Give me notes on physiology of phonation according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for comprehensive notes. Here are the complete, well-organized notes on the physiology of phonation compiled from three standard ENT textbooks.
Physiology of Phonation
Sources: Cummings Otolaryngology Head and Neck Surgery; KJ Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
1. Definition
Phonation is a laryngeal motor behaviour used for speech production, involving highly specialized coordination of laryngeal and respiratory neuromuscular control. The larynx acts as a vibrator, activated by exhaled air (the excitor). Adducted vocal folds vibrate passively, powered by exhaled air.
- Scott-Brown's, p. 941
2. Five Requirements for Normal Phonation (Box 53.1, Cummings)
- Adequate breath support
- Approximation of vocal folds
- Favorable vibratory properties
- Favorable vocal fold shape
- Control of length and tension
Additionally, KJ Lee adds:
- Some degree of mucosal pliability for sustained sound
- Adequate vocal fold bulk (the TA-LCA complex may atrophy with aging or neuropathy)
- Resonance of the vocal tract
- Cummings, p. 1023; KJ Lee, p. 916
3. Historical Theories of Phonation
- Neurochronaxic hypothesis (Husson, 1950): Proposed that each vibratory cycle was caused by a separate neural impulse. This is now considered physiologically impossible and has been discarded.
- Myoelastic-aerodynamic theory (van den Berg, 1950s): Now the widely accepted theory. States that the interaction of aerodynamic forces and the mechanical properties of laryngeal tissues is responsible for inducing vocal fold vibration and generating vocal sound.
- Cummings, p. 1023
4. Mechanism of Phonation (Step by Step)
Initiation
- Pre-phonatory inspiratory phase (Wyke): Just before phonation, vocal folds rapidly abduct to allow air intake.
- The vocal folds are then adducted by contraction of the lateral cricoarytenoid muscles, positioning them near the midline.
- Subglottic pressure builds below the adducted vocal folds during expiration until it overcomes their resistance.
The Vibratory Cycle
- Elevated subglottic pressure blows the vocal folds apart, starting from the inferior margin (they peel apart from below upward).
- A puff of air escapes through the glottis.
- Airflow through the narrowed glottis creates a drop in pressure (Bernoulli effect): "When air passes from one large space to another through a constriction (the glottis), velocity is greatest and pressure is least at the site of the constriction."
- This negative pressure sucks the vocal folds back together, inferior margins closing first.
- Elastic (myoelastic) recoil of the vocal folds also contributes to their return to midline.
- Contact between the folds increases until subglottic pressure again overcomes resistance, and the cycle repeats.
Each cycle = one vibratory oscillation, producing one sound wave. The frequency of this cycle determines the fundamental frequency (pitch) of the voice.
- Cummings, p. 1023; Scott-Brown's, p. 945; KJ Lee, p. 916
5. The Vibratory Cycle - Four Phases (Scott-Brown's)
| Phase | Description |
|---|---|
| Closing phase | Vocal folds begin to close rapidly from their lower margin |
| Closed phase | Medial edges are in full contact |
| Opening phase | Folds begin to separate from lower margin; superior margin remains in contact until end of phase |
| Open phase | Vocal folds are separated (longest part of a normal cycle) |
- The closing phase is more rapid than the opening phase.
- Scott-Brown's, p. 945
6. Body-Cover Theory (Hirano's Concept)
Actual phonation is three-dimensional. The vocal fold is not a homogeneous structure, and the vibration of the mucosa does not correspond directly to that of the underlying tissue.
- Body = vocalis muscle (relatively static; provides firm substrate)
- Cover = mucosa (moves as a wave over the body)
The mucosal wave begins on the inferomedial aspect of the vocal fold and moves rostrally (upward). As the superior edges begin to separate, the lower edges are already closing - this is explained by the two-mass model (Ishizaka & Flanagan).
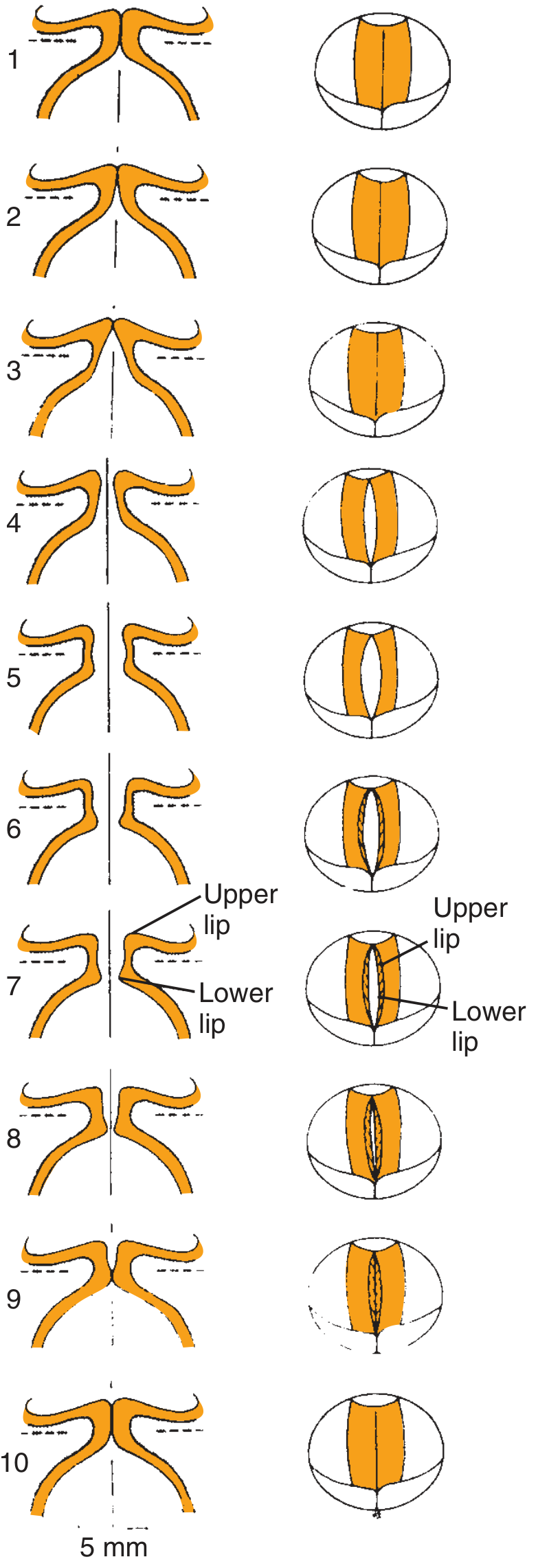
Fig. Movements of different portions of vocal folds during one cycle of vibration: coronal plane (left) and from above (right). Mucosal upheaval begins caudally (1) and moves rostrally. Lower portion closes as upper margin opens (5). (From Hirano M, Clinical examination of voice, 1981)
This mucosal wave can only be visualized using laryngostroboscopy or high-speed photography.
- Cummings, p. 1024; Scott-Brown's, p. 945
7. Histological Layers of the Vocal Fold (Hirano)
The undulating mucosal wave is possible because of a specialized layered connective tissue separating mucosa from the vocalis muscle:
| Layer | Composition |
|---|---|
| Superficial (Reinke's space) | Loosely connected collagen and elastin fibers |
| Intermediate layer | Predominantly elastic fibers |
| Deep layer | Densely arranged collagen fibers |
The intermediate + deep layers together form the vocal ligament.
The mucosal cover is mechanically separate from the body, allowing the wave to propagate freely - abnormalities of this wave (e.g., from scarring, edema) result in dysphonia.
- Cummings, p. 1024
8. Phonation Threshold Pressure
The minimum subglottic air pressure required to initiate vocal fold vibration is called the phonation threshold pressure. It is affected by:
- Size of the vocal folds
- Tension of the vocal folds
- Viscoelastic properties of the vocal fold cover
Vocal folds have inertia that must be overcome for phonation to begin.
- Scott-Brown's, p. 945; Cummings, p. 1025
9. Expiratory (Breath) Support
- Power for phonation comes from expired air.
- Depends on: lung volume, elastic recoil of chest wall and diaphragm, and strength of abdominal and intercostal muscles.
- Normal conversational speech is powered by passive expiration alone.
- Shouting/singing requires deeper prephonatory inspiration and active expiratory effort.
- Voice disorders from pulmonary disease become clinically significant when the compensatory capacity (extra breath effort) is impaired.
- Cummings, p. 1024
10. Vocal Fold Positioning and the Gap
- Vocal folds must be close enough for airflow to entrain oscillations.
- Too wide a gap → breathy voice or aphonia (only turbulent air noise, no periodic sound)
- Too tight (hyperadduction) → strained voice, excessive subglottic pressure needed
- Wider gaps can still phonate if airflow is proportionally higher; low airflow requires a narrower gap.
- Too loose → breathiness; Too tight → strained voice (KJ Lee)
- Cummings, p. 1024; KJ Lee, p. 916
11. Pitch Control (Fundamental Frequency)
- Fundamental frequency is controlled by changes in vocal fold length and tension.
- Cricothyroid (CT) muscle contraction: elongates and tenses the vocal fold → raises pitch
- Thyroarytenoid (TA) muscle contraction: decreases tension in the vocal cover → lowers pitch
- In the lower vocal range: TA contraction lowers pitch.
- During CT contraction without TA activity: falsetto is produced.
- Strengthening TA during CT contraction causes rising pitch.
Determinants of pitch range:
- Larynx size: smaller larynx (children) → higher pitch; larger larynx (adult males) → lower pitch
- Puberty: rapid laryngeal growth in boys causes unstable pitch ("voice breaking")
- Aging: loss of elasticity and ossification of thyroid lamina → elevation of pitch in older adults
- Lowest pitches produced by young men (longer, heavier, more compliant folds)
- Cummings, p. 1025
12. Vocal Registers
A register is defined in terms of laryngeal behaviour (governed by degree of vocalis muscle contraction), not just acoustic output.
| Register | Alternate Name | Characteristics |
|---|---|---|
| Loft | Falsetto | Highest frequencies; folds lengthened, extremely tense, thinned; minimal vibration; knife-thin edges almost adducted; high subglottic pressure; larynx raised |
| Modal | Chest/Normal speech | Range of everyday speech and singing; membranous folds adducted, full closure in closed phase; triangular cross-section; mucosal wave most prominent |
| Pulse | Vocal fry / Glottal fry / Creaky voice | Lowest frequencies; long closed phase per cycle; pulsatile sound; normal feature of speech |
- In modal low notes: intrinsic muscles relax, folds increase in bulk (opposing surface deepens from 3 to 5 mm), vibrating slowly along their whole length; infrahyoid muscles pull larynx down.
- In falsetto: only superior edges of vocal folds make contact; mucosal wave decreases markedly and is not visible; elastic recoil (rather than Bernoulli effect) drives closure; shorter closing phase.
- Scott-Brown's, p. 946; Cummings, p. 1024
13. Acoustics and Resonance
- The voice is a complex waveform (not sinusoidal); it contains a variety of formants and subharmonics.
- Increase in aperiodic components → dysphonia.
- The raw glottic sound resembles a "goose call" in isolation.
- Voice acquires human character through resonance of the chest, upper airway, and skull.
- Resonance = prolongation, amplification, and filtering of sound by sympathetic vibration.
- The enhanced vocal frequencies are called formants.
- The pharynx walls are too compliant to resonate directly; the primary resonator is the air column within the pharynx.
- The speaker controls resonance by: altering pharynx shape/volume, raising/lowering the larynx, moving tongue or jaw, and varying nasopharyngeal transmission.
- Supraglottic, hypopharyngeal, oropharyngeal, oral, and nasopharyngeal cavities all act as resonance chambers (KJ Lee).
- Cummings, p. 1025; KJ Lee, p. 916
14. Articulation (Source-Filter Hypothesis)
- The larynx is the source of a constant sound; the upper vocal tract is the filter.
- Consonants and vowels are formed by lips, tongue, palate, and pharynx.
- The larynx contributes primarily at onset and offset of phonation, coordinating to produce voiced vs. unvoiced sounds.
- Cummings, p. 1025; KJ Lee, p. 916
15. Neuroanatomy and Neural Control of Phonation
(Scott-Brown's, p. 941-942; Cummings, p. 1026)
Central Pathways
Periaqueductal grey matter (PAG) of the midbrain:
- Key site for mammalian voice production.
- Involved in both involuntary/emotional sounds and voluntary speech-related laryngeal motor patterns.
- Integrates cortical and subcortical aspects of language with respiratory/laryngeal motor patterns.
Nucleus retroambigualis (NRA):
- Receives projection from PAG.
- Generates respiratory pressure and laryngeal adduction for both vocalization and vegetative functions (e.g., coughing).
Nucleus ambiguus (NA):
- Contains motor neurons for all intrinsic laryngeal muscles, in a rostrocaudal organization:
- CT neurons most rostral
- LCA neurons most caudal
- PCA and CT neurons are significantly smaller than adductor neurons
- Influenced by both pyramidal and extrapyramidal systems.
Voluntary Phonation Pathway
- Arises in the pre-central gyrus (motor cortex), both hemispheres.
- Descends via corticobulbar tract (pyramidal / "direct activation" system).
- Some fibers stay ipsilateral; others decussate at bulbar level.
- Synapse at the vagal nuclei (nucleus ambiguus) in the reticular formation of the medulla.
- From there, via the vagus nerve (CN X) → intrinsic laryngeal muscles.
- Human speech and singing are controlled by direct corticobulbar projections to the nucleus ambiguus (a pathway not found in other animals).
Extrapyramidal System
- Includes basal ganglia, substantia nigra, subthalamic nucleus, cerebellum, thalamus.
- Regulates muscle tone, posture, and automatic components of skilled voluntary movement.
- Phonation may be adversely affected by neurological conditions involving these structures (e.g., Parkinson's disease).
Frontal Lobes
- Clinical cases and fMRI evidence show frontal lobe involvement in coordinated phonation and exhalation.
Reflex Control
- Laryngeal mechanoreceptors provide reflex feedback to stabilize and return vocal folds to pre-set patterns after displacement by expiratory airstream.
- This fine-tuning cannot be purely cortically regulated; it operates independently of auditory feedback (Wyke, Kirchner).
Sensory Feedback
- Auditory feedback: most important in learning to speak; less essential for everyday voice use.
- Tactile/proprioceptive feedback: vibration sensed in face, throat, and chest; important for trained singers.
- Laryngeal receptors respond to air pressure, flow, and joint motion.
16. Summary Table
| Aspect | Key Point |
|---|---|
| Theory | Myoelastic-aerodynamic (van den Berg) |
| Power source | Subglottic air pressure from expired air |
| Initiating force | Subglottic pressure exceeds vocal fold resistance |
| Closing forces | Bernoulli effect + myoelastic recoil |
| Mucosal wave | Travels inferior to superior; visible on stroboscopy |
| Body-cover concept | Vocalis = body; mucosa = cover |
| Pitch control | CT (raises) vs TA (lowers); length and tension |
| Registers | Loft (falsetto), Modal (speech), Pulse (vocal fry) |
| Resonance | Air column in pharynx; shaped by vocal tract |
| Articulation | Source-filter model |
| Neural center | Nucleus ambiguus (CN X); PAG; corticobulbar tract |
Compiled from: Cummings Otolaryngology Head and Neck Surgery (5th ed.), p. 1023-1026 | KJ Lee's Essential Otolaryngology (11th ed.), p. 916 | Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 941-946
From Scott brown volume 3 head and neck, chapter 59- physiology of larynx
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here are the complete notes on Chapter 59 - Physiology of the Larynx from Scott-Brown's Otorhinolaryngology Head & Neck Surgery, reproduced faithfully from the text.
Chapter 59: Physiology of the Larynx
Scott-Brown's Otorhinolaryngology Head & Neck Surgery
INTRODUCTION
This chapter covers the functions of the larynx with particular emphasis on its role as the source of the voice. It describes the motor and sensory laryngeal nerve supply, the neuroanatomy of phonation, the role of the larynx in swallowing, coughing and effort closure, and the biomechanics of phonation.
The larynx has a number of functions, the most important of which is to prevent foreign material from entering the airway (aspiration). This is achieved by:
- A combination of heightened sensitivity
- A strong sphincteric action during swallowing
- A means of effective expulsion via coughing
The larynx also acts as:
- A valve that controls air pressure and airflow
- A vibrator for generating sound (voice)
It is essential to be familiar with the considerable potential range of laryngeal adjustments that can occur in normal phonation, in order to avoid drawing inappropriate conclusions about phonatory physiology in a clinical setting.
1. THE NEUROANATOMY OF PHONATION
Definition: Phonation is a laryngeal motor behaviour used for speech production, involving highly specialized coordination of laryngeal and respiratory neuromuscular control. It is dependent upon the integrated functioning of many elements of the central and peripheral nervous systems (CNS and PNS).
Subcortical Control
-
Periaqueductal grey matter (PAG) of the midbrain is a crucial site for mammalian voice production.
- Involved in both emotional/involuntary sounds AND generation of specific respiratory and laryngeal motor patterns fundamental to human speech and singing.
- Patterned muscle activity corresponding to the major categories of voiced and voiceless sound production is represented in the PAG (Davis et al.).
- May integrate cortical and subcortical aspects of language with basic respiratory and laryngeal motor patterns by which speech is produced.
- The linguistic demands of intonation, phonemic differentiations and emotional nuances in quality appear to be regulated by this independent subcortical reflex neural system.
-
Nucleus retroambigualis (NRA):
- Receives projections from the PAG.
- Plays a significant role in generating respiratory pressure and laryngeal adduction occurring in both vocalization and vegetative manoeuvres (e.g., coughing).
Cortical / Voluntary Phonation Pathway
- The cortical mechanisms for vocalization and speech modulate the subcortical systems involved in involuntary/vegetative phonation (e.g., crying) - these mechanisms coordinate timing, pitch and intensity fluctuations with segmental and suprasegmental aspects of speech and voice.
- Frontal lobes and other cerebral structures are important in the integrated neurological systems required for phonation (fMRI evidence).
- fMRI has shown common volitional control of the two upper airway functions of phonation and exhalation.
- Multiple forebrain systems converge on motor neurons innervating the thyroarytenoid muscle.
Neural pathway for voluntary vocalization:
- Arises in the pre-central gyrus of the motor cortex, both cerebral hemispheres
- Fibres descend as part of the corticobulbar tract (pyramidal system / "direct activation" tract)
- On reaching the medulla:
- Some fibres take a direct pathway (remain ipsilateral) → synapse with ipsilateral vagus nucleus
- Other fibres decussate at bulbar level → synapse with contralateral vagal nucleus
- The vagal nuclei lie in the nucleus ambiguus within the reticular formation of the medulla, in a group of cells also containing CN IX and CN XI elements
- They are influenced by both the pyramidal and extrapyramidal systems
Pyramidal System
- Direct neurones: related to discrete movement
- Indirect neurones: multiple offshoots and synapses with basal ganglia and reticular formation; contribute to temporospatial orientation
- Upper motor neurones govern groups of muscles, not isolated muscles
- The frontobulbar portions of the pyramidal tracts connect with CN IX-XII, controlling articulation, phonation and respiration
Extrapyramidal System
Includes: basal ganglia (corpus striatum → caudate + lenticular nucleus [putamen + globus pallidus]), substantia nigra, subthalamic nucleus in upper brainstem, cerebellum, and thalamus.
- The cerebellum regulates force, speed, range, timing and direction of movements - excesses are inhibited
- The extrapyramidal system regulates muscle tone required for posture and position change; also involved in the automatic component of skilled voluntary movement
- The specific function of each extrapyramidal element with respect to phonation is unknown, but phonation may be adversely influenced by neurological conditions involving these structures
Reflex/Fine-Tuning Control
- Extrinsic and intrinsic muscles of the larynx are under voluntary cortical control - responsible for pre-phonatory tuning (precedes phonation), followed by phasic, tonic and volitional contractions; they also maintain length, tension, bulk and position of the vocal folds.
- The phonatory modulations during speech happen with precision and speed suggesting a finely coordinated system of reflex controls over:
- Laryngeal muscles themselves
- Abdominal and intercostal muscles maintaining subglottic air pressure
- Such fine tuning cannot be cortically regulated.
- Stimulation of all categories of laryngeal mechanoreceptors initiates activity in the larynx, ensuring vocal folds are stabilized and return to their pre-set pattern following displacement by the expiratory airstream.
- This monitoring of tonicity and position enables instantaneous and accurate adjustments.
- This process is independent of auditory feedback (Wyke; Kirchner).
2. LARYNGEAL INNERVATION
The vagus nerve (CN X) provides all the innervation to the intrinsic laryngeal muscles and the sensory structures of the larynx. It also supplies the pharynx, palate, trachea, bronchi, lungs, heart, external ear and parts of the GIT.
Origin of vagal fibres:
- Some fibres originate in the medulla in the nucleus ambiguus:
- Rostral pole: motor neurons for CN IX (glossopharyngeal)
- Middle part: motor neurons for CN X (vagus)
- Caudal pole: motor neurons for CN XI (accessory)
- The right and left vagus nerves provide ipsilateral innervation to the larynx.
CN IX, X and XI are intimately connected in the medulla that all muscles supplied by them are frequently involved equally or progressively in medullary lesions - termed the 'glossopharyngeal-accessorius complex' (Walshe). Nuclear lesions of the vagus can therefore cause paralysis of the palate, tongue and larynx simultaneously.
Branches of the Vagus Relevant to the Larynx

Fig. 59.3 Diagrammatic representation of the laryngeal nerve supply. (Mathieson)
Superior Laryngeal Nerve (SLN)
- Branches off from the vagus at the ganglion nodosum (inferior ganglion), below the level of the jugular foramen
- Subdivides into internal and external branches:
Internal branch of the SLN:
- Contains sensory and parasympathetic secretomotor fibres
- Supplies glands within tissue above the level of the vocal folds
- Divides into three branches:
- Superior branch: runs to the lingual surface of the epiglottis; sends small fibres through epiglottic foramina to laryngeal surface
- Middle branch: runs through the aryepiglottic fold into the ventricular fold
- Inferior branch: runs to the pyriform sinus and postcricoid region; forms anastomoses with the RLN
- Density of sensory innervation greatest at the laryngeal inlet (protective mechanism for respiratory system)
- Laryngeal surface of the epiglottis has the greatest sensory innervation
- Vocal folds have a lower density of sensory fibres; the anterior vocal folds have a lower density than the posterior half
External branch of the SLN:
- Provides motor supply to the cricothyroid muscle
Recurrent Laryngeal Nerve (RLN)
- Provides motor supply to all intrinsic laryngeal muscles (except cricothyroid)
- Contains both adductor and abductor fibres
- Also provides sensory supply to the glottis and subglottis
Asymmetry between left and right RLN:
| Right RLN | Left RLN | |
|---|---|---|
| Origin | Arises from vagus in front of subclavian artery | Arises from vagus at the arch of the aorta |
| Course | Shorter | More extensive |
| Vulnerability | Less | More - especially to: aortic aneurysm, intrathoracic masses, thyroidectomy, thoracic surgery |
Therefore, left vocal fold paralysis is far more common than right vocal fold paralysis.
Both RLNs ascend the groove between trachea and oesophagus, dividing into anterior and posterior branches before entering the larynx behind the cricothyroid articulation.
- Recent evidence: ventricular fold adduction is a result of ventricularis muscle contraction mediated by the RLN.
Pharyngeal Nerve
- Descends between internal and external carotid arteries
- Supplies middle pharyngeal constrictor
- Fibres join with glossopharyngeal, external laryngeal nerves and sympathetic trunk branches → form the pharyngeal plexus
- Pharyngeal plexus supplies: pharynx and all muscles of the soft palate except tensor palati
3. LARYNGEAL MECHANORECEPTORS
Free fibrils and terminal filaments enclosed in capsules constitute the receptor end organs (mechanoreceptors) embedded in laryngeal tissues at sites sensitive to muscle stretch and airflow pressures. Some protect the airway; others contribute to control of phonation.
- Reflex closure of the larynx is triggered by tactile receptors in the glottic and supraglottic mucosa, which evoke reflex contraction of laryngeal muscles.
- Subglottic mucosal receptors elicit laryngeal closure and cough.
Wyke's classification - three sites of mechanoreceptors:
-
Mucosal mechanoreceptors - in the mucosal lining of the larynx
- Corpuscular nerve endings in the surface covering of the vocal folds
- Particularly numerous and sensitive to: muscle stretch, air pressure level, liquid and touch
- Discharge impulses into afferent fibres of the vagus
-
Articular mechanoreceptors - in the capsules of the articulatory joints
- Existence and function remain controversial
-
Myotatic mechanoreceptors - in the extrinsic and laryngeal muscles
- Tone of laryngeal muscles depends on the myotatic reflex, a function of the muscle spindles
- Laryngeal muscles contain a large number of muscle spindles
4. FUNCTIONS OF THE LARYNX
4a. Swallowing (Deglutition)
The primary function of the larynx during swallowing is to prevent food and liquid entering the airway, achieved by:
- Sphincteric action of the aryepiglottic folds, true vocal folds and ventricular folds
- Occurs simultaneously with elevation of the larynx (also important for cricopharyngeal sphincter control)
Stages of swallowing:
- Oral stage (voluntary): oral preparatory stage (manipulation and breakdown of bolus by tongue) + oral transport stage (propulsion toward oropharynx)
- Pharyngeal stage (reflex): initiated when bolus reaches back of tongue:
- Glottis closed by adduction of arytenoids + contraction of lateral cricoarytenoid muscles, false and true vocal folds
- Vocal fold adduction during swallowing averages approximately 2.3 seconds
- Epiglottis covers laryngeal entrance and directs bolus into valleculae and pyriform sinuses
- Rapid laryngeal elevation displaces hyoid anteriorly - further protects airway
- When bolus arrives at upper border of cricopharyngeus: sphincter relaxes, bolus enters oesophagus
4b. Coughing
Coughing expels material from the airway. The laryngeal adductor response is a protective reflex:
- Rapid inspiration
- Forceful closure of both vocal folds and ventricular folds
- Air pressure builds below adducted folds as diaphragm ascends spasmodically
- Folds separate explosively - mucus or foreign material expelled
This laryngeal motor response to sensory stimuli is not suppressed during volitional laryngeal tasks.
4c. Effort Closure (Valsalva)
- Laryngeal structure evolved to contain intrathoracic pressure to provide a stable fulcrum for the upper limbs.
- Expiratory effort against a closed glottis = Valsalva manoeuvre.
- During exertion involving arms: vocal folds are firmly adducted, preventing air expulsion and chest wall collapse, providing a fixed origin for arm and shoulder muscles.
Clinical relevance:
- Laryngectomy or vocal fold paralysis → difficulty with weight-bearing activities (inability to close glottis effectively)
- Trauma to vocal fold mucosa can occur from forceful, prolonged vocal fold adduction during physical training (e.g., weight-lifting)
- Effort closure also occurs during childbirth and defaecation (abdominal contents compressed by abdominal muscles)
5. BIOMECHANICS OF PHONATION
The vocal folds are composed of laryngeal connective tissues with complex matrix composition providing viscoelastic mechanical properties required for voice production.
At rest / quiet respiration:
- Vocal folds abduct on inspiration, slightly adduct on expiration
- Move slightly up and down with respiratory air flow
- Larynx descends on inspiration and ascends on expiration
- Full abduction occurs in forceful inspiration
- Subglottic and supraglottic influences must be considered when analyzing vocal fold dynamics
5a. INITIATION OF VOICE
- Pre-phonatory inspiratory phase (Wyke): vocal folds rapidly abduct to allow air intake
- Vocal folds adducted by contraction of the lateral cricoarytenoid muscles
- Vocal note generated by pulmonary air exhaled between adducted folds
- The vocal folds together constitute the vibrator, activated by exhaled air (the excitor)
- Subglottic air pressure increases below adducted folds until it overcomes their resistance and blows them apart - setting vibratory cycles in motion
- The vocal folds (like all vibrators) have inertia that must be overcome
Phonation Threshold Pressure:
- The amount of air pressure required to begin voicing
- Affected by: size + tension of vocal folds in combination with the viscoelastic properties of the vocal fold cover
6. THE VIBRATORY CYCLE
Each vibratory cycle of the vocal folds consists of three phases: adduction, aerodynamic separation and recoil.
Step-by-step:
- Increased subglottic pressure overcomes resistance of adducted vocal folds
- Vocal folds peel apart from their inferior border
- When they finally separate at the superior margin, a puff of air is released
- Bernoulli effect: resulting negative pressure in the glottis → vocal folds close rapidly, inferior vocal fold margins closing first
"When air passes from one large space to another through a constriction (the glottis), the velocity will be greatest and the pressure least at the site of the constriction" (Maran) The drop in pressure at the glottis draws the vocal fold mucosa into the space between the folds
- Contact between vocal folds increases until subglottic air pressure overcomes resistance again → cycle recommences
Each vibratory cycle = one mucosal wave travelling from inferior to superior surface
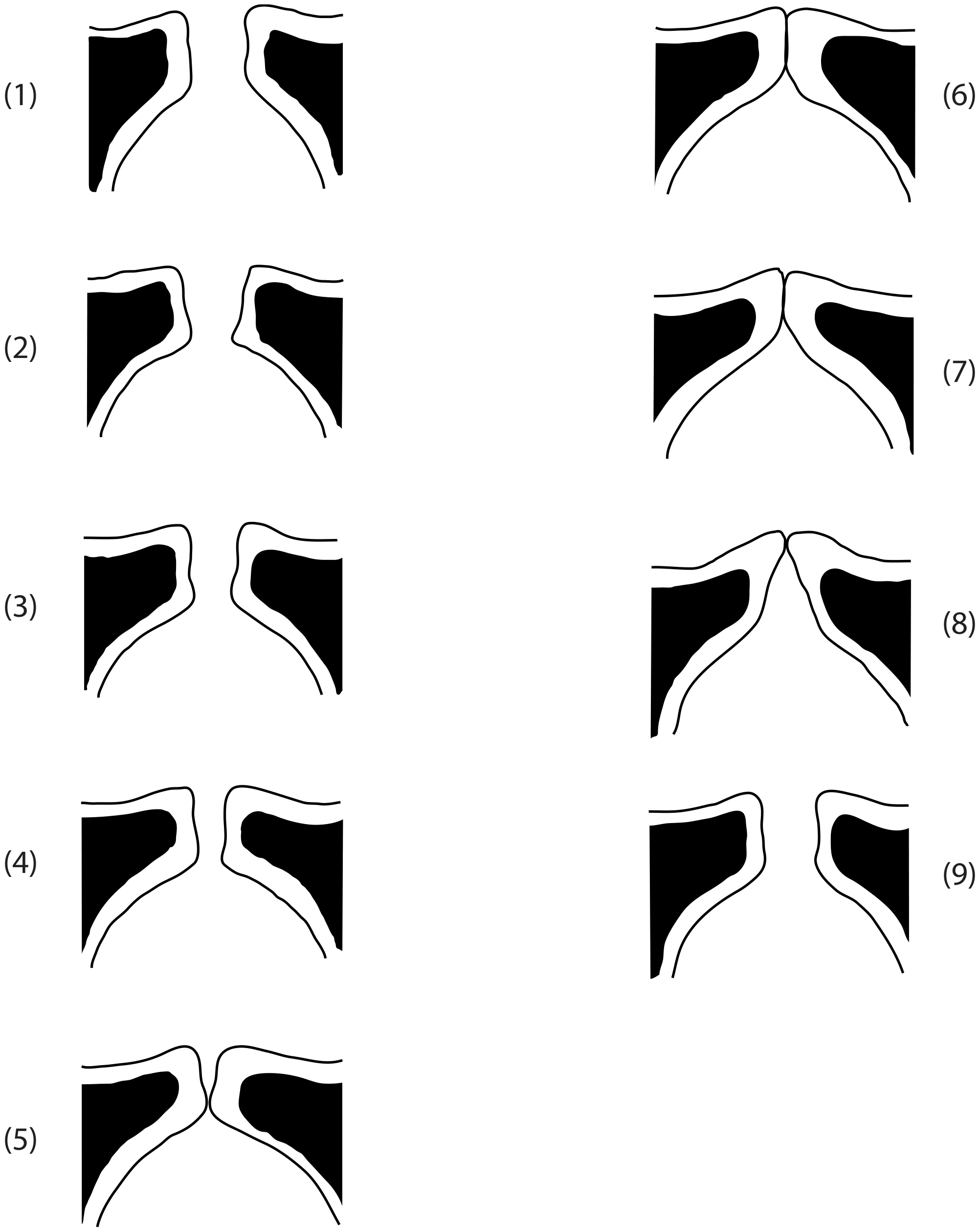
Fig. 59.4 Vocal fold vibratory cycle (Mathieson)
Cover/Body Theory
The mechanism by which the mucosal wave occurs is explained by the cover/body theory:
- Body = vocalis muscle - provides the firm body of the vocal fold
- Cover = mucous membrane - blown by the expiratory airstream over the body
Undulations of the vocal fold's thin cover and any abnormalities of the mucosal wave can only be observed using laryngostroboscopy or high-speed photography.
Four Phases of the Vibratory Cycle
| Phase | Description |
|---|---|
| Closing phase | Vocal folds begin to close rapidly from their lower margin |
| Closed phase | Medial edges of vocal folds in full contact |
| Opening phase | Folds begin to separate from lower margin; gradually peel apart; superior margin remains in contact until end of phase |
| Open phase | Vocal folds separated (the longest part of a normal cycle) |
The closing phase is more rapid than the opening phase.
Glottal Configuration and Approximation
- Folds must be structurally and functionally symmetrical, at the same level, and close rapidly for a clear vocal note to be maintained.
- Insufficient approximation (glottal insufficiency) → air wastage + breathy voice quality
- When membranous folds fail to approximate with a slightly increased aperture in the cartilaginous section → turbulent air escapes and is audible
Middle pitch phonation: interarytenoid muscles adduct the cartilaginous portion and hold them together, while the anterior portion is gently adducted but free to vibrate.
Important: incomplete glottal closure and normal phonation:
- Full vocal fold adduction during phonation has traditionally been regarded as the norm, but studies have refuted this
- Normal phonation can occur with incomplete glottal closure
- This pattern is more common in women than men
- In all speakers, incomplete glottal closure is normal in high-frequency modal voice and in falsetto (hourglass or spindle configurations can occur normally)
- Posterior glottal chink: common finding in young and middle-aged women
- Anterior chinks: more likely in elderly women
- In children: posterior glottal gap and predominantly open phase should be considered normal glottal configuration
- Similarly, arytenoid asymmetries should be viewed with caution - not necessarily indicative of pathology
Age-Related Changes
- Changes in pitch and breath rate in older individuals indicate fundamental change in maintenance of the speech mechanism
- Reductions in pulmonary elastic recoil and respiratory muscle strength affect subglottal air pressure generation for speech
- Older adults have very different lung volume adjustments for loud speech compared to young adults
7. VOCAL REGISTERS: CHARACTERISTICS OF VOCAL FOLD ADDUCTION AND VIBRATION
Significant variations in vocal fold vibratory characteristics and adduction occur according to the vocal register in use.
The subject of vocal registers is confusing and controversial. Listeners cannot reliably identify the change from one register to another.
Terminology conflict:
- Singers: classify as head, middle, chest (regarded as unsatisfactory by voice scientists)
- Voice scientists: refer to falsetto, modal and vocal fry
Hollien's proposal (clarified by Baken and Orlikoff): registers should be defined in terms of laryngeal behaviour (governed by degree of contraction of the vocalis muscle), not in acoustic terms. This gives three terms: loft, modal and pulse registers.
Table 59.1 - Vocal Registers
| Register | Also called | Frequency | Vocal fold characteristics |
|---|---|---|---|
| Loft | Falsetto | Highest frequencies | Lengthened, extremely tense, thinned; minimal vibration; knife-thin free edges almost adducted; high subglottic air pressure; larynx raised by suprahyoid muscles; pharynx shortened |
| Modal | Chest / Normal speech | Range used in everyday speech and singing | Membranous folds adducted; complete closure in closed phase; triangular cross-section in low notes: intrinsic muscles relax, folds increase in bulk (opposing surfaces deepen from 3 mm to 5 mm); vibrate slowly along whole length; lower surfaces make contact and separate as upper surfaces approximate (rolling / figure-of-eight motion); in lowest notes: infrahyoid muscles pull larynx down |
| Pulse | Glottal fry / Vocal fry / Creaky voice | Lowest vocal frequencies | Pulsatile nature; long closed phase in each vibratory cycle; normal feature of speech |
The terminology related to vocal registers is not consistent. Various overlapping terms are used that have different theoretical bases.
8. FUTURE RESEARCH (areas identified in chapter)
- Detailed innervation of laryngeal structures
- Processes of regulation of linguistic demands of intonation and emotional nuances in vocal quality
- The cerebral systems controlling phonation
- Studies of normal variations of the vocal tract during phonation
KEY POINTS (from chapter)
- The prime function of the larynx is to protect the airway. It also acts as a valve controlling airflow and air pressure and as a vibrator for generating sound (voice).
- The vagus nerve (CN X) provides all the innervation to the intrinsic laryngeal muscles and to the sensory structures of the larynx.
- Phonation involves highly specialized coordination of laryngeal and respiratory neuromuscular control.
- The quality of the glottal source sound is dependent on the structure and function, particularly the efficiency of approximation, of the vocal folds.
- An understanding of normal and age-related differences of glottal configurations is essential in order to avoid pathologizing normal laryngeal structure and function.
Source: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 59 - Physiology of the Larynx, pp. 941-947
This is a shared conversation. Sign in to Orris to start your own chat.