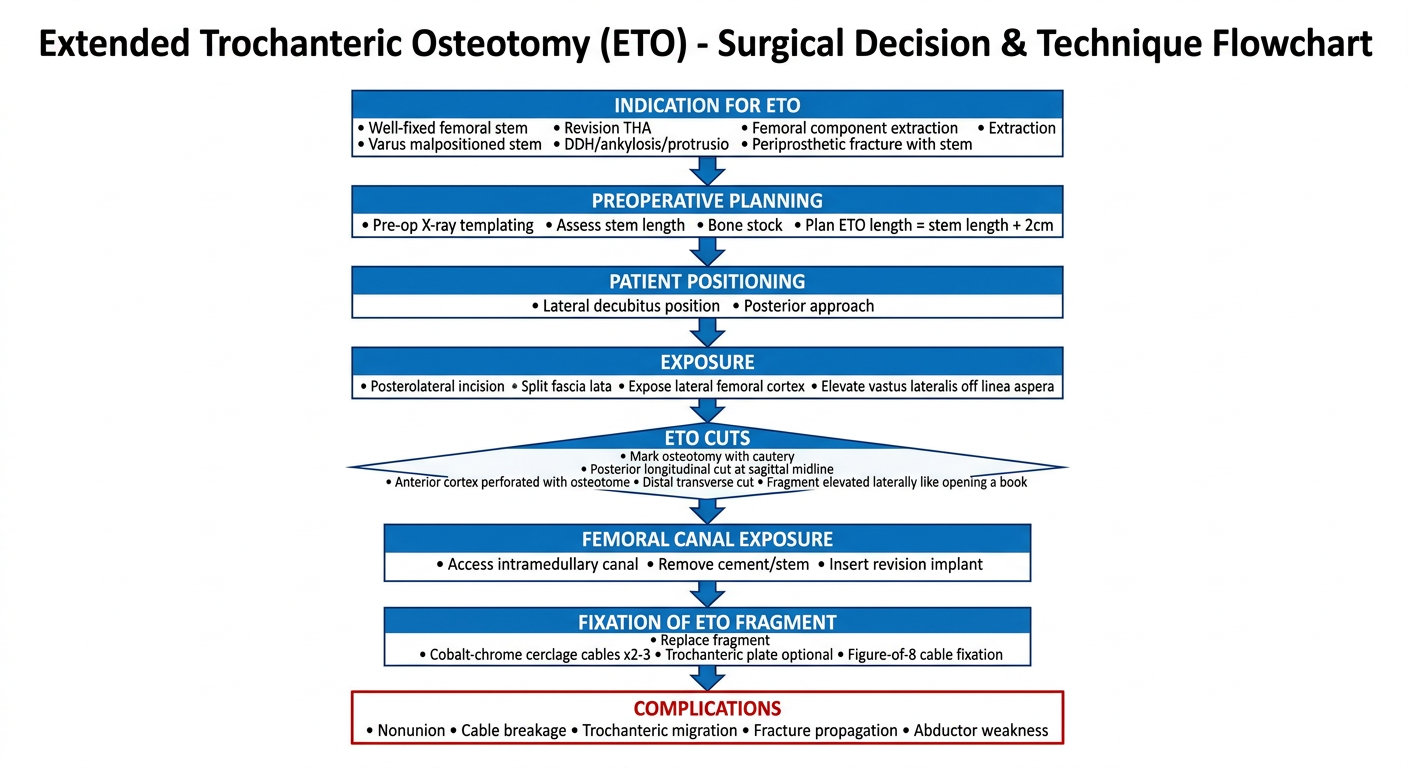
A clean medical flowchart titled "Extended Trochanteric Osteotomy (ETO) - Surgical Decision & Technique Flowchart". The flowchart should flow top to bottom with the following nodes connected by arrows: 1. "INDICATION FOR ETO" box at top (with sub-bullets: Well-fixed femoral stem, Varus malpositioned stem, Revision THA, Femoral component extraction, DDH/ankylosis/protrusio, Periprosthetic fracture with stem). Arrow down to 2. "PREOPERATIVE PLANNING" box (Pre-op X-ray templating, Assess stem length, Bone stock, Plan ETO length = stem length + 2cm). Arrow down to 3. "PATIENT POSITIONING" (Lateral decubitus position, Posterior approach). Arrow down to 4. "EXPOSURE" (Posterolateral incision, Split fascia lata, Expose lateral femoral cortex, Elevate vastus lateralis off linea aspera). Arrow down to 5. "ETO CUTS" diamond shape (Mark osteotomy with cautery, Posterior longitudinal cut at sagittal midline, Anterior cortex perforated with osteotome, Distal transverse cut, Fragment elevated laterally like opening a book). Arrow down to 6. "FEMORAL CANAL EXPOSURE" (Access intramedullary canal, Remove cement/stem, Insert revision implant). Arrow down to 7. "FIXATION OF ETO FRAGMENT" (Replace fragment, Cobalt-chrome cerclage cables x2-3, Trochanteric plate optional, Figure-of-8 cable fixation). Arrow down to 8. "COMPLICATIONS" box in red (Nonunion, Cable breakage, Trochanteric migration, Fracture propagation, Abductor weakness). The design should use blue and white colors with clear readable Arial font on a white background, professional medical illustration style.
Extended Trochanteric Osteotomy (ETO)
10-Mark Answer | Campbell's Operative Orthopaedics, 15th Ed. 2026
Definition
Types of Trochanteric Osteotomy
| Type | Feature | Indication |
|---|---|---|
| Standard/Conventional | Osteotomy at base of trochanter only | Complex acetabular revision, protrusio cage |
| Trochanteric Slide | Sagittal-plane cut, includes vastus lateralis origin | Direct lateral approach revisions |
| Extended (ETO) | Greater trochanter + lateral femoral cortex raised en bloc | Well-fixed stems, varus malposition, revision THA |
- Campbell's Operative Orthopaedics, 15th Ed. p.279-280
Indications for ETO
- Removal of well-fixed, fully coated press-fit cementless femoral stems (primary indication)
- Revision of femoral stems placed in significant varus
- Revision THA - to facilitate exposure of femur and acetabulum
- Periprosthetic femoral fractures around a well-fixed stem
- Complex primary THA - ankylosis/hip fusion, severe protrusio acetabuli, high dislocation in DDH
- When the bony bed for a standard osteotomy would be compromised (e.g., trochanter filled with cement)
- To allow distal advancement of abductors when residual laxity causes hip instability
Key rule: ETO is used only when a cementless femoral reconstruction is anticipated, because a large segment of lateral cortex is removed, rendering cementing techniques imperfect.
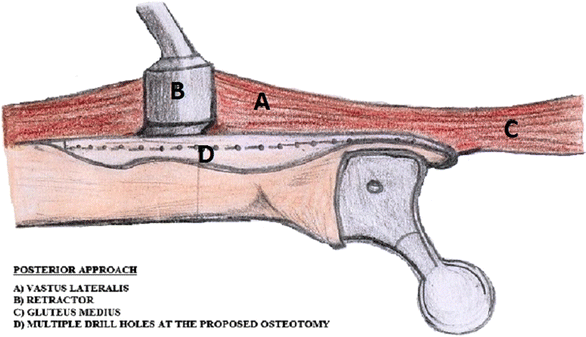
Surgical Technique (Posterior Approach)
- Patient in lateral decubitus position
- Posterior approach via posterolateral incision centered over greater trochanter
- Split fascia lata; expose lateral femoral cortex
- Elevate the vastus lateralis off the linea aspera (laterally), exposing the lateral femoral shaft
- Caution: If a previous anterolateral approach was made, elevating the lateralis off the linea aspera may devascularize it, causing catastrophic muscle necrosis
- Mark the lines of the osteotomy with electrocautery
- Fragment length = length of femoral stem + approximately 2 cm distally (typically 10-15 cm from GT tip)
- Posterior longitudinal cut: close to the sagittal midline of the femur (posterior to the mid-lateral line)
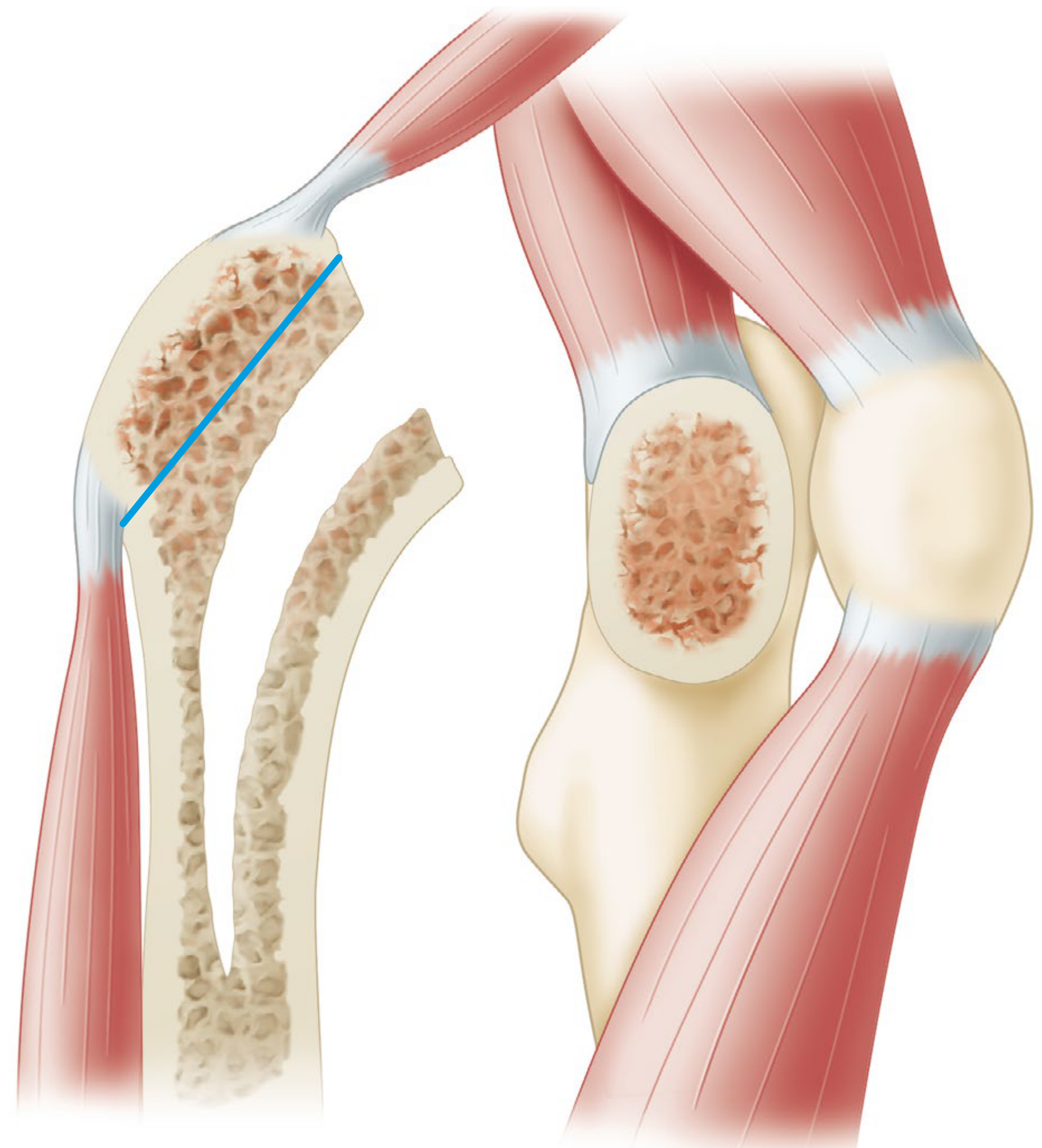
- Anterior cut: avoid stripping the vastus lateralis; instead, use a small osteotome to perforate the anterior femoral cortex through the vastus lateralis
- Distal transverse cut: completed with a Gigli saw or oscillating saw
- The osteotomy fragment is completed by inserting the osteotome underneath the trochanter and applying a prying (book-opening) motion
- ETO fragment is reflected laterally, exposing the intramedullary canal
- Cement, well-fixed stem, or membrane can be removed under direct vision
- New revision femoral component is inserted
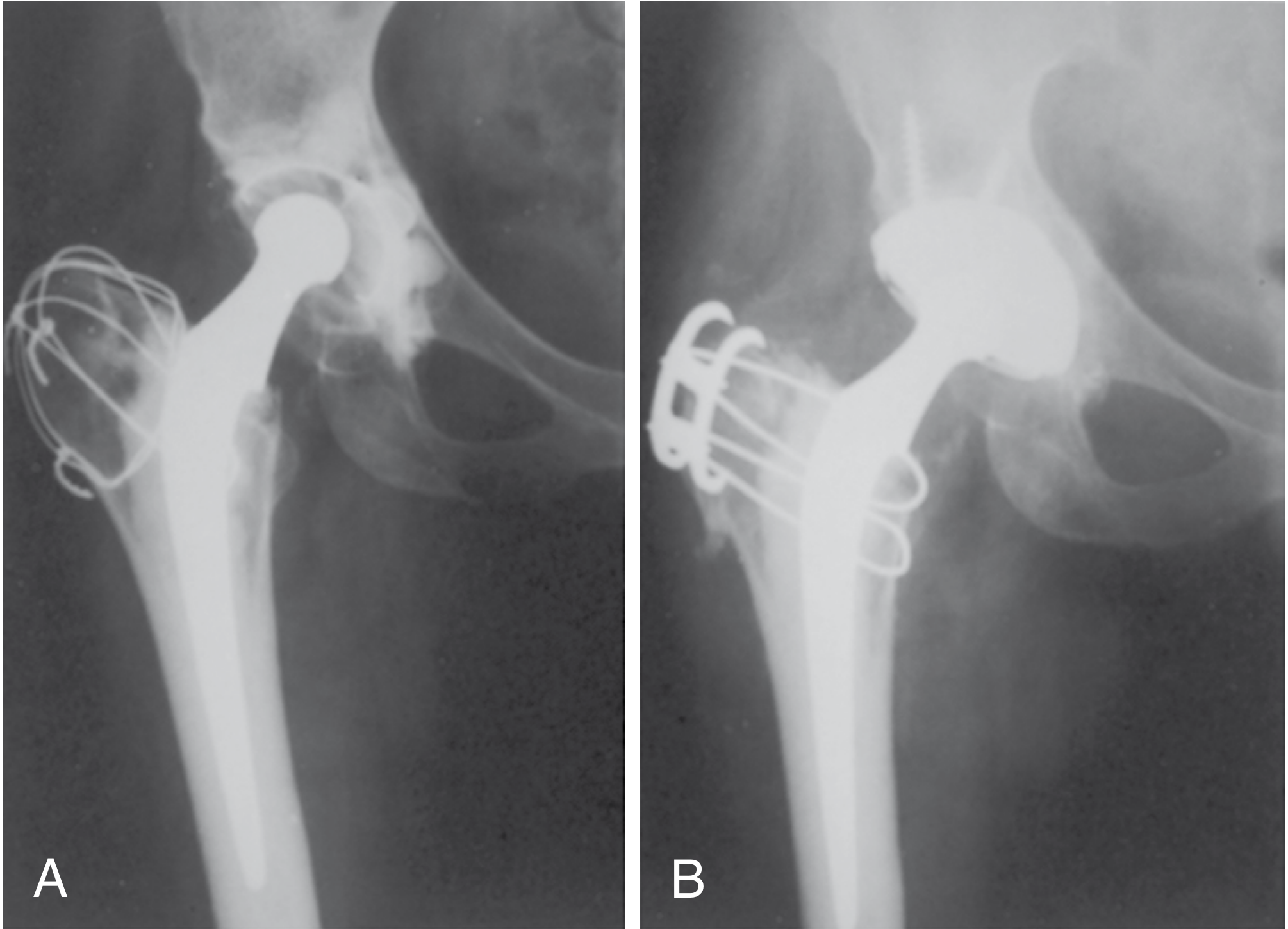
Fixation of the ETO Fragment
- ETO fragment is reduced back and secured with cobalt-chrome cerclage cables (2-3 cables; NOT stainless steel - less risk of fretting corrosion)
- Cable fixation technique:
- Horizontal cable passed under the vastus lateralis
- Vertical cable in a figure-of-eight pattern in two planes
- Distal cerclage cable just distal to the lesser trochanter
- Anterior cable passed through an oblique drill hole in the greater trochanter
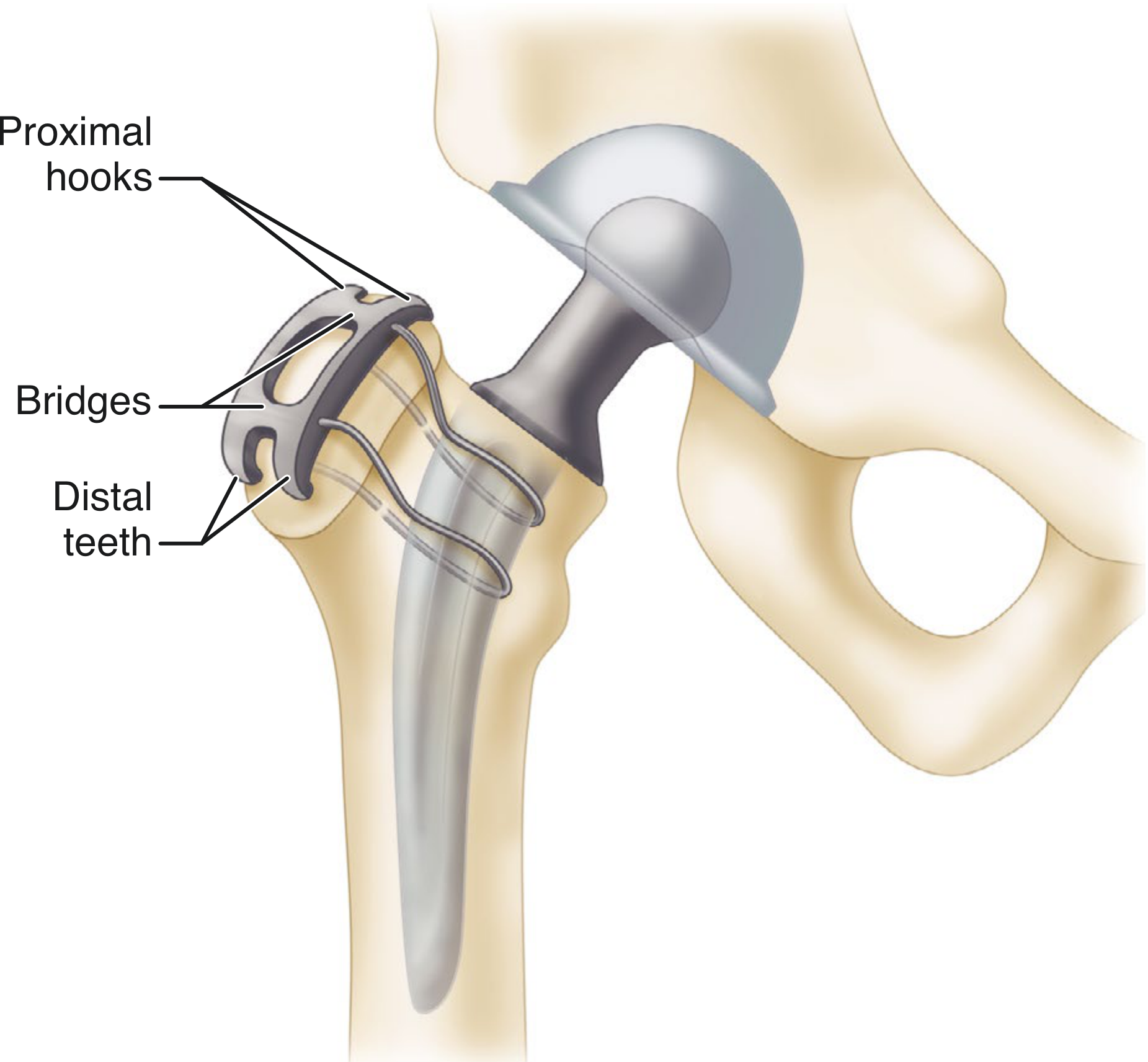
- Trochanteric plate options: Accord plate or similar devices with proximal hooks + plate extension fixed to femur with cerclage cables (Fig. 4.77)
- Some revision components allow a trochanteric plate to bolt directly into the femoral component
Keys to Achieving Union
- Anatomic reduction OR slight distal overlap of the trochanter leads to union within 6 months
- Residual superior and medial tilt leads invariably to delayed union or nonunion
- Compression must be applied across the osteotomy
- Hip should NOT be abducted more than 10-15 degrees during reattachment, or fixation strain and avulsion may follow
- A biplanar/chevron osteotomy offers greater resistance to anteroposterior displacement than uniplanar
Lakstein Modification (Modified ETO)
- The posterior capsule and short external rotators are left intact to reduce the risk of postoperative dislocation
- Particularly useful in revision surgery where instability is a concern
Flowchart
Postoperative Management
| Phase | Protocol |
|---|---|
| Immediate | Partial weight bearing with walker |
| 6 weeks | Protected weight bearing until radiographic union |
| Full weight bearing | Delayed until trochanteric union confirmed on X-ray (usually 3-6 months) |
| Physiotherapy | Abductor strengthening program; avoid active hip abduction until union |
Advantages of ETO
- Excellent direct visualization of the intramedullary canal
- Protects surrounding soft tissues during extraction
- Avoids iatrogenic femoral shaft fracture during stem removal
- Allows controlled, predictable access to well-fixed implants
- Fragment heals with biological bone-to-bone union (reliable if fixed correctly)
- Allows distal advancement of abductors to improve abductor function
Complications
| Complication | Details |
|---|---|
| Nonunion | Most serious complication; 25% reported with wire techniques; reduced with cable systems |
| Trochanteric migration | Fragment displaces proximally; causes abductor weakness, Trendelenburg gait |
| Cable/wire breakage | Fatigue failure of fixation hardware |
| Persistent limp | Abductor weakness from migration or nonunion |
| Fracture propagation | Osteotomy may extend distally if cuts inadequate |
| Increased blood loss | More than standard approaches |
| Delayed rehabilitation | Due to restricted weight-bearing |
| Bursitis | From prominent hardware |
| Nerve injury | Sciatic nerve at risk during posterior cuts |
Summary Points for Exam
-
ETO = greater trochanter + lateral femoral cortex raised en bloc
-
Used only with cementless femoral reconstruction
-
Length = stem length + 2 cm
-
Fragment fixed with cobalt-chrome cables (not stainless)
-
Anatomic or slightly distal reduction gives best union
-
Lakstein modification preserves posterior capsule to reduce dislocation risk
-
Nonunion is the most feared complication
-
Campbell's Operative Orthopaedics, 15th Ed. 2026, pp. 278-281
-