Top 10 heart disease and ecg report and ecg images
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram heart disease patterns
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
atrial fibrillation ECG rhythm strip
Searching Images
heart block bundle branch block ECG
Finding Sources
Searching Images
ventricular tachycardia ventricular fibrillation ECG
Searching Images
heart failure hypertensive heart disease ECG changes
Searching Images
pulmonary embolism right heart strain ECG
Searching Images
Wolff-Parkinson-White WPW syndrome delta wave ECG
Here is a comprehensive clinical report on the Top 10 Heart Diseases with ECG Findings and Images.
Top 10 Heart Diseases: ECG Report with Images
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Overview: Acute occlusion of a coronary artery causing transmural myocardial injury. The LAD artery territory (anterior STEMI) is the most common and most lethal.
ECG Findings:
| Feature | Description |
|---|---|
| ST Elevation | ≥1 mm in ≥2 contiguous limb leads; ≥2 mm in ≥2 contiguous precordial leads |
| Morphology | Convex (tombstone) or concave ST elevation |
| Reciprocal changes | ST depression in opposite leads |
| Hyperacute T waves | Tall, peaked T waves (early phase) |
| Pathological Q waves | Develop within hours–days (necrosis marker) |
| Location | Anterior (V1–V4): LAD; Inferior (II, III, aVF): RCA; Lateral (I, aVL, V5–V6): LCx |
Anterior STEMI ECG:


2. 💔 Non-STEMI / Unstable Angina (ACS without ST Elevation)
Overview: Partial coronary occlusion or severe stenosis causing subendocardial ischemia. Includes Wellens' syndrome — a pre-infarction pattern warning of critical LAD stenosis.
ECG Findings:
| Feature | Description |
|---|---|
| ST Depression | Horizontal or downsloping ≥0.5 mm in ≥2 leads |
| T-wave inversion | Symmetrical, deep inversions (lateral leads common) |
| Wellens' Type A | Biphasic T-waves in V2–V3 |
| Wellens' Type B | Deep, symmetrical T-wave inversions in V2–V4 |
| No Q waves | (differentiates from completed infarct) |
Wellens' Syndrome ECG (critical LAD stenosis):
3. ❤️🔥 Atrial Fibrillation (AF)
Overview: The most common sustained cardiac arrhythmia worldwide. Disorganized atrial electrical activity with irregular ventricular response. Major risk factor for stroke.
ECG Findings:
| Feature | Description |
|---|---|
| Rhythm | Irregularly irregular — hallmark finding |
| P waves | Absent; replaced by fibrillatory (f) waves |
| f waves | Fine, rapid oscillations (best seen in V1, II) |
| QRS | Narrow unless aberrant conduction or BBB |
| Rate | Variable; can be bradycardic, normal, or rapid |
Classic Atrial Fibrillation ECG:
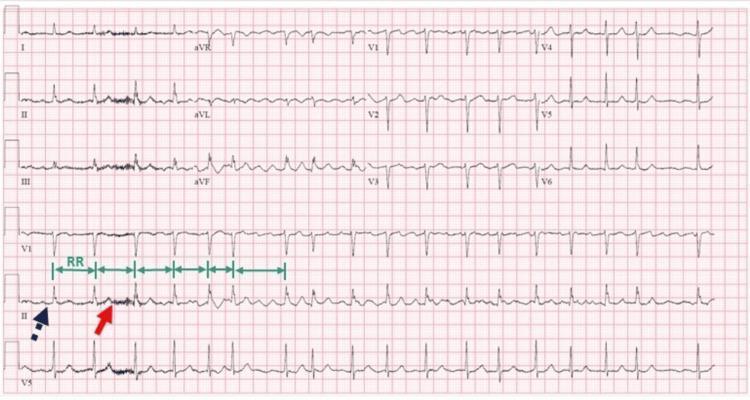
AF with complete AV block (regular rhythm paradox):
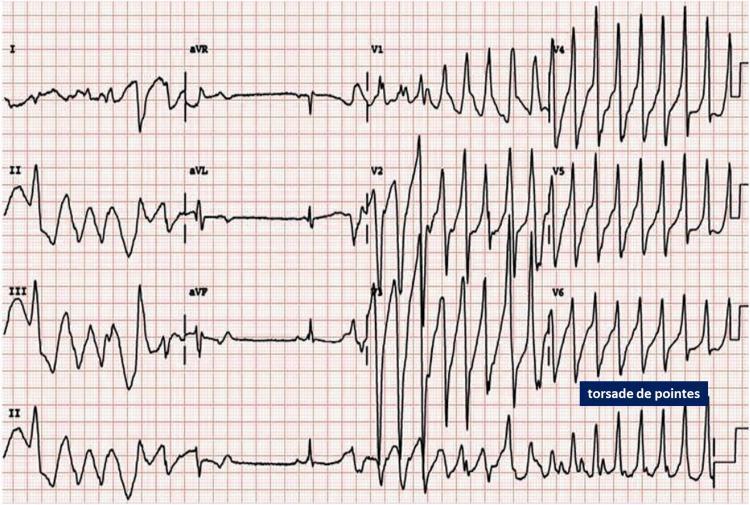
4. ⚡ Ventricular Tachycardia (VT) / Torsades de Pointes
Overview: Life-threatening arrhythmia originating in the ventricles. Torsades de Pointes is a polymorphic VT associated with prolonged QT interval.
ECG Findings:
| Feature | Description |
|---|---|
| Rate | >100 bpm (usually 140–200 bpm) |
| QRS | Wide (>120 ms), monomorphic or polymorphic |
| AV dissociation | P waves independent of QRS (if visible) |
| Fusion beats | Pathognomonic when present |
| Torsades | QRS amplitude "twists" around isoelectric baseline |
| Trigger | Preceded by short-long-short RR sequence in TdP |
Torsades de Pointes ECG:
5. 🧱 Left Bundle Branch Block (LBBB)
Overview: Conduction delay through the left bundle branch; always indicates significant cardiac disease. New LBBB + chest pain = STEMI equivalent (Sgarbossa criteria apply).
ECG Findings:
| Feature | Description |
|---|---|
| QRS Duration | ≥120 ms |
| Leads V1–V3 | Deep QS or rS complexes |
| Leads I, aVL, V5–V6 | Broad, notched R waves (no septal Q waves) |
| ST/T changes | Discordant (opposite to QRS direction) |
| Axis | Left axis deviation common |
Left Bundle Branch Block ECG:
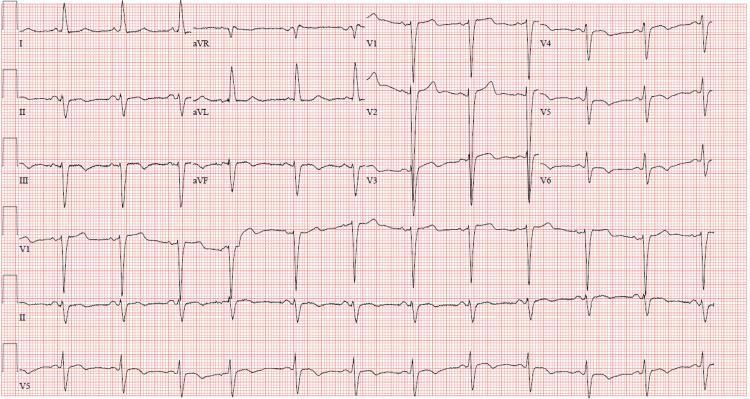
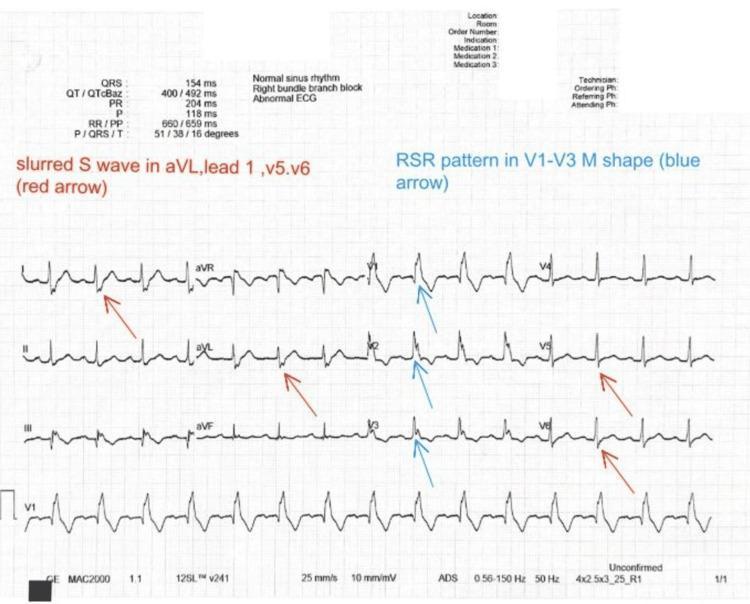
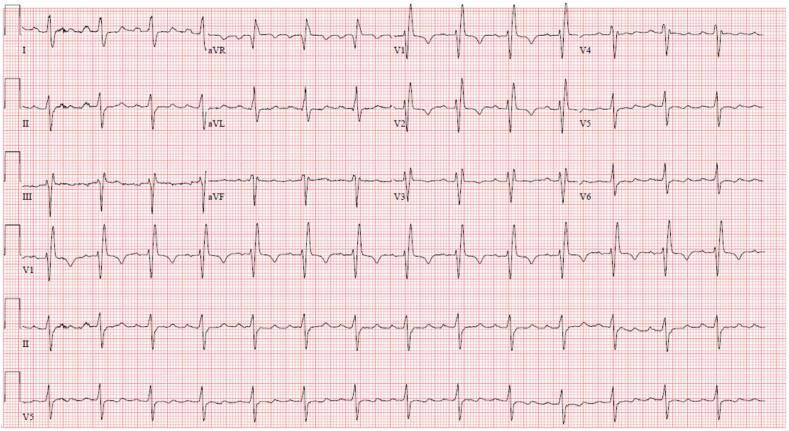
6. 🔀 Right Bundle Branch Block (RBBB)
Overview: Delayed right ventricular depolarization. Can be normal variant or indicate right heart strain, pulmonary embolism, or structural heart disease.
ECG Findings:
| Feature | Description |
|---|---|
| QRS Duration | ≥120 ms (complete); 100–120 ms (incomplete) |
| V1–V3 | rSR' pattern ("M-shaped" or "rabbit ears") |
| Leads I, aVL, V5–V6 | Broad, slurred S waves |
| ST/T | T-wave inversion in V1–V3 (secondary change) |
Right Bundle Branch Block ECG:
Bifascicular Block (RBBB + Left Anterior Fascicular Block):
7. 🚫 Complete (Third-Degree) AV Heart Block
Overview: Complete failure of AV conduction; atria and ventricles beat independently. Causes include ischemia (inferior MI most common), fibrosis, drugs, and Lyme disease.
ECG Findings:
| Feature | Description |
|---|---|
| P waves | Regular, independent of QRS |
| QRS | Slow escape rhythm (junctional: narrow 40–60 bpm; ventricular: wide <40 bpm) |
| PR interval | No fixed relationship (AV dissociation) |
| Rate | Ventricular rate 20–40 bpm (ventricular escape) |
Complete Heart Block + LBBB ECG:
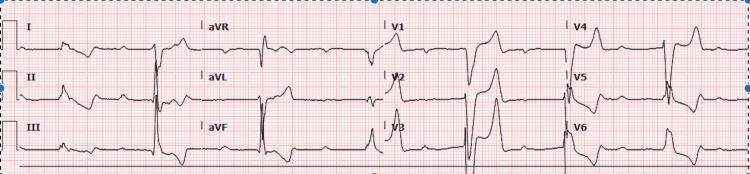
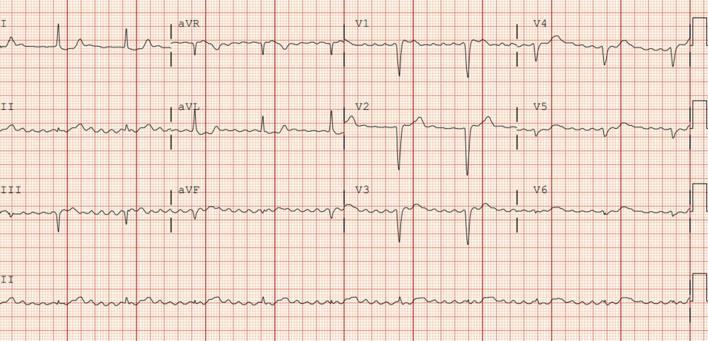
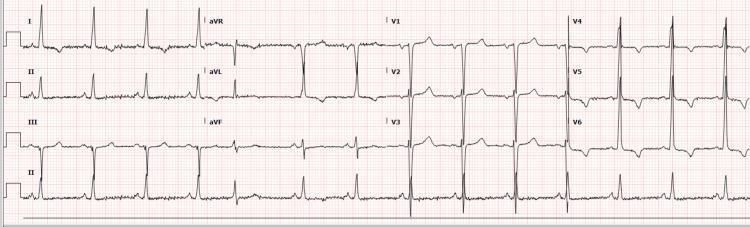
8. 🫁 Acute Pulmonary Embolism (Right Heart Strain)
Overview: Massive PE causes acute right ventricular pressure overload, producing characteristic ECG changes. ECG alone cannot diagnose PE but raises clinical suspicion.
ECG Findings:
| Feature | Description |
|---|---|
| S1Q3T3 | S wave in I, Q wave + T inversion in III |
| Sinus tachycardia | Most common finding |
| Right axis deviation | Acute RV pressure overload |
| Incomplete/Complete RBBB | RV conduction delay |
| T-wave inversions | V1–V4 (right precordial strain pattern) |
| P pulmonale | Peaked P waves in II (RAE) |
Acute PE with S1Q3T3 pattern:

PE with sinus tachycardia, S1Q3T3 and incomplete RBBB:

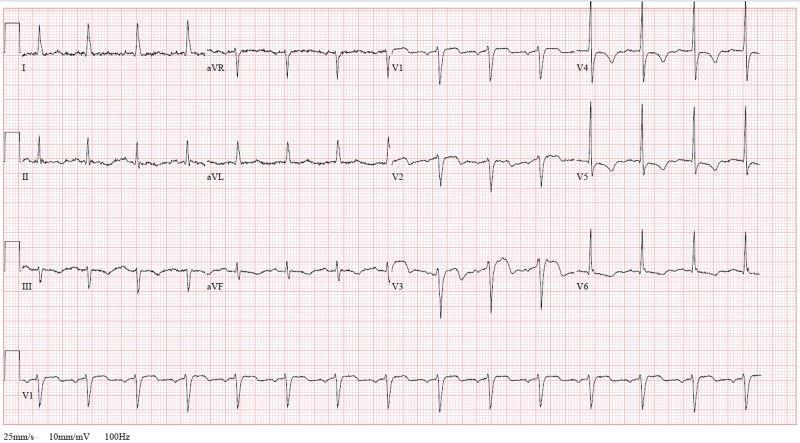
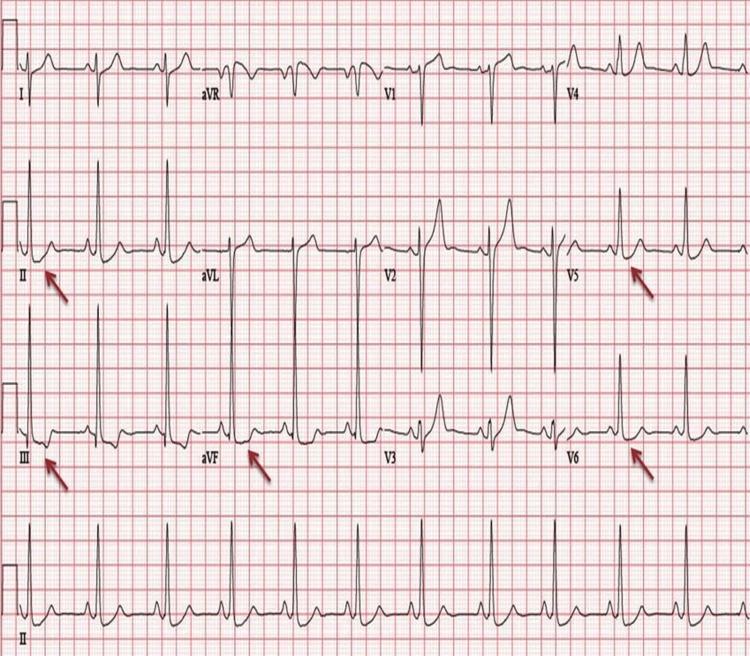
9. 🔋 Left Ventricular Hypertrophy (LVH) / Hypertensive Heart Disease
Overview: Chronic pressure overload (hypertension, aortic stenosis) causes LV wall thickening with characteristic voltage and strain changes on ECG.
ECG Findings:
| Feature | Description |
|---|---|
| High voltage | Sokolow-Lyon: S(V1) + R(V5 or V6) ≥35 mm |
| Strain pattern | ST depression + T-wave inversion in lateral leads (I, aVL, V5–V6) |
| Left axis deviation | Common |
| QRS duration | Mildly prolonged |
| Cornell criteria | R(aVL) + S(V3) >20 mm (women) or >28 mm (men) |
LVH with Strain Pattern ECG:
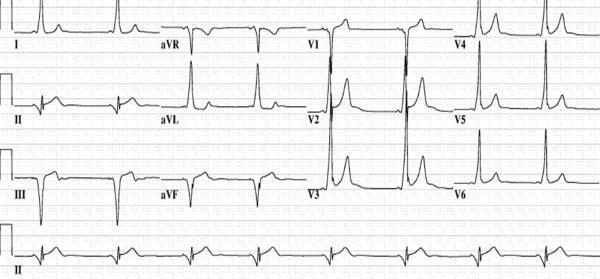
10. ⚡ Wolff-Parkinson-White (WPW) Syndrome
Overview: An accessory conduction pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Risk of sudden death if AF conducts rapidly via the accessory pathway.
ECG Findings:
| Feature | Description |
|---|---|
| Short PR interval | <120 ms (bypasses AV node delay) |
| Delta wave | Slurred upstroke at start of QRS |
| Wide QRS | >120 ms (fusion of normal + pre-excitation) |
| Secondary ST/T changes | Discordant, secondary to altered depolarization |
| Pathway localization | Delta wave polarity in V1/inferior leads identifies location |
WPW Syndrome ECG – Classic Triad:

Quick Reference Summary Table
| # | Condition | Key ECG Finding | Emergency? |
|---|---|---|---|
| 1 | STEMI | ST elevation ≥2 leads, reciprocal changes | 🔴 Yes – cath lab activation |
| 2 | NSTEMI/Unstable Angina | ST depression, T inversion, Wellens' pattern | 🟠 Urgent |
| 3 | Atrial Fibrillation | Irregularly irregular, no P waves | 🟡 Rate control / anticoagulation |
| 4 | VT / Torsades | Wide-complex tachycardia, twisting QRS | 🔴 Cardioversion / defibrillation |
| 5 | LBBB | Wide QRS, broad R in I/V6, QS in V1–V3 | 🟠 New onset = STEMI equivalent |
| 6 | RBBB | rSR' in V1, slurred S in I/V6 | 🟡 Context dependent |
| 7 | Complete Heart Block | AV dissociation, slow escape rhythm | 🔴 Pacemaker |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tach, RV strain | 🔴 Anticoagulation / thrombolysis |
| 9 | LVH / Hypertensive HD | High voltage + strain pattern | 🟡 BP control |
| 10 | WPW Syndrome | Short PR, delta wave, wide QRS | 🟠 Ablation indicated |
Clinical note: ECG interpretation must always be integrated with clinical history, symptoms, and other investigations. A normal ECG does not exclude significant heart disease.
This is a shared conversation. Sign in to Orris to start your own chat.