What is awareness under anesthesia . Monitoring of depth of Anaesthesia and Recent advances . Prevention of awareness during Anaesthesia. For md Anaesthesia exam
Reading File
Finding Sources
Finding Sources
Searching PubMed
"awareness under anesthesia" AND "prevention"
Finding Sources
Finding Sources
Searching PubMed
"bispectral index" AND "depth of anesthesia" AND monitoring
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Awareness Under Anaesthesia - A Comprehensive Review for MD Anaesthesia
1. DEFINITIONS AND TERMINOLOGY
Awareness under anaesthesia refers to a state in which the patient regains some degree of consciousness during a general anaesthetic and retains a memory of intraoperative events.
Key definitions (Miller's Anesthesia, 10e):
| Term | Definition |
|---|---|
| Awareness with Recall (AWR) | Subjective intraoperative experience with explicit episodic memory - the classic, clinically significant form |
| Wakefulness without recall | Patient is awake/responsive but has no memory (due to amnesia) |
| Implicit memory | Memory that influences behaviour without conscious recollection |
| Connected consciousness | Awareness of the environment or one's own body (extero/interoception) |
| Disconnected consciousness | Dreaming - internal experience not connected to outside world |
| Intraoperative dreaming | Drug-induced endogenous experience; not considered true awareness |
The clinical states during general anaesthesia are best illustrated by the Venn diagram from Miller's (Fig. 36.1):
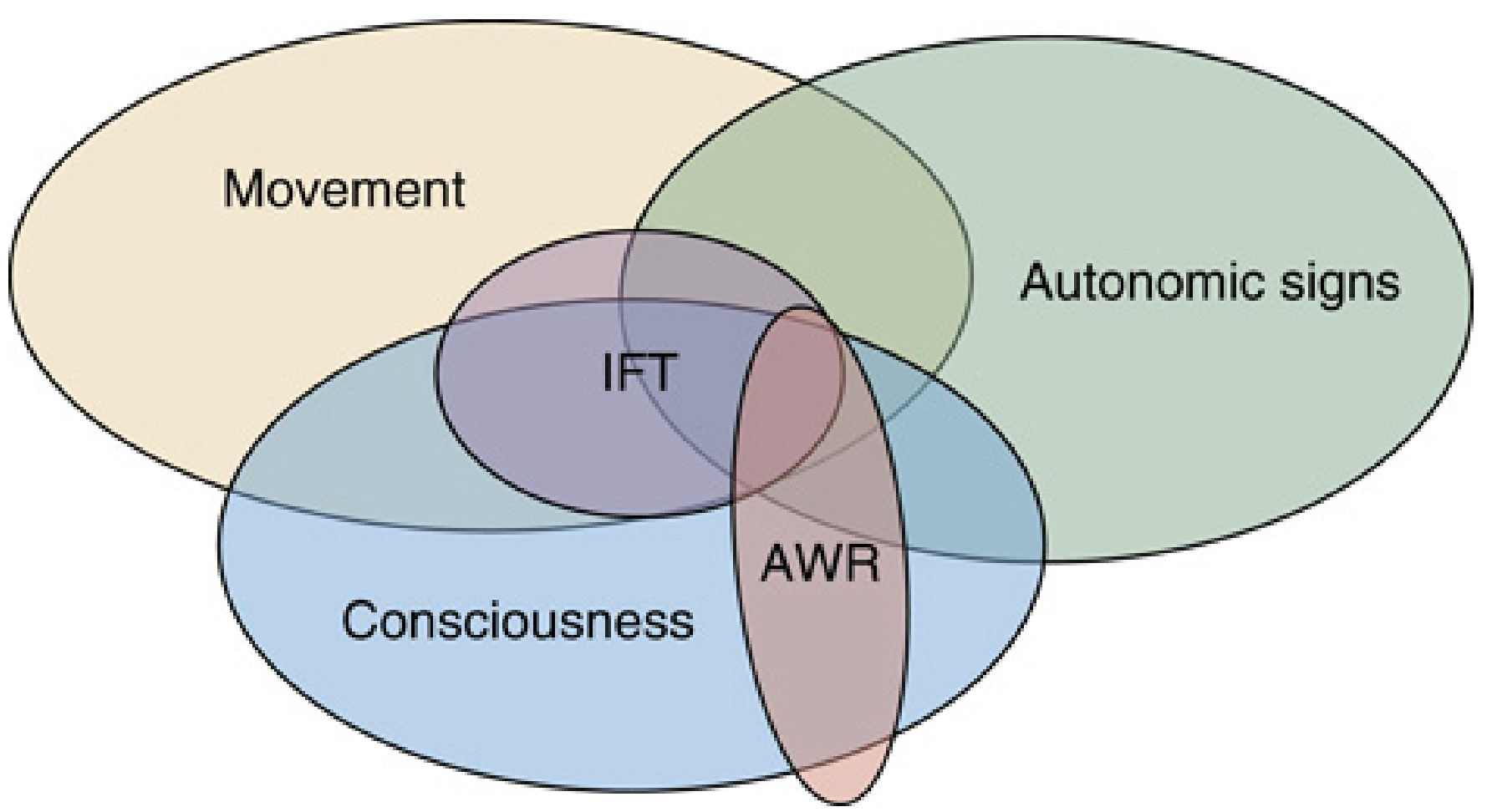
Movement and autonomic signs are unreliable indicators of consciousness - the three circles are largely non-overlapping.
2. INCIDENCE
- Overall incidence: 1 in 19,000 general anaesthetics (increasing to 1 in 8,000 for caesarean delivery) - Miller's Anesthesia, 10e
- Major trauma surgery: up to 43% in older series
- Cardiac surgery: 1.5%
- Caesarean section: 0.4%
- Approximately 2% of ASA Closed Claims relate to awareness under anaesthesia
- Morgan & Mikhail's, 7e: 79 awareness claims were filed in the ASA database up to 1999, with another 71 appearing subsequently
3. RISK FACTORS FOR AWARENESS
Patient-Related
- Previous history of awareness (strongest predictor)
- Female sex
- Morbid obesity (increased drug requirements)
- Chronic substance abuse / opioid tolerance / benzodiazepine tolerance
- Difficult airway (distraction during prolonged intubation)
- ASA physical status IV-V
Surgery-Related
- Major trauma (limited haemodynamic reserve restricts dose)
- Cardiac surgery (deliberate light anaesthesia for haemodynamic stability)
- Caesarean section (foetal concerns limit agent use)
- Rigid bronchoscopy (inhalational agent difficult to deliver)
- Emergency surgery
Anaesthetic Technique-Related
- Total intravenous anaesthesia (TIVA) - no end-tidal agent monitoring
- Neuromuscular blockade (abolishes motor responses that signal awakening)
- Vaporiser malfunction / empty vaporiser
- IV line disconnection / failure
- Inadequate pre-oxygenation leading to rush during induction
- Drug labelling errors (e.g., NMB given before induction)
- Nitrous oxide / oxygen technique without volatile agent
4. PRESENTATION AND SEQUELAE
Intraoperative Signs (unreliable with NMBDs)
- Purposeful movement
- Tachycardia, hypertension, sweating, lacrimation
- Dilated pupils, breath-holding
Postoperative Symptoms
- Explicit recall of intraoperative events (pain, paralysis, conversations)
- Anxiety, nightmares, sleep disturbances
- Post-Traumatic Stress Disorder (PTSD) - the most serious long-term consequence
- Social difficulties and avoidance behaviours
- Morgan & Mikhail's, 7e: Symptoms range from mild anxiety to full PTSD
5. MONITORING DEPTH OF ANAESTHESIA
5A. Clinical Signs (Guedel's and Modern Modifications)
The traditional Guedel stages apply only to ether in spontaneously breathing patients. In modern multimodal anaesthesia, the following are used:
| Sign | Limitation |
|---|---|
| Somatic movement | Abolished by NMBDs |
| Haemodynamic response (HR, BP, sweating) | Non-specific; influenced by vasopressors, beta-blockers |
| Brainstem reflexes (lacrimation, pupil size, corneal reflex) | Can persist even with awareness; abolished by topical agents |
| Respiratory pattern | Controlled ventilation makes this useless |
Key Point: These clinical signs are unreliable indicators of consciousness - the main impetus for neuromonitoring technology. - Miller's Anesthesia, 10e
5B. Isolated Forearm Technique (IFT)
- First described by Tunstall in 1977 for caesarean section
- A tourniquet or BP cuff is inflated to 200 mmHg on the arm before NMB administration, preserving neuromuscular function in the isolated limb
- Allows purposeful motor responses to commands: "If you can hear me, open and close your fingers"
- Cuff must be released within 30 minutes to prevent ischaemia
- Considered the gold standard for detecting intraoperative consciousness but remains largely a research tool
- IFT detects connected consciousness - responses are NOT usually associated with explicit memory formation
- Miller's, 10e: IFT likely underestimates true consciousness frequency due to lack of volition and partial consciousness
5C. EEG-Based Monitoring
Principles of EEG During Anaesthesia
As the patient transitions from awake to anaesthetised:
- Awake: Low amplitude, high frequency (beta/gamma, ~5-10 μV)
- Mild sedation: Beta oscillations appear ("beta buzz," 12-30 Hz) - excitatory phase
- Loss of responsiveness: Frontal alpha anteriorization (8-12 Hz moves from occipital to frontal)
- Surgical anaesthesia: Alpha + delta pattern ("alpha-delta EEG")
- Deep anaesthesia: Delta dominance, alpha peak frequency slows below 10 Hz
- Overdose: Burst suppression
Drug-Specific EEG Patterns (Miller's, 10e):
- Volatile agents (sevoflurane, isoflurane, desflurane): Progressive shift from alpha to delta, burst suppression at high doses; sevoflurane/enflurane can cause epileptiform spikes
- Propofol: More pronounced narrowband alpha and delta oscillations; alpha peak stays above 10 Hz
- Ketamine/N2O: Activation patterns - EEG may show HIGH frequency activity; EEG indices unreliable for these agents
- Dexmedetomidine: Spindle activity similar to natural sleep
EEG Index Monitors (Table - Commercial Monitors)
| Monitor | Manufacturer | Signal | Range for Anaesthesia | Principle |
|---|---|---|---|---|
| BIS (Bispectral Index) | Aspect Medical Systems | Single-channel EEG | 40-60 | Weighted sum: alpha/beta ratio + bicoherence + burst suppression |
| PSI (Patient State Index) | Physiometrix PSA 400 | 4-channel EEG | 25-50 | Discriminant analysis of spectral variables, hemispheric synchrony |
| Narcotrend | Monitor-Tech, Germany | 1-2 channel EEG | Stage D2-C (index 40-60) | Discriminant analysis classifying EEG stages A (awake) to F (burst suppression) |
| Entropy (SE/RE) | Datex-Ohmeda, GE | Single-channel EEG | 40-60 | State Entropy (0-32 Hz) + Response Entropy (0-47 Hz, includes EMG) |
| AAI (A-Line ARX Index) | Danmeter, Denmark | Middle-latency AEP | 10-25 | Autoregressive model of auditory evoked potential; AAI >60 = awake |
| CSI (Cerebral State Index) | Danmeter, Denmark | Single-channel EEG | 40-60 | Non-linear combination of EEG spectral features |
Source: Morgan & Mikhail's Clinical Anesthesiology, 7e, Table 6-1
Bispectral Index (BIS) - In Detail
- Scale: 0 (isoelectric/brain dead) to 100 (fully awake)
- 40-60: Surgical anaesthesia (low probability of recall)
- 60-80: Sedation
- >80: Risk of awareness
- <40: Deep anaesthesia / burst suppression risk
- Derived from weighted sum of three EEG parameters:
- Relative alpha/beta frequency ratio
- Bicoherence (phase coupling between EEG components)
- Burst suppression ratio
- Limitations:
- Different individuals can become aware at BIS values 40-90
- Unreliable with ketamine, N2O (both produce high-frequency activity)
- EMG contamination falsely elevates BIS
- ECG artefact, electrocautery interference
- The B-Aware trial (2004, Myles et al.) showed BIS guidance reduced awareness in high-risk patients; however, the B-Unaware and BAG-RECALL trials showed BIS was NOT superior to ETAC (end-tidal anaesthetic agent concentration) monitoring
Spectral Entropy
- State Entropy (SE): Measures EEG in 0.8-32 Hz range (reflects cortical activity)
- Response Entropy (RE): Measures 0.8-47 Hz (includes EMG, detects responses)
- RE-SE difference: Increases when facial EMG activates (patient may be reacting to stimulus)
Middle Latency Auditory Evoked Potentials (MLAEPs)
- The Aa (A-line ARX) Index uses mid-latency AEPs (10-100 ms latency)
- May be a more sensitive indicator than BIS for anaesthetic depth
- Amplitude decreases and latency increases with deeper anaesthesia
- Morgan & Mikhail's, 7e: "Middle latency auditory EP may be a more sensitive indicator than BIS"
5D. End-Tidal Anaesthetic Concentration (ETAC) Monitoring
- Continuous measurement of exhaled volatile agent concentration
- MAC-awake (the concentration preventing response to verbal command) = ~0.3-0.4 MAC
- MAC (prevents movement to surgical stimulus) = 1.0 MAC
- MAC-awareness = ~0.6 MAC (prevents recall)
- Maintaining >0.6 MAC (or ETAC at age-adjusted MAC equivalent) is a simple, effective strategy
- The BAG-RECALL trial showed ETAC-guided anaesthesia was at least as effective as BIS in preventing awareness
5E. Pharmacokinetic-Pharmacodynamic (PK-PD) Modelling / TCI (Target-Controlled Infusion)
- Used in TIVA with propofol +/- remifentanil
- Plasma and effect-site concentration targeting using validated models (Schnider, Marsh for propofol)
- Maintains calculated effect-site concentrations above awareness thresholds
- Does not directly measure brain state - must be combined with EEG monitoring for best practice
6. RECENT ADVANCES IN MONITORING
6A. EEG Spectrogram (Density Spectral Array / DSA)
- Visual display of EEG power across frequencies over time - replaces the single BIS number with a full "fingerprint" of brain state
- Shows drug-specific signatures; allows detection of burst suppression, alpha shifts, etc.
- The NeuroSENSE and similar devices display raw EEG + spectrogram
- Miller's, 10e: "There is much more useful clinical information about the state of the brain in the EEG signal than can be captured by a single number"
6B. Multichannel EEG
- Single-channel frontal EEG misses posterior and inter-regional information
- Connectivity measures (phase amplitude coupling, coherence between brain regions) show stronger correlation with consciousness than single-channel power
- Phase-amplitude coupling can distinguish sedation from general anaesthesia
- Still largely investigational but gaining clinical traction
6C. EEG-Based Nociception Monitors
- Surgical Pleth Index (SPI) / ANI (Analgesia Nociception Index): Derived from heart rate variability to measure pain/nociception balance
- qCON / qNOX (Quantium Medical): Two separate indices for hypnosis and nociception
- Addresses the problem that existing EEG monitors measure hypnosis but NOT analgesia
6D. Novel Indices Under Investigation
- Lempel-Ziv complexity: Measures diversity of EEG patterns - decreases with deeper anaesthesia
- Permutation entropy and symbolic entropy
- Phase-amplitude coupling (PAC)
- Slow-wave activity saturation: Linked to functional imaging evidence of loss of thalamic activation
- Connectivity-based indices measuring inter-regional information flow
6E. Machine Learning Approaches
- Neural network-based classifiers trained on large EEG datasets to predict awareness
- Not yet in clinical practice but promising
7. PREVENTION OF AWARENESS UNDER ANAESTHESIA
7A. Pre-operative Strategies
- Identify at-risk patients during pre-anaesthetic assessment
- Informed consent - discuss the possibility of awareness in high-risk cases
- Consider benzodiazepine premedication (midazolam) in high-risk patients (provides amnesia)
- Scopolamine - potent amnesic; useful adjunct especially in cardiac surgery
7B. Equipment Checks
- Check vaporiser level and function before every case
- Ensure IV line patency and continuity before induction
- Verify correct labelling of syringes (prevent NMB before induction)
- Check anaesthesia machine breathing circuit integrity
7C. Intraoperative Strategies
ASA Task Force (2006) recommendations for high-risk patients:
| Strategy | Evidence |
|---|---|
| Ensure ETAC ≥0.7 MAC (age-adjusted) | Strong |
| Use EEG depth monitor (BIS 40-60) in TIVA or high-risk cases | Moderate |
| Use peripheral nerve stimulator for minimal necessary NMB | Strong |
| Supplement TIVA with volatile agent where possible | Moderate |
| Administer benzodiazepine or scopolamine if volatile agent cannot be used | Moderate |
| Document ETAC values and drug doses intraoperatively | Expert opinion |
| Consider IFT if intense NMB is essential | Research tool |
Practical checklist (Morgan & Mikhail's, 7e):
- Volatile agents at amnesia concentration (≥0.5-0.7 MAC) whenever possible
- If not possible: benzodiazepines OR scopolamine (or both)
- Peripheral nerve stimulator to guide NMB to minimum necessary dose
- Re-dose IV anaesthesia during long intubation attempts / bronchoscopy
- Titrate TCI propofol to appropriate effect-site concentration
- Check ETAC continuously and respond to falls
7D. Crisis Management - When Awareness is Suspected Intraoperatively
- Increase volatile agent / propofol dose immediately
- Administer IV benzodiazepine (midazolam) for amnesia
- Administer opioid if pain suspected
- Document the event meticulously
- Post-operative follow-up and counselling
7E. Postoperative Management of Confirmed Awareness
- Detailed debriefing of the patient's experience
- Empathetic discussion - acknowledge the event
- Answer all patient questions honestly
- Psychological counselling / psychiatry referral for PTSD
- Critical incident reporting
- Morgan & Mikhail's, 7e: "Most patients reporting awareness are dissatisfied with the manner in which their concerns are addressed" - proactive engagement is essential
8. KEY CLINICAL TRIALS
| Trial | Year | Finding |
|---|---|---|
| B-Aware (Myles et al.) | 2004 | BIS monitoring reduced awareness by 82% in high-risk patients (TIVA, LSCS, cardiac) |
| B-Unaware (Avidan et al.) | 2008 | BIS NOT superior to ETAC monitoring in preventing awareness |
| BAG-RECALL (Avidan et al.) | 2011 | ETAC monitoring as effective as BIS; confirmed ETAC as valid comparator |
| Michigan Awareness Control Study | 2011 | BIS guidance did not reduce awareness vs ETAC in unselected population |
| IFT studies (Sanders, Gaskell et al.) | 2017 | Frontal alpha-delta EEG does NOT preclude volitional response; IFT shows higher incidence of connected consciousness than AWR rates suggest |
9. SUMMARY TABLE: MONITORS AT A GLANCE
| Monitor | Type | Index Range for GA | Best for | Limitations |
|---|---|---|---|---|
| BIS | EEG (1-channel) | 40-60 | TIVA, propofol | Ketamine, N2O unreliable; EMG artifact |
| Entropy (SE/RE) | EEG + EMG | SE 40-60 | Volatile + TIVA | Similar to BIS; RE detects EMG |
| AAI (AEP) | Auditory EEP | 10-25 | Detecting subtle awareness | Technical complexity |
| PSI | EEG (4-channel) | 25-50 | Broader EEG view | Less validation data |
| ETAC monitor | Expired gas | MAC-equivalent | Volatile GA | Not applicable for TIVA |
| IFT | Motor response | N/A (qualitative) | Gold standard detection | Research tool; limited duration |
| SPI/ANI | Autonomic/HRV | Agent-specific | Nociception monitoring | Does NOT measure hypnosis |
10. HIGH-YIELD EXAM POINTS
- AWR = Awareness WITH Recall - the clinically significant form; wakefulness without recall is more common but clinically under-recognized
- Overall incidence: 1:19,000; cardiac surgery: 1.5%; LSCS: 0.4%
- NMBDs are the biggest risk factor because they abolish motor signs that betray awakening
- BIS range for anaesthesia: 40-60; >60 = light, <40 = too deep
- IFT (Tunstall, 1977) - gold standard for detecting consciousness; tourniquet at 200 mmHg before NMB
- Brice Interview (5 questions) - standard tool for postoperative awareness assessment
- B-Aware showed BIS reduces awareness; but B-Unaware and BAG-RECALL showed ETAC monitoring is equally effective
- Ketamine and N2O increase EEG activity - BIS is unreliable with these agents
- PTSD is the most serious sequela
- Recent advances: spectrogram/DSA, multichannel EEG, nociception indices (ANI, SPI), Lempel-Ziv complexity, phase-amplitude coupling
Sources:
- Miller's Anesthesia, 2-Volume Set, 10e (Chapter 36: Consciousness, Memory, and Anesthesia)
- Morgan & Mikhail's Clinical Anesthesiology, 7e (Chapters 6 & 54)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
- Roche D, Mahon P. Depth of Anesthesia Monitoring. Anesthesiol Clin. 2021 [PMID: 34392880]
- Baron Shahaf D, Shahaf G. Intraoperative EEG-based monitors: are we looking under the lamppost? Curr Opin Anaesthesiol. 2024 [PMID: 38390951]
This is a shared conversation. Sign in to Orris to start your own chat.