Week rottar cuff muscle symtom and how to strengthen each muscles and also in group
Reading File
Finding Sources
Searching the Web
rotator cuff muscles weak symptoms strengthening exercises each muscle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me compile it:
Weak Rotator Cuff - Muscles, Symptoms & Strengthening
The 4 Rotator Cuff Muscles (SITS)
The rotator cuff is made up of four muscles whose tendons form a "cuff" around the humeral head, stabilizing the glenohumeral joint and controlling rotation. A helpful mnemonic is SITS:
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa (posterior scapula, above spine) | Greater tuberosity (superior) | Initiates abduction (first 15-30°) | Suprascapular nerve |
| Infraspinatus | Infraspinous fossa (posterior scapula, below spine) | Greater tuberosity (posterosuperior) | External rotation | Suprascapular nerve |
| Teres minor | Lateral border of scapula | Greater tuberosity (posterior) | External rotation, weak adduction | Axillary nerve |
| Subscapularis | Subscapular fossa (anterior scapula) | Lesser tuberosity | Internal rotation | Upper & lower subscapular nerves |
"The subscapularis is the largest of the rotator cuff muscles... The supraspinatus superiorly, the infraspinatus posterosuperiorly, and the teres minor posteriorly [all insert on the greater tuberosity]." - Rockwood and Green's Fractures in Adults, 10th ed.
General Symptoms of a Weak/Injured Rotator Cuff
From the textbooks (Miller's Review of Orthopaedics, Harrison's, Campbell's):
- Dull, aching pain deep in the shoulder, often in the deltoid region
- Night pain - woken by rolling onto the affected shoulder
- Weakness with overhead activities - lifting, reaching, throwing
- Painful arc - pain between 60-120° of active abduction
- Loss of active range of motion while passive range is often preserved (key sign)
- Difficulty with everyday tasks - combing hair, reaching behind the back, fastening a bra
- Muscle atrophy - wasting visible above/below the scapular spine (supraspinatus/infraspinatus) with chronic tears
- Acute onset - sudden pain and weakness after a fall on outstretched hand or heavy lift (traumatic tear)
Symptoms Specific to Each Muscle When Weak
1. Supraspinatus (most commonly injured)
- Inability to initiate shoulder abduction (arm lifting away from side)
- "Drop arm" - cannot sustain the arm at 90° against gravity or resistance
- Painful arc between 60-120°
- Weakness on the empty can test (arm at 30° forward, thumb pointing down - resistance applied)
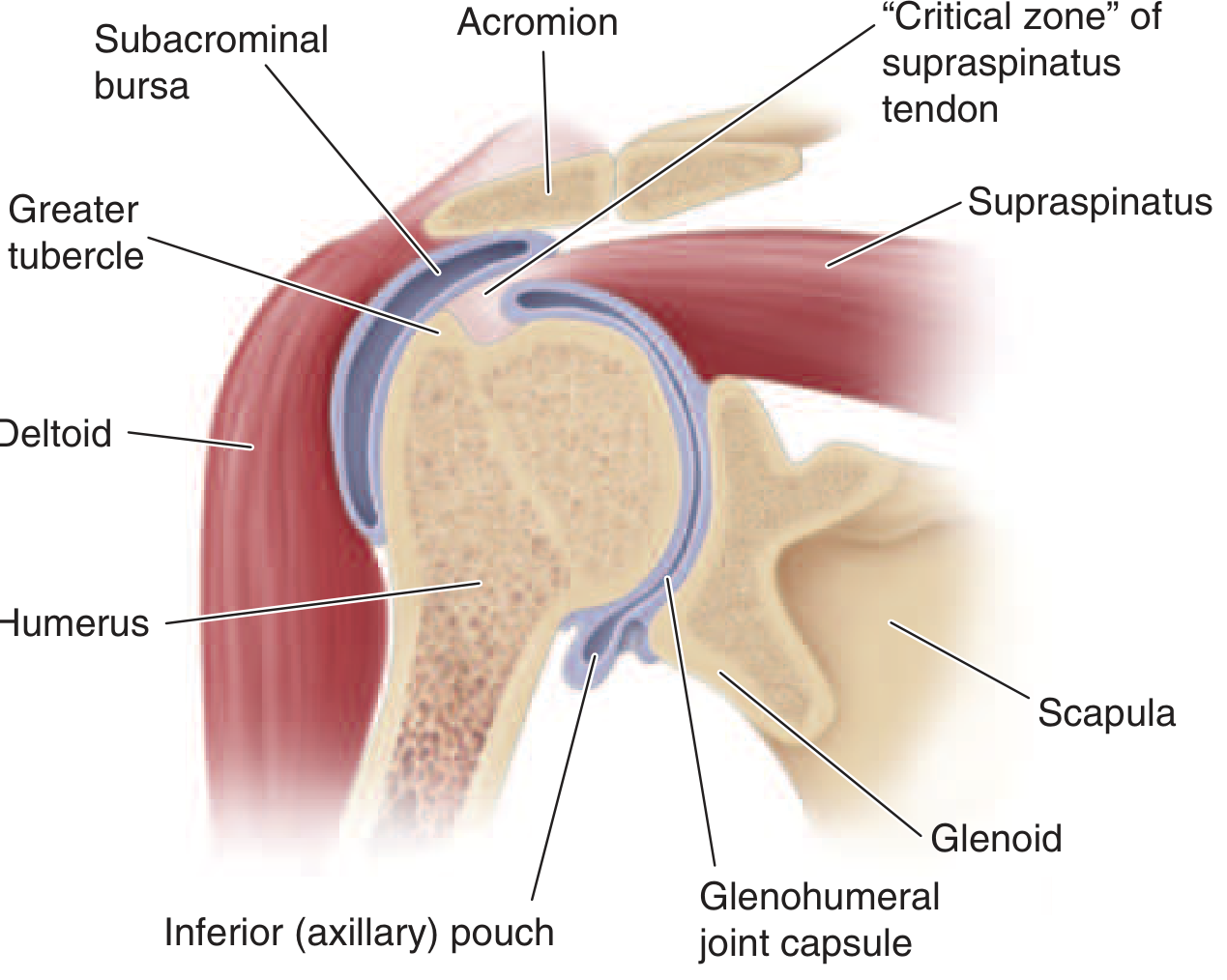
- Most tears begin here, often in the "critical zone" of poor blood supply near the insertion
2. Infraspinatus
- Weakness of external rotation - difficulty rotating the forearm away from the body with elbow at 90°
- Trouble with overhead throwing motions (e.g., tennis serve, pitching)
- Hornblower's sign if combined with teres minor tear - cannot hold the hand to the mouth without abducting the elbow
- Visible atrophy in the infraspinous fossa below the spine of the scapula
3. Teres Minor
- Also weak external rotation, but isolated weakness is uncommon
- Contributes to the hornblower's sign alongside infraspinatus
- Usually affected alongside infraspinatus
4. Subscapularis (least commonly torn, but most powerful)
- Weakness of internal rotation - trouble tucking in shirt behind the back, reaching the spine
- Belly press test - cannot press the palm against the abdomen while keeping the elbow forward
- Lift-off test (Gerber) - cannot hold the hand away from the lower back against resistance
- Pain with reaching across the body
Strengthening Exercises - Individual Muscles
Supraspinatus
Empty Can / Full Can Raises
- Stand with arm at side. Raise arm to shoulder height at 30° forward of the coronal plane (the scapular plane), thumb pointing down (empty can) or up (full can - safer, less impingement).
- Start with no weight; progress to 1-3 lbs.
- 3 sets x 15 reps
Side-Lying Abduction
- Lie on the unaffected side, raise the top arm to shoulder height in the plane of the scapula.
- Keep thumb pointing up.
- 3 sets x 15 reps
Infraspinatus + Teres Minor (both are external rotators - trained together)
Side-Lying External Rotation (most targeted exercise)
- Lie on the unaffected side, affected arm on top, elbow bent 90°, forearm resting across abdomen.
- Slowly rotate forearm up toward the ceiling, keeping elbow pinned to the side.
- Hold 1-2 seconds at top, lower slowly (eccentric phase is key).
- 3 sets x 10-15 reps. Start with 1-2 lbs.
Banded External Rotation (standing)
- Stand with elbow bent 90°, tucked against the side (place a folded towel between elbow and ribs to maintain position).
- Resistance band anchored at elbow height.
- Rotate forearm outward, hold, return slowly.
- 3 sets x 12-15 reps.
Subscapularis
Internal Rotation with Band
- Stand with elbow at 90° tucked to your side.
- Band anchored behind you at elbow height.
- Rotate forearm in toward the abdomen against resistance, return slowly.
- 3 sets x 12-15 reps.
Belly Press Progression
- Press palm against abdomen keeping the elbow forward (not dropping to the side).
- Progress to adding resistance by pressing into a wall with forearm.
Strengthening as a Group (Full Rotator Cuff Programs)
These exercises train all four muscles together and also recruit the scapular stabilizers, which are essential for restoring the normal "scapulohumeral rhythm."
Phase 1 - Pain Control / Early Rehab
- Pendulum swings - lean forward, let arm hang, make small circles with gravity - unloads the joint, reduces spasm
- Passive range of motion - no muscle work, just restoring movement
Phase 2 - Range of Motion Restoration
- Posterior capsule stretch (cross-body stretch) - pull the affected arm across the chest with the other hand; holds the posterior capsule and infraspinatus
- Sleeper stretch - lie on affected side, push forearm down gently; stretches posterior capsule
Phase 3 - Strengthening (all four muscles + scapula)
Prone Y/T/W raises - excellent group exercise
- Lie face down on a table or elevated surface. Raise both arms:
- Y shape (arms angled forward) = targets supraspinatus
- T shape (arms straight out) = infraspinatus/teres minor
- W shape (elbows bent, hands up) = subscapularis/external rotators
Scapular rows (resisted)
- Pull resistance band toward your chest keeping elbows close to the body.
- Trains the rotator cuff and the lower trapezius/rhomboids together - restores scapular rhythm.
Wall push-up plus
- Push-up against a wall, add a "plus" at the top by protracting (pushing) the scapula forward.
- Activates serratus anterior to stabilize the scapula, allowing the rotator cuff to work from a stable base.
Diagonal PNF patterns (D1/D2 patterns)
- Often guided by a physiotherapist; combines flexion-abduction-external rotation in one diagonal movement, training all cuff muscles in functional patterns similar to daily activities.
Key Training Principles
| Principle | Why It Matters |
|---|---|
| Use the scapular plane (~30° forward) | Reduces impingement under the acromion |
| Eccentric emphasis (slow lowering) | Builds tendon load tolerance; reduces re-injury |
| Start light (1-3 lbs) | The rotator cuff is an endurance/stabilizer group - heavy loads recruit the deltoid instead |
| Pain-free range only | Sharp/catching pain means tissue is being compressed |
| Fix the scapula first | A poorly moving scapula closes the subacromial space; always include scapular exercises |
Important note: If you have significant pain, a known tear, or weakness that doesn't improve after 4-6 weeks of conservative exercise, see an orthopaedic physician or physiotherapist. An MRI can determine whether a tear is partial or full-thickness, which significantly changes management - particularly whether surgery is needed before starting a strengthening program.
Sources: Harrison's Principles of Internal Medicine 22E; Miller's Review of Orthopaedics 9th Ed; Campbell's Operative Orthopaedics 15th Ed; Rockwood and Green's Fractures in Adults 10th Ed; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.