Teratoma of Testis -gross, microscopic features ; Seminoma - gross and microscopic features; Labelled diagram; Classical Seminoma - morphology, modes of spread Classify Testicular Tumors Teratoma - define, classify, Extragonadal sites of appearance ; Testicular Germ Cell Tumors - enumerate, describe any one ; Fibroid Uterus - gross, microscopic, complications ; Germ Cell Tumors of Ovary - classify, Dysgerminoma - gross, microscopic findings ; Teratoma - define, classify, Extragonadal sites of appearance; refer robbins 2nd yr mbbs pathology answer each question in detail add diagrams as well
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Here is the complete, detailed pathology answer covering all your questions, sourced directly from Robbins:
Pathology: Testicular & Ovarian Tumors + Fibroid Uterus
(Robbins Pathology - 2nd Year MBBS)
PART 1: CLASSIFICATION OF TESTICULAR TUMORS
WHO Classification
A. Germ Cell Tumors (95% of all testicular tumors; nearly all malignant)
I. Postpubertal type (derived from Germ Cell Neoplasia In Situ - GCNIS):
- Seminoma (~50%)
- Embryonal carcinoma
- Yolk sac tumor
- Choriocarcinoma
- Teratoma (malignant in adults)
- Mixed GCTs (~30-40%; most common: teratoma + embryonal carcinoma)
II. Spermatocytic tumor - distinct entity; NOT from GCNIS; older males (50-60 yrs); benign
III. Prepubertal type (NOT from GCNIS; benign behavior):
- Yolk sac tumor (most common in children <3 yrs)
- Teratoma (prepubertal; benign)
B. Sex Cord-Stromal Tumors (uncommon, usually benign):
- Leydig cell tumor, Sertoli cell tumor, Granulosa cell tumor
C. Mixed GCT-Sex Cord-Stromal: Gonadoblastoma
Summary Table of Testicular GCTs (Robbins & Kumar Basic Pathology, Table 16.1)
| Tumor | Peak Age | Morphology | Tumor Marker |
|---|---|---|---|
| Seminoma | 40-50 yrs | Sheets of uniform polygonal cells, clear cytoplasm; lymphocytes in stroma | hCG in 10% |
| Embryonal carcinoma | 20-30 yrs | Poorly differentiated pleomorphic cells; cords, sheets, papillae | AFP may be elevated |
| Spermatocytic tumor | 50-60 yrs | Small, medium, large polygonal cells; no inflammatory infiltrate | Negative |
| Yolk sac tumor | <3 yrs | Schiller-Duval bodies; microcysts, reticular pattern | AFP in 90% |
| Choriocarcinoma | 20-30 yrs | Cytotrophoblast + syncytiotrophoblast; no villus formation | hCG in 100% |
| Teratoma | All ages | Tissues from all 3 germ layers, varying differentiation | AFP in 20-25% |
| Mixed GCT | 15-30 yrs | Variable; depends on mixture | AFP + hCG variably elevated |
PART 2: SEMINOMA - GROSS AND MICROSCOPIC FEATURES + MORPHOLOGY + MODES OF SPREAD
Classical Seminoma - Pathogenesis
- Most common testicular GCT (~50% of all testicular GCTs)
- Virtually all arise from Germ Cell Neoplasia In Situ (GCNIS)
- Nearly all have isochromosome 12p [i(12p)] - extra copies of chromosome 12p short arm
- KIT oncogene mutations in up to 25%
- Risk factors: cryptorchidism (10% of cases), intersex syndromes, family history
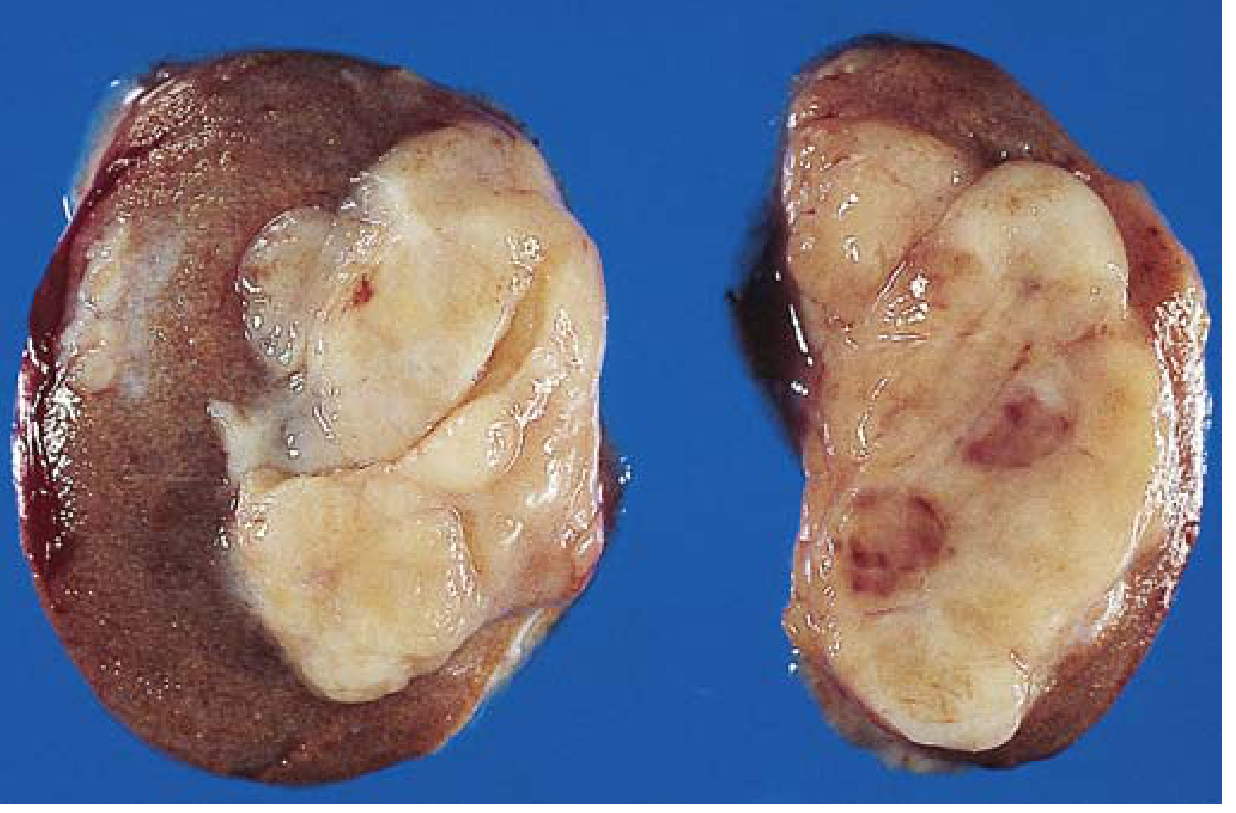
GROSS FEATURES
- Soft, well-demarcated, lobulated gray-white homogeneous tumor
- Bulges prominently from the cut surface of the affected testis
- "Fish flesh" or "fleshy" appearance
- No hemorrhage (unlike embryonal carcinoma - key distinguishing feature)
- Large tumors may show foci of coagulative necrosis
- May be very large at diagnosis (remains confined to testis for long periods)
MICROSCOPIC FEATURES
- Large, uniform, polygonal cells with distinct cell borders
- Clear, glycogen-rich cytoplasm (PAS positive)
- Round nuclei with coarsely clumped chromatin
- Conspicuous nucleoli (1-2 prominent nucleoli per cell)
- Cells arranged in small lobules separated by delicate fibrous septa
- Lymphocytic infiltrate in the stroma (hallmark - T lymphocytes)
- May elicit granulomatous reaction (epithelioid cells, giant cells)
- In ~15% of cases, syncytiotrophoblast cells present (source of mildly elevated hCG)
Labeled Diagram - Classical Seminoma Histology
CLASSICAL SEMINOMA - HISTOLOGICAL FEATURES
═══════════════════════════════════════════
┌──────────────────────────────────────────────────────┐
│ FIBROUS SEPTUM │
│ (divides tumor into lobules) │
│ Contains: Lymphocytes (•) + Granulomas [G] │
└──────────────────┬───────────────────────────────────┘
│
┌──────────────────▼───────────────────────────────────┐
│ LOBULE OF TUMOR CELLS │
│ │
│ ○ ── ○ ── ○ ── ○ ── ○ ── ○ ── ○ │
│ │ │ │ │ │ │ │ │
│ ○ ○ ○ ○ ○ ○ ○ │
│ │
│ ○ = Large polygonal tumor cell: │
│ - Distinct cell borders │
│ - CLEAR glycogen-rich cytoplasm (PAS+) │
│ - Round nucleus │
│ - 1-2 PROMINENT NUCLEOLI │
│ │
│ • = Lymphocytes in stroma (HALLMARK) │
│ [G] = Epithelioid granuloma │
│ *ST* = Syncytiotrophoblast (15% cases; hCG+) │
└──────────────────────────────────────────────────────┘
IHC: PLAP (+), OCT3/4 (+), D2-40 (+), CD117/KIT (+)
AFP (-), CD30 (-)
hCG: mildly elevated in 10-15% (stage I)
MODES OF SPREAD of Seminoma
1. Lymphatic spread (primary and early route):
- First drains to iliac and para-aortic (retroperitoneal) lymph nodes
- This reflects the embryologic origin of the testis from the retroperitoneum
- NOT to inguinal nodes (unless scrotal skin is invaded - scrotal nodes only if skin infiltrated)
- Predictable, stepwise lymphatic progression
2. Hematogenous spread (late in course):
- Occurs late - distinguishes seminoma from NSGCTs
- Common metastatic sites: lungs, liver, bone, brain
- Seminoma characteristically spreads hematogenously much later than embryonal carcinoma
3. Direct local spread:
- Late involvement of epididymis, spermatic cord
- Usually well-contained by tunica albuginea early on
Clinical significance: Seminoma spreads in a predictable, stepwise lymphatic pattern and is exquisitely sensitive to radiation therapy and platinum-based chemotherapy. Stage I disease has ~99% cure rate.
PART 3: TERATOMA - DEFINITION, CLASSIFICATION & EXTRAGONADAL SITES
Definition
A teratoma is a germ cell tumor in which neoplastic germ cells differentiate along multiple somatic (non-germ) cell lineages, producing tissues derived from two or more (usually all three) embryonic germ layers: ectoderm, mesoderm, and endoderm. Elements may be mature or immature.
Classification
A. By Age/Pathogenesis:
| Feature | Prepubertal (Pediatric) | Postpubertal (Adult) |
|---|---|---|
| Origin | NOT from GCNIS | From GCNIS |
| i(12p) | Absent | Present |
| Behavior | Benign | Malignant (regardless of maturity) |
| Pure form | Common in infants/children | Rare (2-3%); usually mixed |
B. By Degree of Differentiation (Histological Classification):
-
Mature teratoma - well-differentiated adult-type tissues
- In ovary ("dermoid cyst"): mainly ectodermal (skin, hair, teeth, sebaceous glands) - almost always benign
- In prepubertal testis: benign
- In postpubertal testis: still malignant despite mature appearance
-
Immature teratoma - embryonal/fetal-type tissues
- Most common immature element: primitive neuroepithelium
- Graded 0-3 (based on amount of immature neural tissue per slide)
- Grade 0 = all mature; Grade 3 = >2 low-power fields immature neuroepithelium per slide
- More aggressive - can metastasize
-
Teratoma with somatic-type malignancy (rare)
- A secondary non-germ cell malignancy arises within the teratoma
- Examples: squamous cell carcinoma, adenocarcinoma, rhabdomyosarcoma, PNET
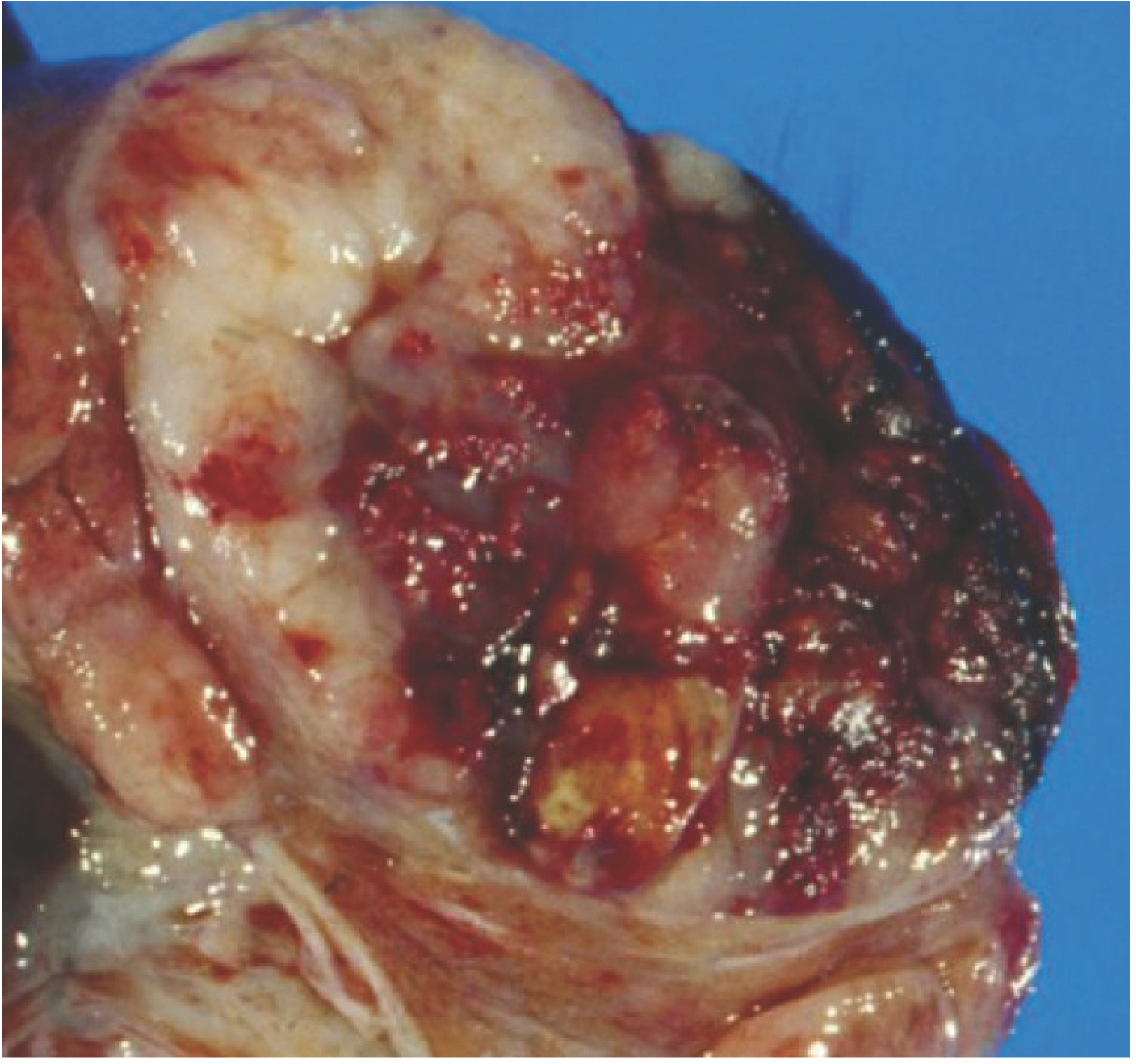
Gross Features of Testicular Teratoma
- Heterogeneous, variegated appearance - hallmark distinguishing from uniform seminoma
- Multiple cysts of varying sizes containing serous, mucinous, or sebaceous material, hair, teeth
- Solid areas with cartilage (white/grey), bone, or fibrous tissue
- Foci of hemorrhage and necrosis in postpubertal/malignant forms
Microscopic Features of Testicular Teratoma
- Tissues from all 3 germ layers in disorganized arrangement, embedded in fibrous/myxoid stroma:
- Ectoderm: Squamous epithelium, skin adnexa (sebaceous glands, hair follicles), neural tissue
- Mesoderm: Smooth/skeletal muscle bundles, islands of cartilage, bone, connective tissue
- Endoderm: Bronchial epithelium, intestinal wall structures, thyroid gland-like tissue, glandular epithelium
- Elements may be mature (adult-type) or immature (fetal-type)
Extragonadal Sites of Teratoma
Teratomas arise along the midline migration path of primordial germ cells (cranial to caudal):
EXTRAGONADAL TERATOMA SITES
(Midline migration path of primordial germ cells)
CRANIAL
│
[Intracranial] - Pineal gland, suprasellar region
│ (germinoma = seminoma equivalent in CNS)
│
[Anterior Mediastinum] - Most common ADULT extragonadal site
│ (50% of mediastinal GCTs)
│
[Retroperitoneum] - 2nd most common adult extragonadal site
│
[Sacrococcygeal] - Most common in NEONATES/infants
│ Most common solid tumor of newborns!
CAUDAL 4:1 female predominance
Other (rare): Neck, orbit, liver
Key facts:
- Sacrococcygeal teratoma - most common solid tumor of newborns; benign in neonates; malignant risk increases with age (if not excised early)
- Anterior mediastinal teratoma - most common in adults; right-sided; may be very large
- Intracranial teratoma - pineal region most common; may cause Parinaud syndrome
- Extragonadal teratomas arise because primordial germ cells migrate along the midline and may arrest at any site during migration
PART 4: TESTICULAR GERM CELL TUMORS - DESCRIBE ANY ONE (Seminoma, with full description above)
(See Part 2 for complete description of Seminoma)
All 7 GCT types enumerated in Table 16.1 above. For examination purposes, Seminoma is the most commonly asked "describe any one" GCT.
PART 5: FIBROID UTERUS (LEIOMYOMA) - GROSS, MICROSCOPIC, COMPLICATIONS
Definition
Uterine leiomyoma (fibroid) is a benign smooth muscle neoplasm of the uterus - the most common tumor in females.
Pathogenesis
- Most have normal karyotypes; ~40% have simple chromosomal abnormalities
- MED12 gene mutations (~70%) - encodes a component of the Mediator transcription complex
- Chromosomal rearrangements at 12q14 and 6p (HMGC/HMGIY genes)
- Associated with HLRCC syndrome (germline FH gene mutations)
GROSS FEATURES
- Sharply circumscribed, discrete, round, firm, gray-white tumors
- Multiple in most cases ("bag of worms" feel on palpation)
- Vary from tiny nodules to massive tumors filling the pelvis
- Locations in myometrium:
UTERINE LEIOMYOMA - LOCATIONS
══════════════════════════════
┌─────────────────────────────────────┐
│ [ENDOMETRIUM] │
│ ┌────┐ │
│ │(SM)│ SUBMUCOSAL │
│ └────┘ (causes most bleeding) │
│ ─────────────────────────────────── │
│ ┌──────────┐ ┌───┐ │
│ │ (IM) │ │(IM│ INTRAMURAL │
│ └──────────┘ └───┘ (most common)│
│ ─────────────────────────────────── │
│ [MYOMETRIUM] │
│ ┌──────────┐ │
│ │ (SS) │ SUBSEROSAL │
│ └────┬─────┘ │
│ │ pedunculated │
│ ─────┼───── SEROSA │
└──────────│─────────────────────────-┘
↓ (P) Pedunculated subserosal - can undergo torsion
- Cut section shows characteristic whorled pattern of smooth muscle bundles
- Large tumors show yellow-brown to red softening (degeneration)
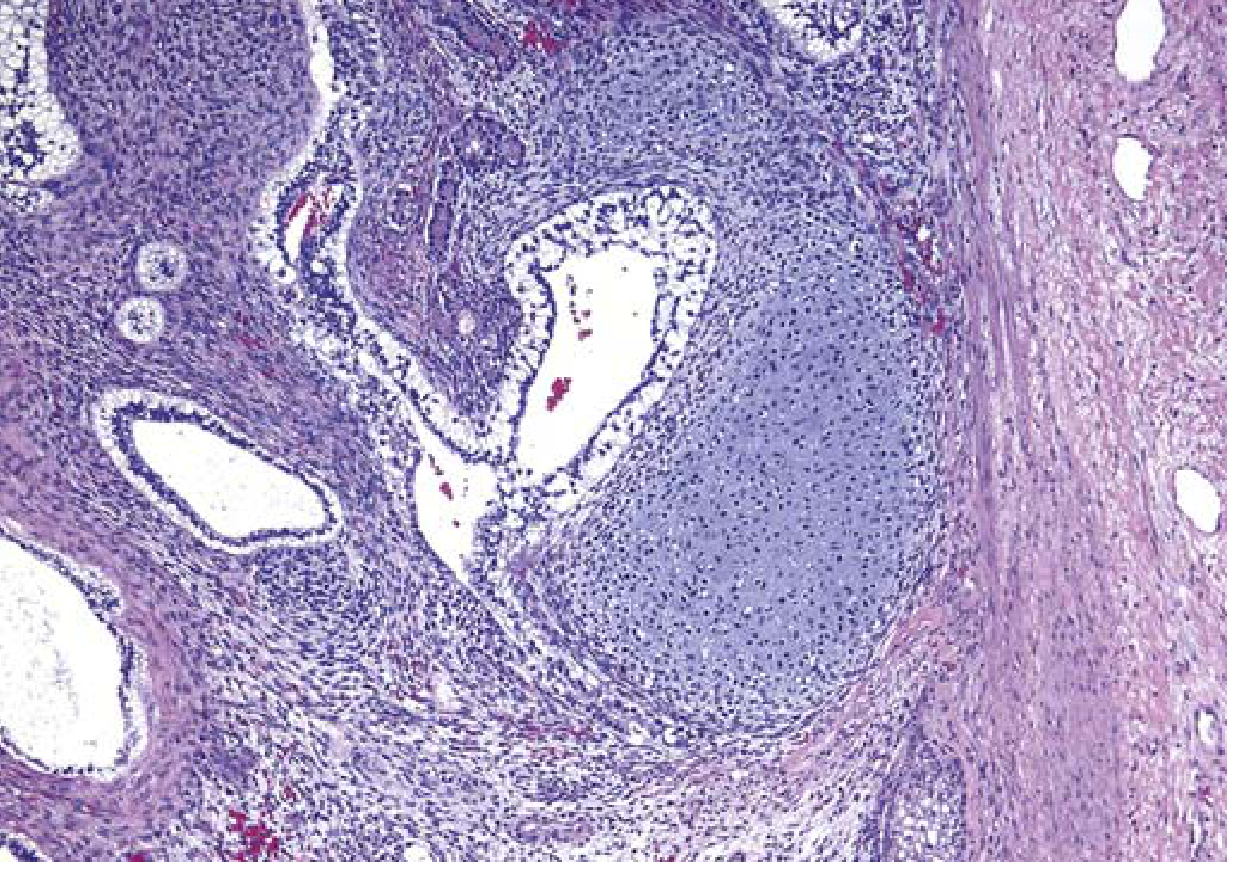
MICROSCOPIC FEATURES
- Bundles of smooth muscle cells resembling normal myometrium
- Cells uniform: oval "cigar-shaped" nuclei, long slender bipolar cytoplasmic processes
- Scarce mitotic figures (key feature - distinguishes from leiomyosarcoma)
- Sharp demarcation from surrounding myometrium (pseudo-capsule)
- Hyalinization common in older/larger tumors
COMPLICATIONS
Symptoms and local complications:
- Abnormal uterine bleeding (menorrhagia) - especially submucosal
- Urinary frequency / hydronephrosis from compression
- Pelvic pain and pressure
- Infertility (distortion of endometrial cavity)
- Pedunculated tumors - torsion, ischemic necrosis
Degenerative changes (complication of growth):
- Hyaline degeneration - most common; replacement by collagen
- Cystic degeneration - liquefaction of hyalinized areas
- Carneous (Red) degeneration - infarction with hemolysis; especially in pregnancy (painful)
- Calcification - late, post-menopausal "womb stones"
- Fatty degeneration - rare
- Myxoid degeneration - gelatinous appearance
Pregnancy-related complications:
- Spontaneous abortion
- Fetal malpresentation
- Uterine inertia (failure to contract adequately during labor)
- Postpartum hemorrhage
Malignant transformation: Extremely rare; leiomyosarcomas arise de novo, not from fibroids
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p.937
PART 6: GERM CELL TUMORS OF OVARY - CLASSIFICATION + DYSGERMINOMA
Classification of Ovarian Germ Cell Tumors
| Category | Examples |
|---|---|
| Dysgerminoma | Malignant; most common malignant GCT |
| Teratoma | Mature (dermoid cyst - benign); Immature (malignant); Monodermal (struma ovarii, carcinoid) |
| Yolk Sac Tumor | Endodermal sinus tumor; AFP elevated |
| Embryonal Carcinoma | Rare |
| Choriocarcinoma (non-gestational) | Rare; hCG elevated |
| Mixed GCT | 2+ elements; most common: dysgerminoma + EST |
| Gonadoblastoma | In dysgenetic gonads; often with dysgerminoma |
PART 7: DYSGERMINOMA - GROSS AND MICROSCOPIC FEATURES
Epidemiology
- Most common malignant ovarian GCT (30-40%)
- 75% occur between ages 10-30 years; 5% before age 10; rare after 50
- 20-30% of ovarian malignancies in pregnancy are dysgerminomas
- Histologically identical to testicular seminoma and CNS germinoma
GROSS FEATURES
- Usually 5-15 cm in diameter
- Slightly bosselated (lobulated) capsule
- Cut surface: fleshy, pale tan to gray-brown
- Principally solid with some cystic areas and necrosis
- Usually unilateral (bilateral in 10-15%)
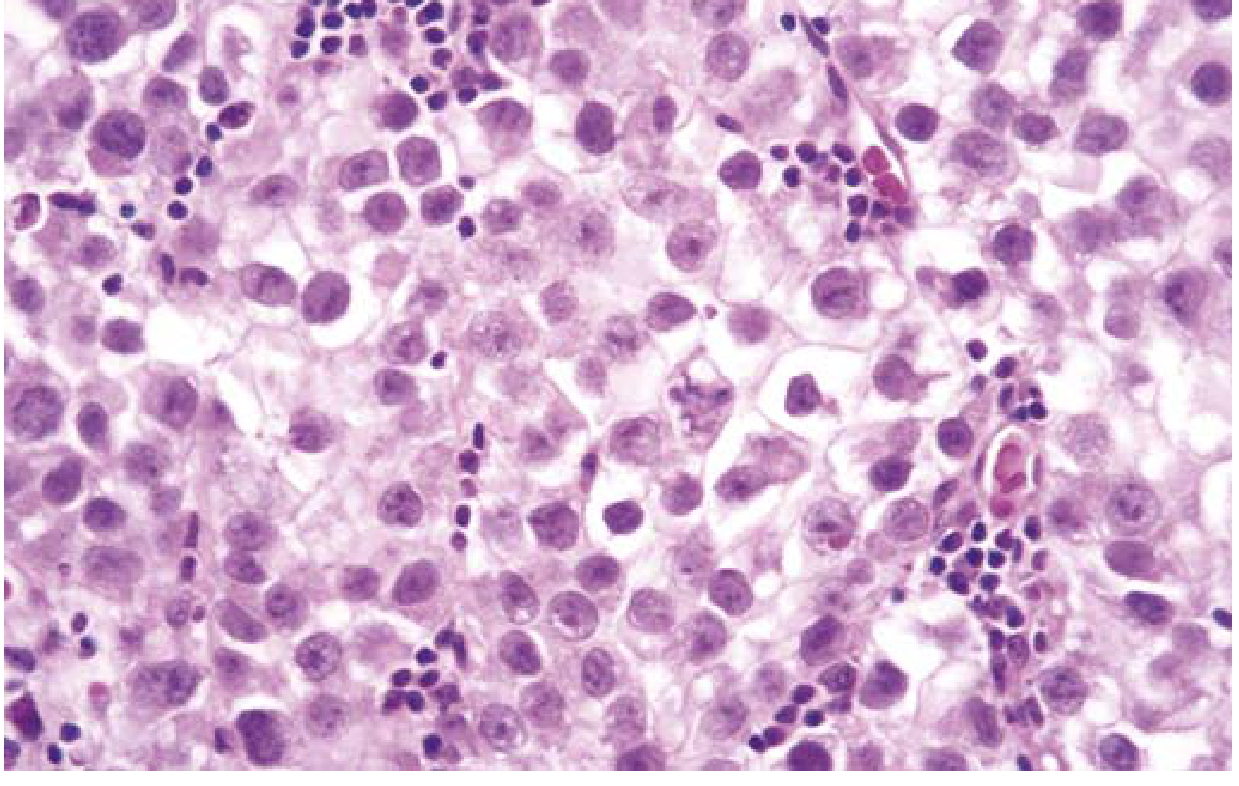
MICROSCOPIC FEATURES
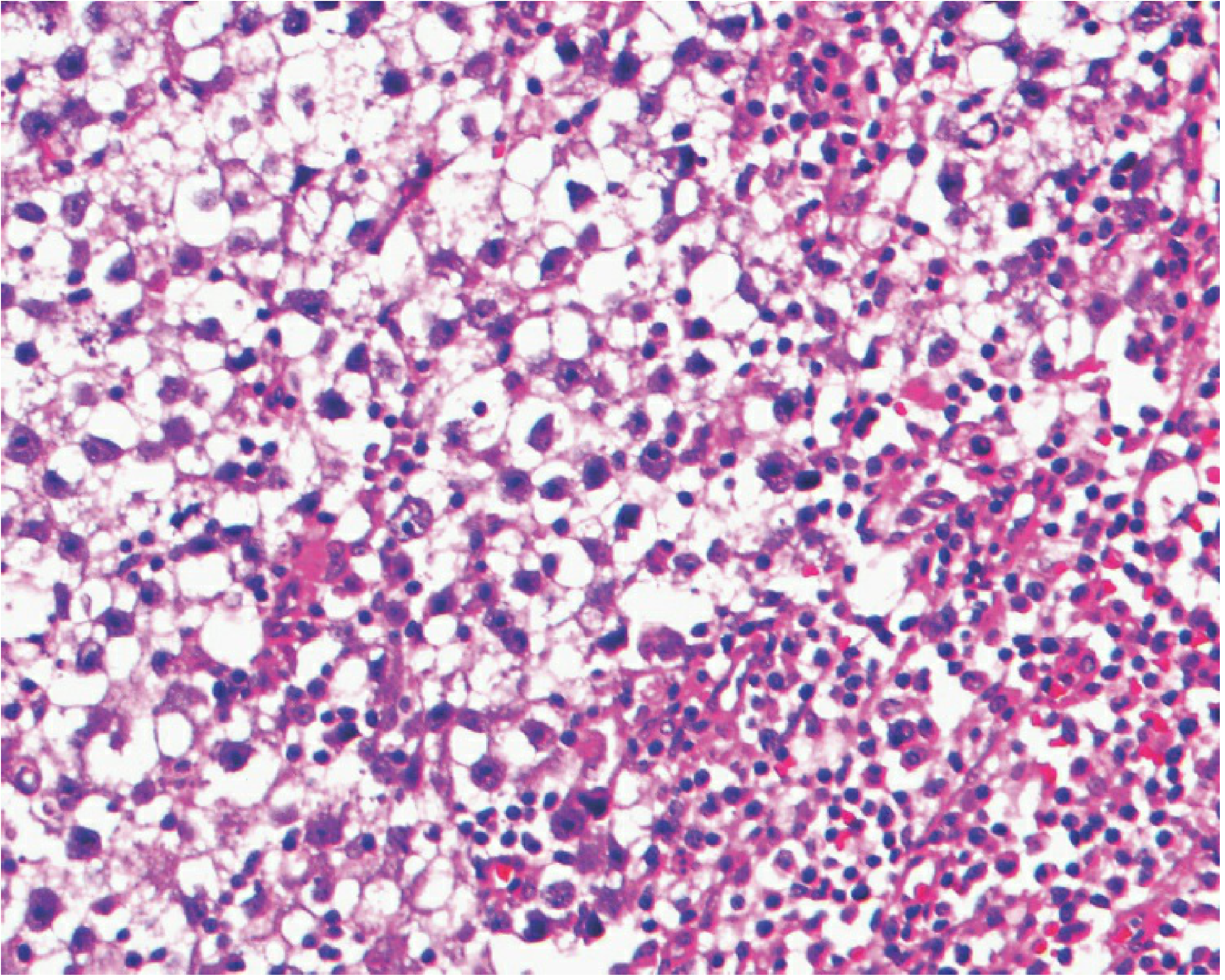
- Large, round/ovoid/polygonal "primitive germ cells"
- Abundant, clear, very-pale-staining cytoplasm
- Large, irregular nuclei with prominent nucleoli
- Numerous mitotic figures
- Cells in lobules and nests separated by fibrous septa
- Septa extensively infiltrated with lymphocytes, plasma cells, epithelioid granulomas with giant cells
- When necrosis is extensive, may mimic tuberculosis
- May contain syncytiotrophoblastic giant cells (→ precocious puberty/virilization; does not alter prognosis)
- Calcifications should prompt search for underlying gonadoblastoma
Labeled Diagram
DYSGERMINOMA - HISTOLOGICAL FEATURES
══════════════════════════════════════
┌──────────────────────────────────────────┐
│ FIBROUS SEPTUM │
│ • = Lymphocytes │
│ [G] = Epithelioid granuloma │
│ PC = Plasma cells │
└──────────────┬───────────────────────────┘
│
┌──────────────▼───────────────────────────┐
│ NEST / LOBULE │
│ │
│ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ │
│ ○ = Large round primitive germ cell: │
│ - Clear/pale cytoplasm │
│ - Large irregular nucleus │
│ - 1-2 PROMINENT NUCLEOLI │
│ - Mitoses frequent │
│ │
│ *ST* = Syncytiotrophoblast (some cases)│
│ [Ca] = Calcifications → gonadoblastoma?│
└──────────────────────────────────────────┘
IHC: PLAP (+), OCT3/4 (+), D2-40 (+), KIT/CD117 (+)
Tumor markers: LDH elevated | hCG: only if ST cells present
AFP: Negative
Behavior and Spread
- Spreads via lymphatics to para-aortic lymph nodes (similar to seminoma)
- Hematogenous metastases occur late
- Exquisitely radiosensitive and chemosensitive (BEP regimen)
- Fertility-sparing surgery appropriate for Stage I
- Prognosis: excellent (5-year survival >90% for localized disease)
QUICK REVISION: TERATOMA vs. DYSGERMINOMA vs. SEMINOMA
| Feature | Teratoma | Dysgerminoma | Seminoma |
|---|---|---|---|
| Germ cell derivation | Pluripotent GC differentiates to somatic lines | Primordial GC (undifferentiated) | Primordial GC (undifferentiated) |
| Gross | Cystic + solid, heterogeneous | Solid, lobulated, tan-gray | Solid, homogeneous, gray-white |
| Microscopy | All 3 germ layers in disorganized arrangement | Large clear cells, fibrous septa, lymphocytes | Same as dysgerminoma |
| Tumor marker | AFP (20-25%) | LDH; hCG if ST cells present | hCG (10%) |
| Spread | Lymphatic + hematogenous (adults) | Lymphatic (para-aortic) | Lymphatic (para-aortic) |
| Radiosensitivity | Resistant | Exquisitely sensitive | Exquisitely sensitive |
Sources consulted:
- Robbins & Kumar Basic Pathology - Chapter 16 (Male Genital System), Table 16.1, Figs. 16.3, 16.4, 16.9
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Chapter 22 (Female Genital Tract), p.937
- Berek & Novak's Gynecology - Chapter 39 (Germ Cell Malignancies), Figs. 39-18, 39-19
This is a shared conversation. Sign in to Orris to start your own chat.