Hepatic encephalopathy management
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-structured answer. Here it is:
Hepatic Encephalopathy: Management
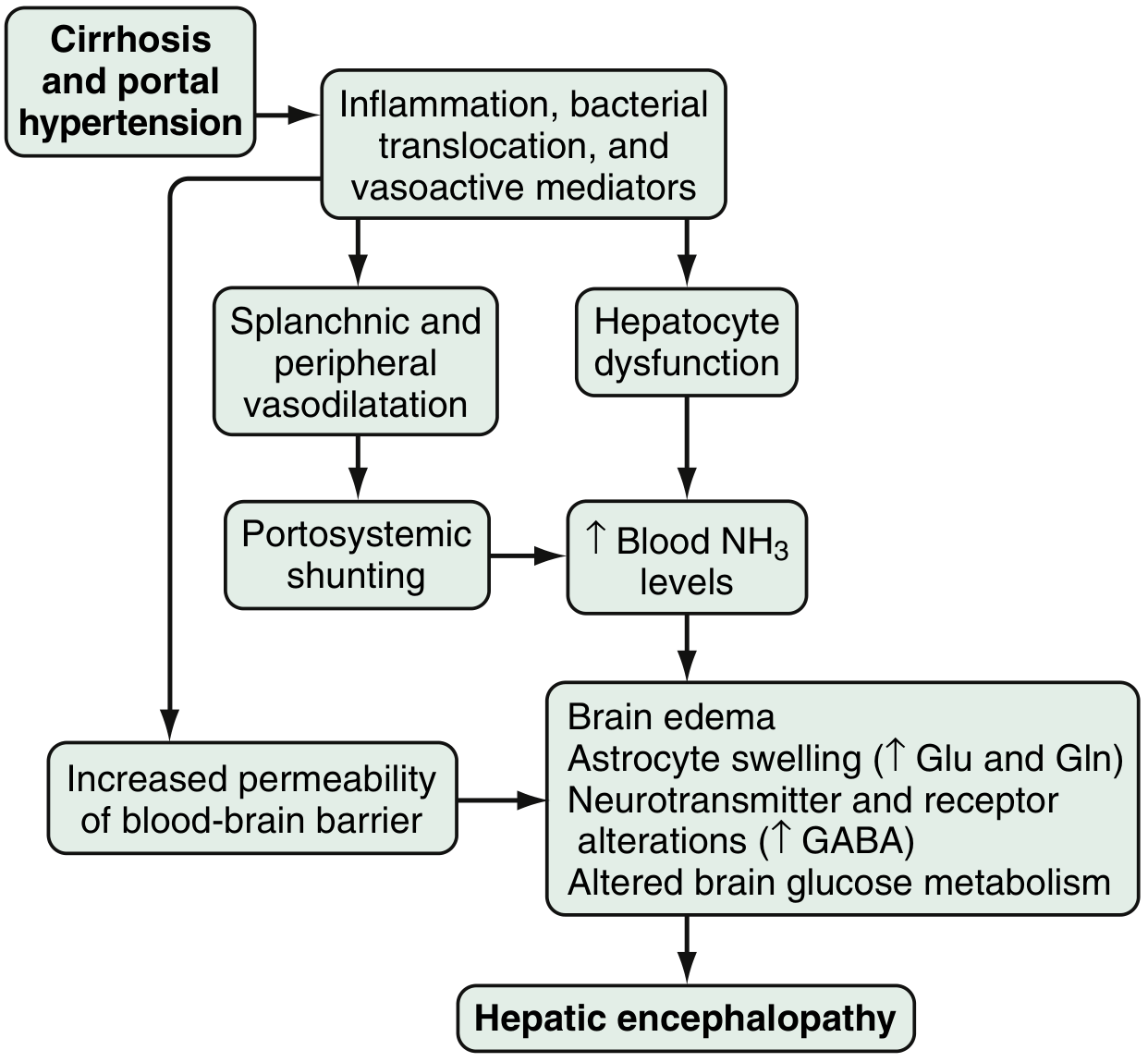
Pathophysiology (Brief)
HE arises primarily from ammonia accumulation caused by hepatocyte dysfunction and portosystemic shunting. Ammonia (produced by colonic bacteria metabolizing nitrogenous substrates and by enterocyte glutaminase) bypasses the liver and crosses an increasingly permeable blood-brain barrier, causing astrocyte swelling, GABA-ergic system upregulation, and altered brain metabolism.
Classification
Type by Underlying Disease
| Type | Mechanism |
|---|---|
| A | Acute liver failure (ALF) |
| B | Portosystemic bypass/shunting without intrinsic liver disease |
| C | Cirrhosis with portal hypertension (most common) |
Severity: West Haven Criteria + SONIC
| Grade | Consciousness | Clinical Symptoms | Neurologic Signs | SONIC Class |
|---|---|---|---|---|
| 0 | Normal | None | None | Unimpaired |
| Minimal | Normal | Normal | Abnormal neuropsych testing only | Covert HE |
| 1 | Sleep-wake reversal, restlessness | Forgetfulness, agitation, mild confusion | Tremor, incoordination | Covert HE |
| 2 | Lethargy, slow responses | Disorientation, inappropriate behavior | Asterixis, dysarthria, ataxia | Overt HE |
| 3 | Somnolence, confusion | Aggressive behavior | Asterixis, hyperreflexia, Babinski positive | Overt HE |
| 4 | Coma | Unresponsive | Decerebration | Overt HE |
Sleisenger and Fordtran's GI and Liver Disease, Table 94.1
Precipitating Factors (ALWAYS identify and treat)
- GI bleeding (most common)
- Infection (including SBP - perform paracentesis if ascites present)
- Electrolyte abnormalities: hypokalemia, alkalosis (from diuretics or diarrhea)
- Azotemia / dehydration
- High protein intake
- Constipation
- Medications: opioids, sedative-hypnotics, benzodiazepines
- TIPS placement or surgical portosystemic shunts
- Progressive hepatocellular dysfunction
- Lactulose non-compliance
Acute Episode Management (Overt HE)
Step 1 - Supportive Care
- Secure airway if Grade 3-4 (aspiration risk); ICU for Grade 3-4
- Correct electrolytes (especially K⁺, Na⁺, Mg²⁺)
- Monitor blood glucose; treat hypoglycemia
- Stop offending medications (opioids, benzodiazepines, diuretics in acute setting)
- Rule out structural causes if focal deficits present (head CT)
Step 2 - Identify and treat precipitant
- Blood cultures, urinalysis, diagnostic paracentesis (if ascites present)
- Treat infection aggressively; treat GI bleeding; correct coagulopathy
Step 3 - Reduce Ammonia
Lactulose (First-line)
- Mechanism: non-absorbable disaccharide - acidifies colon, traps NH₄⁺, cathartic effect, reduces urease-producing bacteria
- Dose: 15-45 mL PO bid-qid titrated to 2-3 soft stools per day (Goldman-Cecil) / 3-5 soft stools/day (Washington Manual)
- Acute phase: 30 mL every 1-2 hours initially, then taper as bowel movements occur
- If oral not tolerated: Lactulose enema (300 mL lactulose + 700 mL distilled water)
- Avoid if ileus or bowel obstruction
- Complications: hypovolemia, hypernatremia (monitor closely)
Rifaximin (Add-on / Second-line)
- Mechanism: minimally absorbed broad-spectrum oral antibiotic; reduces intestinal ammonia-producing bacteria
- Dose: 550 mg PO twice daily (evidence-based dose) or 400 mg PO every 8 hours
- Adding rifaximin to lactulose: complete reversal of HE 76% vs. 50.8% with lactulose alone; decreased mortality 23.1% vs. 49.1%
- Add when no improvement in first 24 hours of lactulose alone
- Mulholland & Greenfield's Surgery, p. 2893
Polyethylene Glycol (PEG)
- 4350-electrolyte solution: 4 L orally or via NG tube over 4 hours
- Goldman-Cecil notes this may lead to more rapid clinical response than lactulose alone - an emerging option for acute episodes
Pharmacotherapy Summary
| Agent | Dose | Role | Notes |
|---|---|---|---|
| Lactulose | 15-45 mL bid-qid PO; 300 mL enema | First-line | Titrate to 2-3 soft stools/day |
| Rifaximin | 550 mg PO bid | Add-on; prevention of recurrence | Preferred over neomycin |
| PEG 3350 | 4 L over 4h | Acute episodes | May act faster than lactulose |
| Neomycin | 500 mg-1 g TID | Alternative antibiotic | Falling out of favor - ototoxicity, nephrotoxicity |
| Metronidazole | 250 mg 2-4x/day | Alternative antibiotic | Risk of neurotoxicity |
| Branched-chain amino acids (BCAA) | IV infusion | Adjunct | Shown benefit without increased mortality |
| L-ornithine L-aspartate (LOLA) | Oral/IV | Investigational ammonia fixation | Under study |
| Glycerol phenylbutyrate | Oral | Investigational | Under study |
Secondary Prophylaxis (Prevention of Recurrence)
After any episode of overt HE, maintenance therapy is recommended indefinitely:
- Lactulose (primary) - titrated to 2-3 soft stools/day
- Add rifaximin 550 mg bid in patients with recurrent episodes (significantly reduces risk of recurrence and hospitalization in RCT)
- Can consider discontinuing only if precipitating factor is well controlled AND liver function/nutrition has improved
- Goldman-Cecil Medicine; Mulholland & Greenfield's Surgery
Dietary Considerations
- Do NOT restrict protein - protein restriction is harmful and not recommended chronically
- Target adequate protein intake (~1.2-1.5 g/kg/day)
- Switch from animal to vegetable source protein - may reduce ammonia generation in recurrent/persistent HE
- Small frequent meals; avoid prolonged fasting
- Late evening snack recommended (reduces catabolic state)
Management of Covert/Minimal HE
- Diagnosis: neuropsychological testing (abnormal in otherwise clinically normal patient)
- Treatment approach is still evolving
- Lactulose reduces progression to overt HE
- Rifaximin improves quality of life and driving performance in studies
- Probiotics have shown some benefit in trials
Special Situations
TIPS-associated HE
- Occurs in 10-50% post-TIPS
- Management: shunt reduction or occlusion may be required in refractory cases
- Rifaximin + lactulose as maintenance
HE in Acute Liver Failure (Type A)
- More likely to develop raised ICP and cerebral edema
- Osmotic therapy (mannitol 0.5-1 g/kg IV), head elevation
- Ammonia >150-200 µmol/L associated with cerebral herniation risk
- ICU management; consider liver transplant evaluation urgently
TIPS Insertion Prophylaxis
- Pre-TIPS lactulose/rifaximin may reduce post-TIPS HE incidence
Liver Transplantation
- Definitive treatment; generally reverses HE completely
- Refer for evaluation when HE occurs in context of decompensated cirrhosis
- Evaluate with Child-Pugh score ≥7 or MELD score ≥15
- Development of overt HE is a poor prognostic indicator: 1-year survival 20-42%, 3-year survival 15-23% without transplant
Diagnostic Pearls
- Ammonia level is neither sensitive nor specific - do not use to diagnose or grade HE
- EEG: slow, high-amplitude, triphasic waves (characteristic but non-specific)
- Asterixis (flapping tremor) present in Grades I-III (not Grade IV - coma)
- Always exclude: hypoglycemia, hyponatremia, intracranial hemorrhage, drug intoxication
Recent Evidence (2024-2026)
A fresh ACG Clinical Guideline on Hepatic Encephalopathy was published in March 2026 (PMID 41773757) - this is the most current North American practice guideline and likely refines recommendations around rifaximin, covert HE management, and newer ammonia-targeting agents. A 2025 meta-analysis also found PPI use increases HE risk in cirrhotic patients (PMID 40812534) - consider deprescribing PPIs where possible.
Key Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 94
- Goldman-Cecil Medicine International Edition, Chapter 139
- Washington Manual of Medical Therapeutics, Chapter (Hepatology)
- Mulholland & Greenfield's Surgery, Chapter (Liver Transplantation)
- Rosen's Emergency Medicine, Chapter 13
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Edition
- ACG Clinical Guideline (2026), PMID 41773757
This is a shared conversation. Sign in to Orris to start your own chat.