Heart failure
Reading File
Asking for Preferences
Based on Davidson latest edition
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the key content needed for a comprehensive answer. Let me compile everything.
Note: Davidson's Principles and Practice of Medicine is not available in the textbook library. The answer below is drawn from Braunwald's Heart Disease (the definitive cardiology reference) which covers the same material in greater depth.
Heart Failure - Braunwald's Heart Disease
Definition
Heart failure (HF) is a complex clinical syndrome resulting from structural and functional impairment of ventricular filling or ejection of blood. Most patients have myocardial impairment ranging from normal ventricular size and function to marked dilation with severely reduced function. The term "congestive HF" is no longer preferred because many patients do not have overt congestion at evaluation - their symptoms may instead reflect reduced cardiac output.
- Braunwald's Heart Disease, p. 933
Epidemiology
- Worldwide, HF affects nearly 23 million people
- In the US, 6.2 million adults have HF; prevalence is projected to rise 46% by 2030
- Prevalence rises exponentially with age - affects 4-8% of people over 65 years
- Lifetime risk for a 40-year-old is approximately 1 in 5
- Age-adjusted incidence is highest in Black men > Black women > White men > White women
- ~30-40% of non-ischemic HF is attributable to genetic factors
Types / Classification by Ejection Fraction
| Type | EF | Description |
|---|---|---|
| HFrEF (reduced) | < 40% | Dilated ventricle, systolic dysfunction |
| HFmrEF (mildly reduced) | 40-49% | "Borderline" or "mid-range" |
| HFpEF (preserved) | ≥ 50% | Diastolic dysfunction, normal or near-normal systolic function |
| HFrecEF (recovered) | Previously reduced, now improved | GDMT should be continued despite improved EF due to ~44% risk of recurrence on cessation |
The distribution of EF across unselected HF populations is bimodal with peaks at ~35% and ~55%.
ACC/AHA Staging vs. NYHA Classification
| ACC/AHA Stage | Description | NYHA Class |
|---|---|---|
| A | High risk for HF, no structural disease, no symptoms | None |
| B | Structural heart disease, no signs/symptoms | I |
| C | Structural heart disease + prior or current HF symptoms | I, II, III |
| D | Refractory HF requiring specialized interventions | IV |
NYHA Functional Classes:
- I - No limitation; ordinary activity does not cause symptoms
- II - Slight limitation; ordinary activity causes symptoms
- III - Marked limitation; less than ordinary activity causes symptoms; comfortable at rest
- IV - Symptoms at rest; any physical activity causes discomfort
Pathophysiology
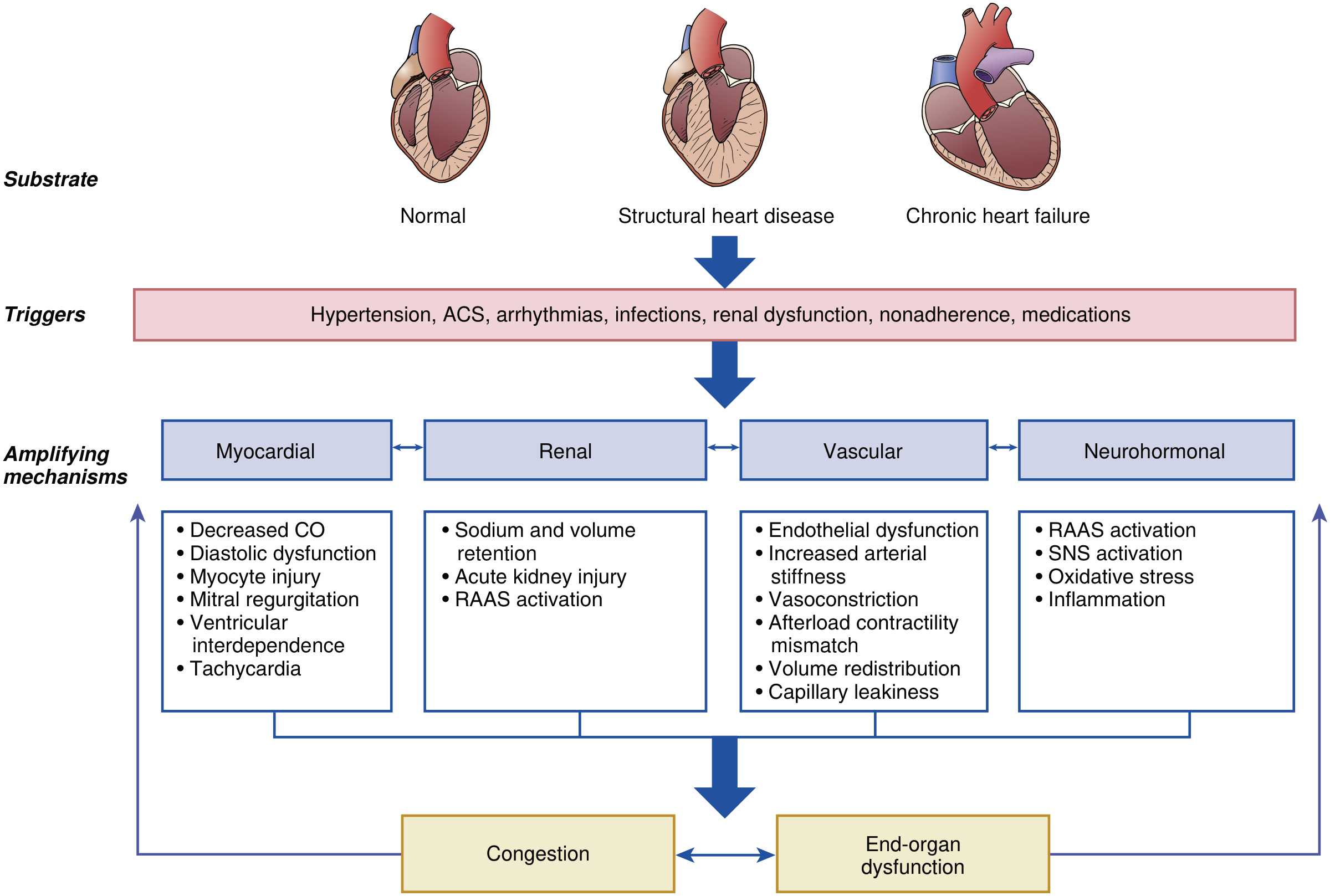
Decompensation occurs when a trigger acts on a susceptible substrate (normal heart, structural heart disease, or chronic HF):
Triggers: Hypertension, ACS, arrhythmias, infections, renal dysfunction, medication non-adherence, NSAIDs, thiazolidinediones
Four amplifying mechanisms perpetuate decompensation:
- Myocardial - Decreased CO, diastolic dysfunction, myocyte injury, mitral regurgitation, tachycardia
- Renal - Sodium and volume retention, acute kidney injury, RAAS activation
- Vascular - Endothelial dysfunction, increased arterial stiffness, vasoconstriction, volume redistribution, capillary leakiness
- Neurohormonal - RAAS activation, sympathetic nervous system (SNS) activation, oxidative stress, inflammation
These lead to two endpoints: Congestion and End-organ dysfunction (which feed each other in a vicious cycle).
Key concept: Clinical vs. Hemodynamic Congestion
- Hemodynamic congestion = elevated ventricular diastolic pressures without overt clinical signs - precedes clinical presentation
- Clinical congestion may resolve with diuretics, but hemodynamic congestion may persist, driving rehospitalization
- Chronically elevated filling pressures cause wall stress, RAAS/SNS activation, myocyte loss, fibrosis, and ventricular remodeling - each hospitalization worsens long-term prognosis
Clinical Features
Symptoms
- Dyspnea (on exertion, orthopnea, paroxysmal nocturnal dyspnea)
- Fatigue and weakness
- Ankle swelling / peripheral edema
- Exercise intolerance
- Bendopnea (dyspnea when bending forward - relatively specific for elevated filling pressures)
Physical Examination Findings
- Elevated JVP (jugular venous pressure)
- S3 gallop (ventricular filling sound) - highly specific for elevated filling pressures
- Pulmonary rales / crackles
- Pitting peripheral edema
- Displaced apex beat (cardiomegaly)
- Hepatomegaly / hepatojugular reflux
- Ascites (severe/right-sided HF)
- Sinus tachycardia (sympathetic activation)
- Low pulse pressure, cool extremities (low output states)
Diagnosis
The diagnosis depends on integration of history, physical examination, laboratory tests, cardiac imaging, and functional studies. No single sign or symptom defines HF. Diagnostic goals are to:
- Confirm HF is present
- Define the underlying cause
- Determine HFrEF vs. HFpEF
- Assess severity
- Identify comorbidities
Chest Radiography
- "Butterfly" pattern of interstitial and alveolar opacities (pulmonary edema)
- Kerley B lines - thin horizontal linear opacities at lung periphery (interstitial fluid)
- Peribronchial cuffing
- Prominent upper lobe vasculature (pulmonary venous hypertension)
- Pleural effusions
- Cardiomegaly
- Note: CXR may be clear even with significant dyspnea in advanced HF - negative predictive value is too low to exclude HF alone
ECG
- Sinus tachycardia (sympathetic activation - also a prognostic finding)
- Atrial arrhythmias (may be cause or consequence)
- LVH (increased QRS voltage)
- Q waves (ischemic etiology)
- Low QRS voltage (infiltrative disease, pericardial effusion)
- Prolonged PR (infiltrative cardiomyopathy, e.g. amyloidosis)
- LBBB (suggests cardiomyopathy; also eligibility for CRT if QRS ≥150 ms)
- Increased ventricular ectopy (risk marker for sudden death, especially EF <30%)
Natriuretic Peptides (BNP / NT-proBNP)
| Use | BNP | NT-proBNP |
|---|---|---|
| Exclude AHF | <30-50 pg/mL (NPV 96%) | <300 pg/mL (NPV 99%) |
| Rule in AHF (single cutoff) | >100 pg/mL | >900 pg/mL |
| Grey zone | 100-400 pg/mL | - |
| Definite AHF | >400 pg/mL | Age-stratified: <450 (<50 yr), <900 (50-75 yr), <1800 (>75 yr) |
Echocardiography
- Most important imaging test - determines EF, wall motion, valve function, diastolic parameters, pulmonary pressures, pericardium
- Lung ultrasound: B-lines indicate pulmonary congestion
Other Labs
- BMP/CMP (renal function, electrolytes - guide diuresis and GDMT)
- CBC (anemia as contributor)
- TFTs (thyroid dysfunction)
- LFTs (hepatic congestion, cardiogenic hepatopathy)
- Troponin (ongoing myocardial injury)
5-Year Outcomes
All three EF subtypes carry similar poor prognosis:
| Mortality | Readmission | Mortality/Readmission | |
|---|---|---|---|
| HFrEF | 75.3% | 82.2% | 96.4% |
| HFmrEF | 75.7% | 85.7% | 97.2% |
| HFpEF | 75.7% | 84.0% | 97.3% |
- Braunwald's Heart Disease, p. 104 (Shah KS et al. JACC 2017)
Risk Factors
- Ischemic heart disease / myocardial infarction
- Hypertension
- Diabetes mellitus
- Valvular heart disease
- Tachyarrhythmias
- Obesity
- Sleep apnea
- Excess alcohol or drug use
- Genetic cardiomyopathies (30-40% of non-ischemic HF)
- Medications: NSAIDs, thiazolidinediones, cancer chemotherapy
When to Refer for Advanced HF Therapies
Indications for advanced HF referral include: persistent NYHA Class III-IV despite optimal GDMT, recurrent hospitalizations, worsening renal function on titration, or consideration of cardiac transplantation or mechanical circulatory support (LVAD).
Source: Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, Chapter 48 - Heart Failure: Pathophysiology, Clinical Features, and Diagnosis, and Chapter 49 - Acute Heart Failure
This is a shared conversation. Sign in to Orris to start your own chat.