Term child just born cried after stimulation,grunting what are intial managment , cpap setting etc
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Searching the Web
neonatal CPAP settings term infant grunting initial pressure FiO2 NRP 2020 guidelines
Searching PubMed
term neonate respiratory distress CPAP management
Here is a thorough, guideline-based answer for this clinical scenario.
Term Neonate: Cried After Stimulation, Now Grunting - Initial Management
Clinical Interpretation
This is a term neonate with labored breathing / signs of respiratory distress (grunting) after initial stimulation. The baby is NOT apneic and DID cry, so the primary pathway is: labored breathing/persistent cyanosis branch of the NRP algorithm - NOT immediate PPV.
NRP Algorithm (per current AHA/AAP guidelines):
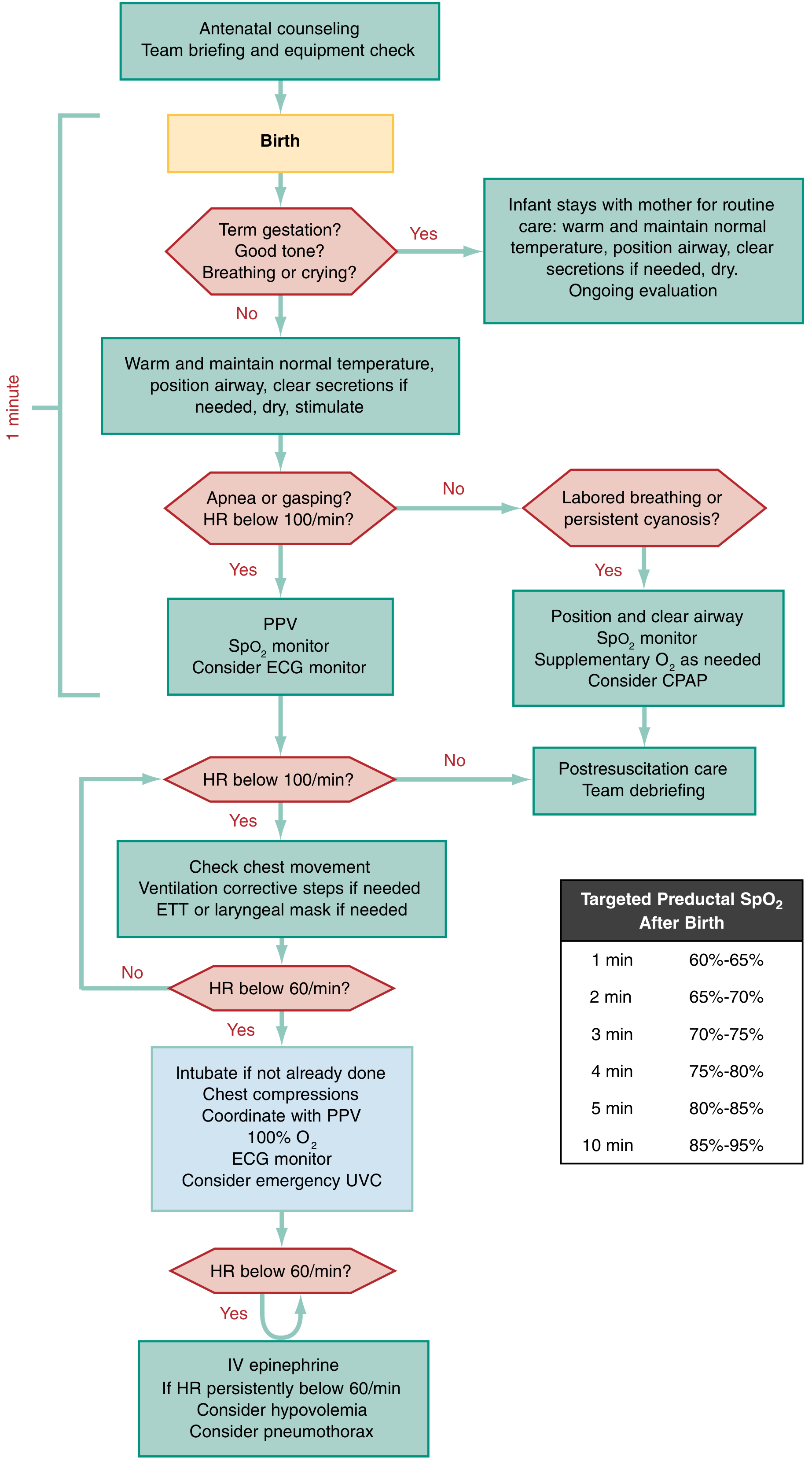
Rosen's Emergency Medicine, Fig 159.5 - NRP Algorithm with targeted preductal SpO2 targets
Step-by-Step Initial Management
1. Immediate Initial Steps (within 60 seconds - the "Golden Minute")
- Warm - place under radiant warmer, maintain body temp 36.5-37.5°C
- Dry - towel dry thoroughly (this itself provides stimulation)
- Position airway - neutral "sniffing" position (slight neck extension)
- Clear secretions (only if needed) - suction mouth first, then nose, with bulb syringe; keep suction <100 mmHg. Do NOT routinely suction if no obvious obstruction
- Assess simultaneously: breathing effort, heart rate (HR), color/SpO2
2. Assess the Three Key Parameters
| Parameter | Finding in This Baby |
|---|---|
| Breathing | Grunting (labored, but breathing) |
| Heart rate | Assess immediately (target >100 bpm) |
| Color / SpO2 | Assess for central cyanosis |
3. Since Baby Has Labored Breathing (Grunting) + HR ≥100:
Per NRP algorithm - "Labored breathing or persistent cyanosis" branch:
- Position and clear airway
- Apply pulse oximeter to right hand/wrist (preductal)
- Supplemental O2 as needed - start with room air (FiO2 0.21) and titrate up
- Consider CPAP
CPAP - Indications and Settings
Indication: Any term neonate with persistent grunting, nasal flaring, or tachypnea who is spontaneously breathing with HR ≥100 bpm.
"Any neonate with persistent cyanosis or signs of respiratory distress (e.g., grunting, nasal flaring, tachypnea) should be assisted by CPAP or PPV." - Rosen's Emergency Medicine
CPAP Settings for a Term Neonate
| Parameter | Setting | Notes |
|---|---|---|
| PEEP/CPAP pressure | 5-6 cm H2O | Start at 5; can go up to 8 cmH2O if needed |
| FiO2 | 0.21 (room air) to start | Titrate up by 10% increments to meet SpO2 targets |
| Flow rate | 5-10 L/min | (device-dependent; T-piece or bubble CPAP) |
| Interface | Nasal prongs (Hudson) or mask | Nasal prongs preferred; ensure good seal |
Targeted Preductal SpO2 After Birth (NRP targets)
| Time after birth | Target SpO2 |
|---|---|
| 1 min | 60-65% |
| 2 min | 65-70% |
| 3 min | 70-75% |
| 4 min | 75-80% |
| 5 min | 80-85% |
| 10 min | 85-95% |
- These are preductal targets - probe on right hand/wrist
- Do NOT panic if SpO2 is 60% at 1 minute - this is physiologically normal
- Titrate FiO2 upward only if not meeting lower end of targets despite CPAP
Escalation Triggers (When to Move Beyond CPAP)
| Situation | Action |
|---|---|
| HR drops <100 bpm | Initiate PPV (BMV) at 40-60 breaths/min |
| No improvement with PPV >2 min | Insert orogastric tube (prevent gastric distension); consider ETT |
| HR <60 bpm despite adequate ventilation | Add chest compressions (3:1 ratio) + PPV + consider intubation |
| HR <60 despite compressions + PPV | 100% FiO2 + IV/UVC epinephrine |
PPV Settings if Required (T-piece resuscitator):
- PIP (peak inspiratory pressure): 20-25 cm H2O for term (first breaths may need 30-40 cm H2O to clear lung fluid)
- PEEP: 5 cm H2O
- Rate: 40-60 breaths/min
- FiO2: Start at 0.21 (room air) for term neonates
Causes of Grunting to Consider Simultaneously
Grunting is a sign of expiratory braking to maintain FRC - always think:
- Transient tachypnea of newborn (TTN) - most common in term babies (especially C-section)
- Retained lung fluid
- Early-onset pneumonia / sepsis
- Meconium aspiration syndrome (if meconium present)
- Congenital pneumonia
- Hypothermia / hypoglycemia - check blood glucose early
- Congenital heart disease (if cyanosis persists despite O2)
Key Monitoring (Ongoing)
- SpO2 - right hand (preductal), continuous
- 3-lead ECG - more accurate than pulse ox for HR in first minutes
- Blood glucose - check within 30-60 min of birth
- Temperature - axillary; maintain 36.5-37.5°C
- Respiratory rate - normal <60 breaths/min; grunting should resolve
- APGAR score at 1, 5, and 10 minutes
Bottom line: This term baby who cried after stimulation but is now grunting falls in the "labored breathing" pathway. Start with positioning, airway clearance, SpO2 monitoring, and nasal CPAP at 5-6 cm H2O, room air (FiO2 0.21). Titrate FiO2 to meet preductal SpO2 targets. Escalate to PPV only if HR drops <100 or respiratory distress worsens.
- Rosen's Emergency Medicine, 10e, pp. 3126-3127
- NRP current guidelines summary - PMC
- Merck Manual - Neonatal Resuscitation
Antibiotics?
Finding Sources
Finding Sources
Searching the Web
early onset neonatal sepsis antibiotics empirical therapy term neonate grunting 2023 2024 guidelines
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Here is a complete, structured answer on antibiotics for this baby.
Antibiotics in the Term Neonate with Grunting
First Principle: Antibiotics Are NOT Part of Initial Resuscitation
"Antibiotics are not indicated in the initial resuscitation phase but may be required once the neonate has been stabilized." - Rosen's Emergency Medicine, 10e
So the first question is: does this baby have risk factors for Early-Onset Sepsis (EOS)?
Step 1 - Risk Stratify for EOS (0-72 hours of life)
Before prescribing antibiotics, assess these maternal and neonatal risk factors:
| Risk Factor | Detail |
|---|---|
| Maternal GBS status | GBS positive, or unknown/untested |
| Intrapartum antibiotic prophylaxis | Was it given, and was it adequate (≥4 hrs before delivery)? |
| Maternal fever | ≥38°C intrapartum |
| Chorioamnionitis | Clinically diagnosed or suspected |
| Prolonged rupture of membranes | PROM ≥18 hours |
| Preterm birth | <37 weeks (more risk) |
| Clinical signs in baby | Grunting, tachypnea, poor tone, temperature instability |
Key pathogens in EOS:
- Group B Streptococcus (GBS) - #1 in term infants
- E. coli - #2
- Klebsiella spp., Enterobacter spp., Listeria monocytogenes
Step 2 - Decision to Start Antibiotics
Use clinical judgment + EOS risk calculator (Kaiser Permanente EOS Calculator or equivalent):
| Scenario | Action |
|---|---|
| Baby looks well, no maternal risk factors | Observe, serial exams - NO empirical antibiotics needed |
| Grunting resolves quickly (TTN), no risk factors | Observe; blood culture if any concern |
| Grunting persists + maternal risk factors present | Draw blood culture + CBC/CRP → Start antibiotics empirically |
| Baby unwell: poor perfusion, hypotonia, apnea | Immediate blood culture + LP if stable → Start antibiotics |
| Chorioamnionitis confirmed | Always start antibiotics regardless of baby's appearance |
Modern guidelines (Swiss Society of Neonatology, 2023) emphasize: "Neonates without any clinical signs of sepsis should not be treated with antibiotics" - the goal is to reduce unnecessary antibiotic use.
Step 3 - Empirical Antibiotic Regimen
First-line (standard of care worldwide):
| Drug | Dose | Frequency | Route |
|---|---|---|---|
| Ampicillin | 50 mg/kg/dose (sepsis) | Q12h (term, 0-7 days) | IV |
| Gentamicin | 4-5 mg/kg/dose | Q36h (term neonate, PMA 37-44 wks, postnatal 0-7d) | IV |
Rationale: Covers GBS (ampicillin) and gram-negative organisms including E. coli (gentamicin).
Dosing details for term neonate (PMA 37-44 weeks, 0-7 days old):
| Drug | Dose | Interval |
|---|---|---|
| Ampicillin | 25-50 mg/kg/dose | Q12h |
| Gentamicin | 4 mg/kg/dose | Q36h |
(Harriet Lane Handbook, 23rd ed.)
If meningitis suspected (bulging fontanelle, seizures, CSF pleocytosis):
- Ampicillin dose increases to 300 mg/kg/day divided Q8h (GBS meningitis)
- Replace gentamicin with cefotaxime 50 mg/kg/dose IV (better CNS penetration)
- Do NOT use ceftriaxone in neonates - displaces bilirubin from albumin → risk of kernicterus
Step 4 - Investigations Before Starting Antibiotics
Ideally collect before first dose (but do NOT delay antibiotics in a sick baby):
- Blood culture x1 (minimum 1 mL)
- CBC with differential - neutropenia/neutrophilia, I:T ratio >0.2
- CRP (may be normal in first 6-12 hours; repeat at 24h)
- Blood glucose (always in neonates)
- LP (if meningitis suspected or baby critically ill) - CSF culture, cell count, protein, glucose
- CXR (if respiratory distress - pneumonia vs TTN vs RDS)
- Urine culture - not useful in EOS (only relevant in LOS >72h)
Step 5 - Duration and De-escalation
| Situation | Duration |
|---|---|
| Blood culture negative, baby improves, labs reassuring | Stop at 36-48 hours (current evidence supports 24-48h is safe) |
| Culture-positive bacteremia (no meningitis) | 10-14 days |
| GBS meningitis | Minimum 14 days |
| Gram-negative meningitis | Minimum 21 days |
A 2023 study found stopping empirical antibiotics at 24 hours had a similar safety profile to the standard 48-hour course when cultures are negative and the baby is clinically well.
Quick Reference Summary
Term neonate, grunting, post-stimulation cry:
1. Stabilize first (CPAP, warmth, monitoring)
2. Assess EOS risk factors
3. If any clinical concern or risk factors:
→ Blood culture + CBC + CRP + glucose + CXR
→ Ampicillin 50 mg/kg IV Q12h
→ Gentamicin 4 mg/kg IV Q36h
4. If meningitis suspected: swap gentamicin → cefotaxime 50 mg/kg IV
5. De-escalate at 36-48h if cultures negative + baby well
- Rosen's Emergency Medicine, 10e, p. 3128
- Harriet Lane Handbook, 23rd ed., Table 18.13
- Antibiotic therapy for neonatal sepsis overview 2024 - PMC
This is a shared conversation. Sign in to Orris to start your own chat.